

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Malocclusion affects many people worldwide. Orthodontists traditionally consider restored oral health, function, and aesthetics as the principal therapeutic goals.1 However, improved aesthetics and its positive psychosocial impact are increasingly being accepted as important benefits of treatment.1,2
Occlusal or orthodontic treatment need indices are available to classify the anatomical and aesthetic aspects of malocclusion. The best-known and most-used tools are the Dental Aesthetic Index (DAI) and Index of Orthodontic Treatment Need (IOTN).3,4 However, they do not account for the influence of malocclusion on the patient's quality of life.5 Tools that attempt to assess the oral health-related quality of life (OHRQoL) offer information on the patient's perception of their welfare in relation to a particular oral condition.6
Several authors have employed OHRQoL assessment questionnaires together with normative indices to study the impact of malocclusion on the patient's quality of life.7,8 In the past, OHRQoL research focused on adults with periodontal disease, tooth loss, or inadequate dentures.9 Recently, however, the OHRQoL of children and adolescents has aroused considerable interest,10 to some extent because adolescents usually show great concern about their appearance, which plays an important role in their psychosocial welfare.11,12
The Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ) is a valuable tool that provides information on one aspect of the OHRQoL. This self-rating instrument was designed to assess the psychosocial impact of dental aesthetics in young adults.6 Brazilian, Chinese, and Spanish versions of the PIDAQ have been published recently,13-15 so its global use is increasing.
The aims of the present study were to evaluate the psychosocial impact of malocclusion, determine its relationship with the severity of malocclusion, and assess the influence of gender and social class on this relationship in adolescents.
MATERIALS AND METHODS
Subjects
The study sample was composed of 627 adolescents aged 12 - 15 years in 42 schools chosen randomly from 1,200 subjects of all the schools in Valencia, Spain. The fieldwork was carried out in November and December 2010.
In each of the selected schools, 15 - 20 adolescents underwent intraoral examinations by three examiners, who were calibrated against a gold standard in the use of the IOTN (intraexaminer and interexaminer kappa > 0.85). Adolescents with visible lesions on their anterior teeth due to caries, traumatic injury, or hypoplasia/fluorosis or those who wore orthodontic appliances were excluded.
The study was approved by the Human Research Ethical Committee of the University of Valencia (approval number H1352114553202) and complied with the recommendations of the Declaration of Helsinki. Written informed consent for the intraoral examinations and survey was obtained from the parents.
Data collection
Psychosocial impact of dental aesthetics
The Spanish version of the PIDAQ for adolescents was employed. The PIDAQ, a psychometric instrument containing 23 items, is composed of four subscales, representing four areas, one positive and three negative: aesthetic concern (AC, three items), psychological impact (PI, six items), social impact (SI, eight items), and dental self-confidence (DSC, six items). A five-point Likert scale is used for each item. The response options are as follows: 0 = not at all; 1 = a little; 2 = somewhat; 3 = strongly; and 4 = very strongly.5 Each subscale score can be calculated separately and is obtained by summing the item scores.14 To calculate the total PIDAQ score, the DSC items were re-coded to align them with the other subscales.
Severity of malocclusion
The IOTN was used to determine the severity of malocclusion. This index is composed of 2 parts: the dental health component (DHC) and the aesthetic component (AC).3,15
The IOTN-DHC is assessed by the examiner and classified into five grades according to the therapeutic need: grade 1 = none (normal occlusion); grade 2 = little (minor malocclusion); grade 3 = borderline (moderate malocclusion); grade 4 = great (severe malocclusion); and grade 5 = very great (very severe malocclusion).
The IOTN-AC is assessed by the patient using 10 photographs that show the degrees of malocclusion ranging from the least severe to the most severe. The patient has to identify with one of the photographs. The 10 IOTN-AC grades are combined into three groups: grades 1 - 4, grades 5 - 7, and grades 8 - 10.3
Social class
The UK Registrar-General's Social Class scale was employed. This scale groups the population into the following five categories: I = professionals and higher managerial and technical occupations; II = lower managerial and technical occupations, trade; III = intermediate supervisory and clerical occupations; IVa = skilled manual workers; IVb = partly skilled manual workers; and V = unskilled workers.16 In this study, categories I and II were considered the high social class, category III was considered the middle social class, and the remaining categories were considered the low social class.
Statistical analysis
PASW Statistics version 18.0 (IBM Inc., Armonk, NY, USA) was used for the data analysis. Univariate descriptive statistics were used to calculate the means of the quantitative variables, proportions of the categorical variables, and confidence intervals of both. The means were compared by using Student's t-test and analysis of variance (p < 0.05). Stepwise linear regression models were employed to study the linear relationship between the PIDAQ data as the dependant variable and the IOTN components, gender, and social class as the independent predictive variables.
RESULTS
By gender, 47.8% and 52.2% of the sample were boys and girls, respectively. In terms of social class, 49.3%, 38.7%, and 12.0% belonged to the low, middle, and high social classes, respectively.
The mean total PIDAQ score was 32.2 (95% confidence interval = 31.1 to 33.3). The mean DSC score was 11.3 (10.8 to 11.7), SI score was 6.1 (5.6 to 6.5), PI score was 5.9 (5.6 to 6.3), and AC score was 7.44 (7.2 to 7.7).
In the IOTN-DHC, 54.4% of the adolescents had grades 1 and 2, 27.4% had grade 3, and 18.2% had grades 4 and 5. The IOTN-AC distribution was 90.3% for grades 1 - 4, 6.4% for grades 5 - 7, and 3.3% for grades 8 - 10.
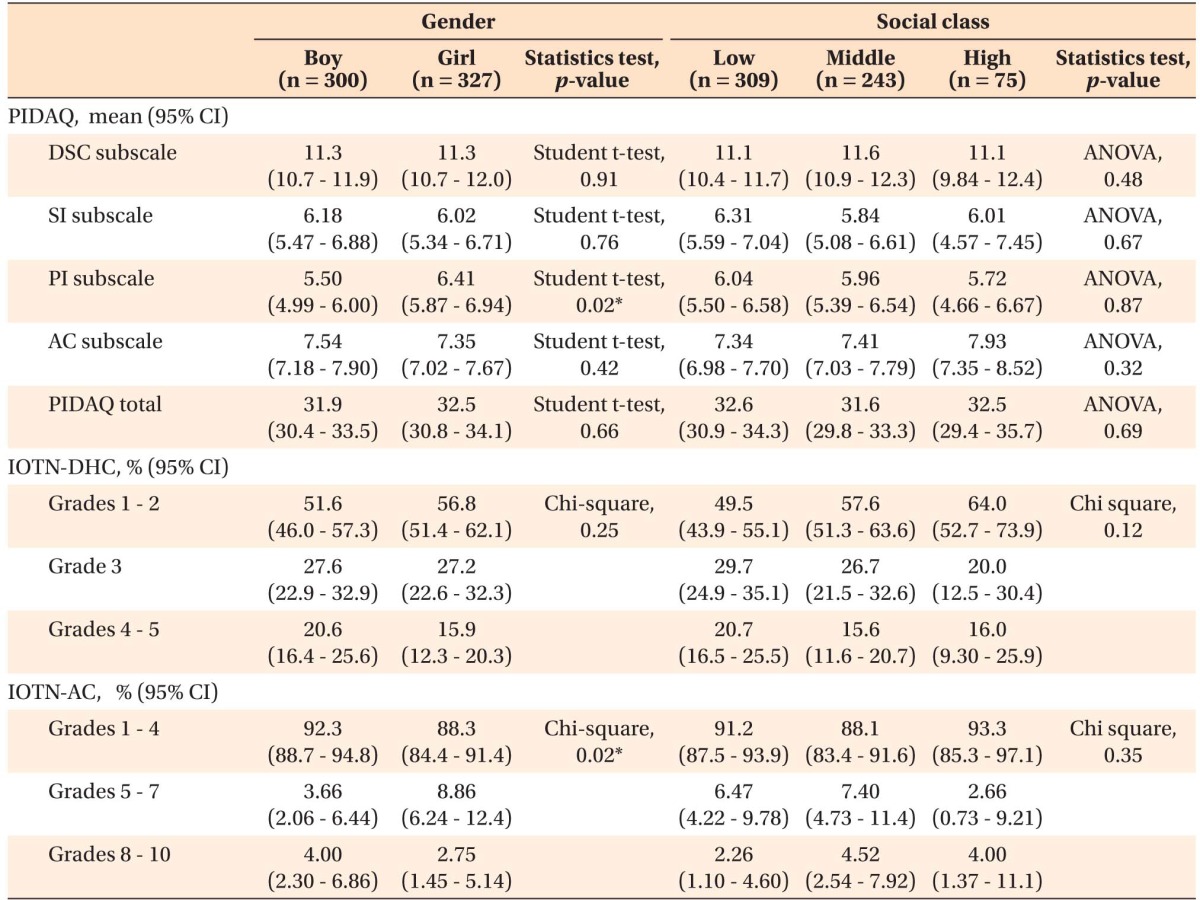
Table 1 shows the relationships of the PIDAQ and IOTN data with gender and social class. The total and subscale PIDAQ scores showed no significant differences by gender, except the PI subscale, where girls had higher scores (p = 0.02). No significant differences by social class were noted. The IOTN-AC presented significant differences by gender, with a greater number of girls having grades between 5 and 10 (p = 0.02).
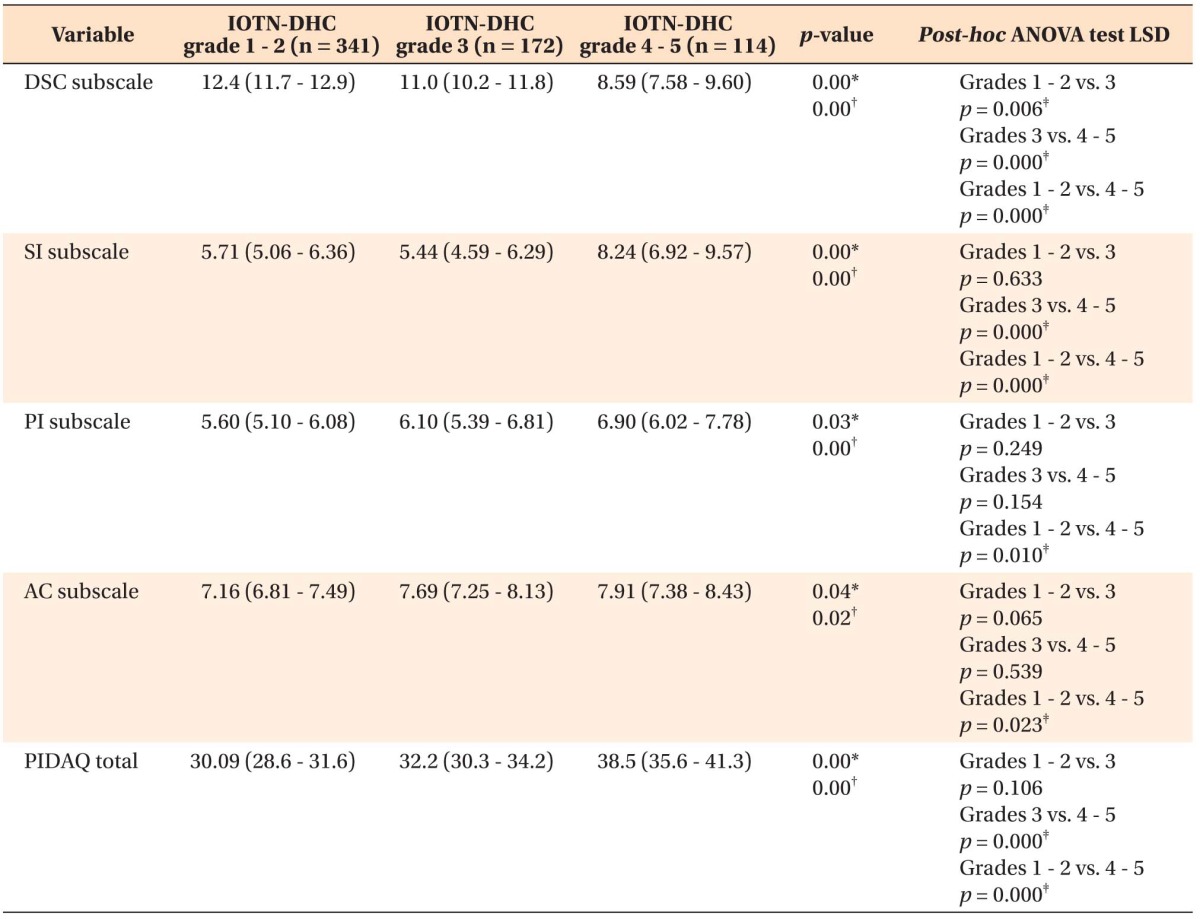
The total PIDAQ score and the SI, PI, and AC scores presented a significant positive linear relationship and the DSC score presented a significant negative linear relationship with the IOTN-DHC grades (Table 2).
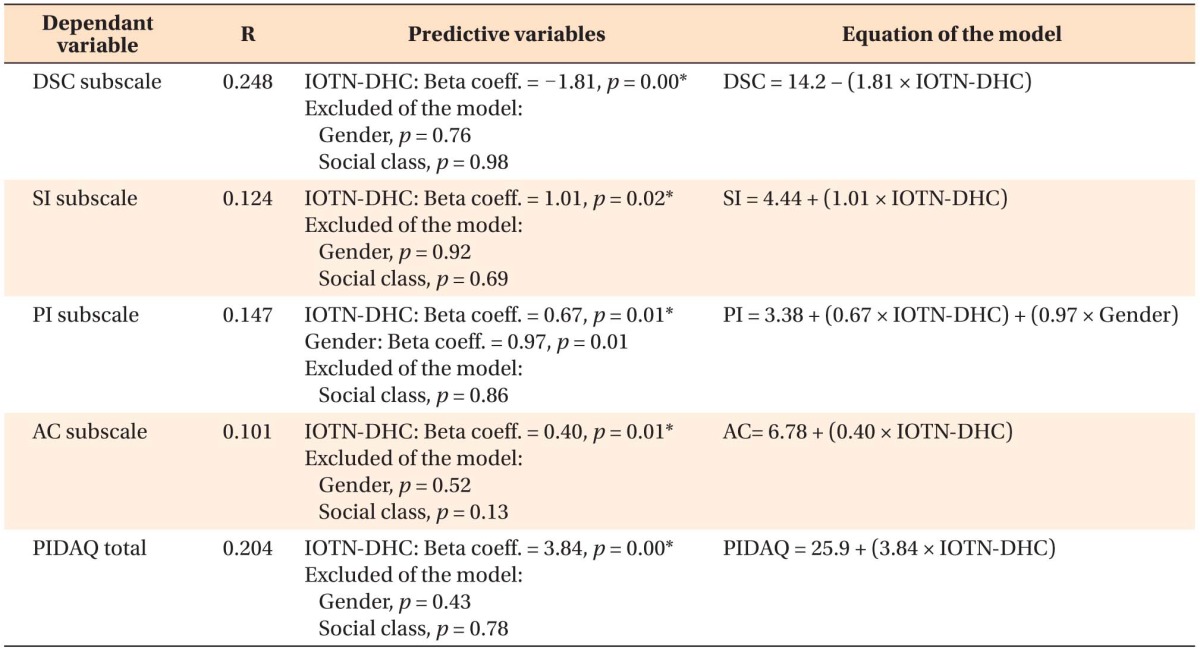
Table 3 shows that the IOTN-DHC was a predictive variable of the total and subscale PIDAQ scores. Neither gender nor social class was an independent predictive variable of the relationship between the PIDAQ scores and the IOTN-DHC grades, except the PI subscale, where gender was a predictive variable in the linear model.
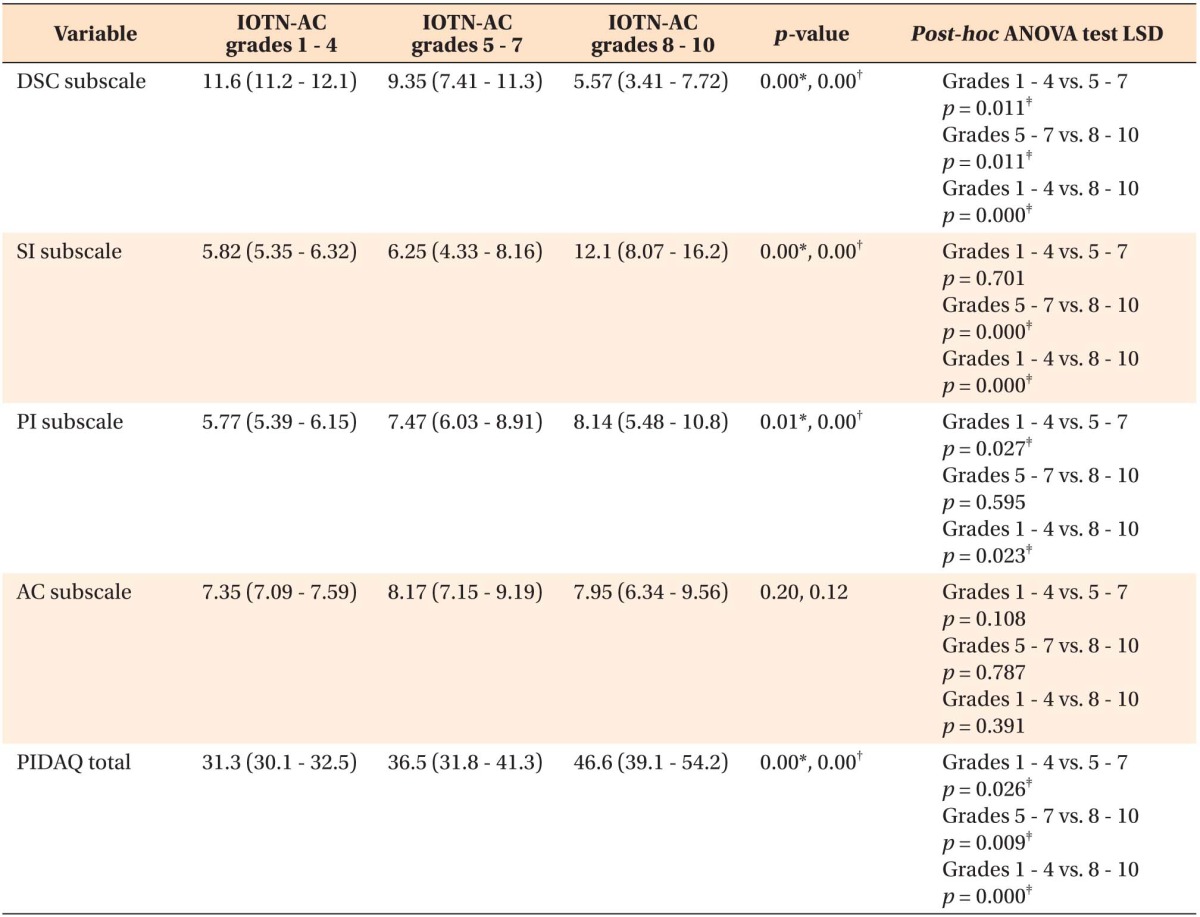
The total PIDAQ and SI and PI scores showed a significant positive linear relationship and the DSC score presented a significant negative linear relationship with the IOTN-AC grades. The PIDAQ-AC scores did not exhibit significant differences in the IOTN-AC grades (Table 4).
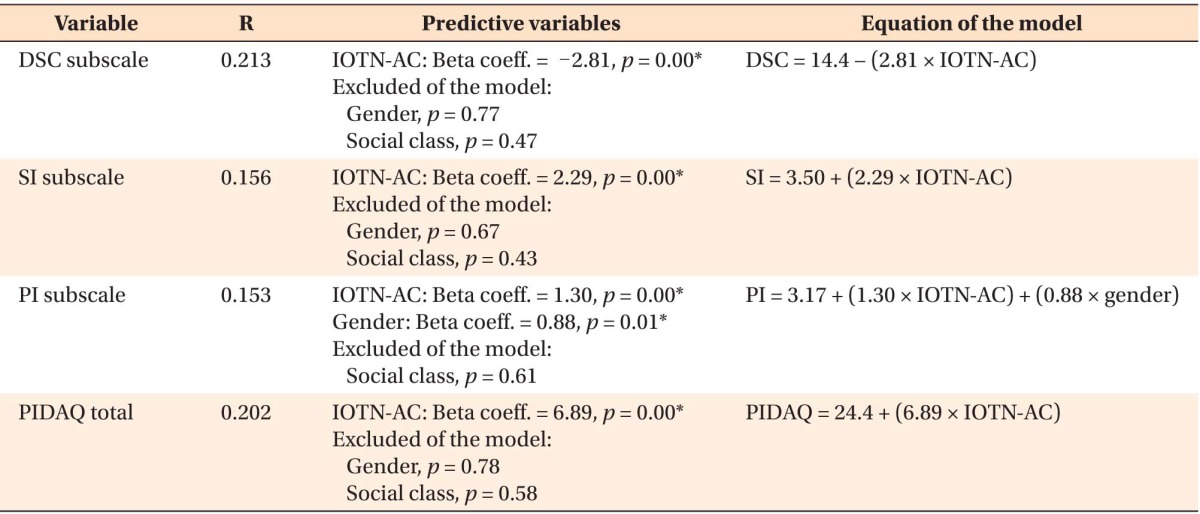
The IOTN-AC was a predictive variable of the total PIDAQ and DSC, SI, and PI scores. Gender appeared as a predictive variable only of the PI scores. A linear relationship between the PIDAQ-AC scores and the IOTN-AC grades could not be established (Table 5).
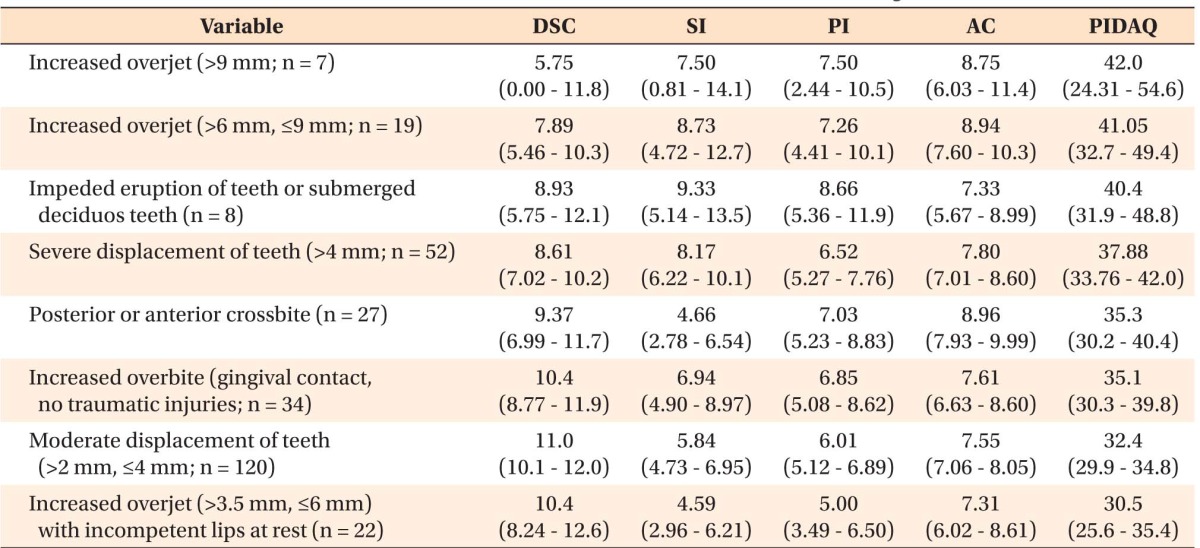
Table 6 shows a descriptive analysis of the main occlusal conditions requiring orthodontic treatment (IOTN-DHC grades 3 - 5) and increasing the PIDAQ scores: increased overjet, impeded tooth eruption or submerged deciduous teeth, tooth displacement, and increased overbite.
DISCUSSION
The present study included a randomized and representative sample, good reliability of the examiners, and a validated questionnaire to measure the psychosocial impact of malocclusion in adolescents. However, considering the age of the subjects, comparisons with other studies should be made cautiously.
Many authors consider it more advisable to analyze the psychosocial impact of dental aesthetics in adults, who are emotionally stable and have a realistic view of dentofacial aesthetics, than in adolescents.17,18 Cooper et al.19 observed that the perception of dental aesthetics changes and even improves with age. Tuominem et al.20 also concluded that the perceived orthodontic treatment need seems to lessen with age even if the patient does not undergo orthodontic treatment.
Several authors agree that the IOTN-DHC measures the severity of malocclusion,21 but the reliability of the IOTN-AC has been questioned.22,23 Indeed, many studies have shown that results differ considerably according to whether the treatment need is measured objectively with the IOTN-DHC or subjectively with the IOTN-AC.22,24,25 Nevertheless, the present study showed a significant linear association between the PIDAQ scores and the grades of both the IOTN components. The PIDAQ-AC was the only subscale that did not show a linear correlation with the IOTN-AC. Although the PIDAQ-DSC showed a linear relationship with the IOTN-DHC, this association was not much stronger than that of the other subscales.
In agreement with other studies,8,17,26 this study showed that the psychosocial impact of dental aesthetics increased with the severity of malocclusion, so the PIDAQ has considerable validity. This finding confirms that malocclusion has a psychosocial impact in adolescents, which can considerably influence their self-confidence and social life.6,27
Increased overjet, tooth displacement, and increased overbite were the occlusal conditions that had a higher psychosocial impact. Dahong et al.28 obtained similar results; they considered that the overjet might induce a protrusive or retrusive profile and further influence the psychology of patients. In this study, only Angle's classification or the incisor classification was used.
Only Sardenberg et al.13 and Lin et al.14 have analyzed the psychosocial impact of malocclusion, but neither study was conducted in adolescents using the PIDAQ. We related the PIDAQ with a normative index (IOTN) that has been used by many authors. Sardenberg et al.13 used the DAI as a normative index, but Lin et al.14 did not use any objective index.
Although some studies have shown a relationship between the aesthetic impact of malocclusion and social class,8 the present study showed no such association, as previously reported.29 Noteworthily, the methods employed to obtain socioeconomic information differ among the relevant studies, so more research should be conducted with this aspect in mind. Other authors such as Doğan et al.30 also concluded that socioeconomic factors are unrelated to the perception of malocclusion.
Gender, however, did affect the psychosocial impact of malocclusion in adolescents. Although it did not influence three PIDAQ subscales (DSC, SI, and AC), it affected the PI subscale. de Oliveira and Sheiham31 also found that the psychosocial impact of malocclusion is significantly greater in women than in men and affects their quality of life. Similarly, the present study showed that the girls' perception of their dental aesthetics was worse than that of the boys. Other studies have also indicated that men tend to be more satisfied with their dental aesthetics.22
We have observed lower punctuation than the Brazilian version on the PIDAQ DSC subscale. The younger sample may explain this difference.
 XML Download
XML Download