

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The increasing number of infants born prematurely and of extremely small premature infants challenges NICU (Neonatal Intensive Care Unit) nurses. Traditionally, care in an NICU focused mainly on the physiologic support of infants (Johnson, 2008). However, as more babies survive, focus has been expanded to include emotional support and developmental care of premature infants (Landry, Smith, & Swank, 2006).
The mother-infant interaction is commonly considered as the most important factor for normal growth and development of a premature infant (Kärtner, Keller, & Yovsi, 2010). Infants' relationship with their parents provides the foundation for the development of self-confidence and security, emotional stability, readiness to learn, social confidence, and the foundation for the development of the self-regulation capacities (Browne & Talmi, 2005). The birth of a premature infant and admission to the NICU disrupts the expected development of interactive skills for both the mother and the infant (Browne & Talmi). Premature infants tend to show behavioral cues which are difficult to understand or they have difficulty in giving signals for interaction. In addition, mothers may have difficulty in initiating and maintaining an interaction with the premature infant, regardless of receptiveness of the infant. For these reasons, mothers of premature infants experience difficulty in beginning and maintaining mother-infant interaction (Jackson, Temestedt, & Schollin, 2003). Lack of this mother-infant interaction leads to adversities in maternal role confidence and adaptation. Many mothers of premature infants fail to understand the response of their children and the delivery of sensitive and reactive care (Jackson et al.). Therefore, it is important to develop nursing interventions to increase mother-premature infant interaction and to improve maternal role confidence (Johnson, 2008). Melynk et al. (2006) also emphasized the importance of understanding infants' behavior and reaction to increase mother-infant interaction. When a competent mother who understands infant cues and responses by establishing good mother-infant interaction, she can also take care of infant's needs and manage health problems with confidence. However, most discharge education programs only provide educational interventions focusing on caring skills and health management of premature infant and do not provide systematic education and information on mother-premature infant interaction (Cho, Jung, & Lee, 1997; Gagliano, 1988; Jackson et al.; Jang, 2005; Johnson; Kwon, & Kwon, 2007; Lagner, 1988; Lederman, Weingarten, & Lederman, 1981; Scherf & Reid, 2006; Song, Park, & Joo, 2007).
Discharge education for the mothers is mainly conducted through booklets or lectures. However, the understanding of written booklets and lectures differs depending on the learner's ability (Gimeno-García, Quinetro, Nicolás-Pérez, Parra-Blanco, & Jiménez-Sosa, 2009). Additionally, the quantity and quality of education content differs depending on the ability of the lecturer when education is conducted by lecture (Gagliano, 1988; Krouse, 2001).
Video education was introduced to solve such problems, and its effect is being verified in the fields of health education (Krouse, 2001). Gagliano (1988) states role modeling through video is the strongest aspect of video education. Considering that mother-infant interaction is a caring behavior including recognition, apprehension, and emotional response (Kärtner et al., 2010; Mercer, 1995), video education can be more effective than written materials. Additionally, video education is appropriate for mothers as they need to have a role model when they care for the children. After a stressful period of having an infant in the NICU, it is important for a mother to learn how to interact with her infant by video, because this program increases maternal role confidence by role modeling (Johnson, 2008).
Thus, the main purpose of this study was done to develop and evaluate discharge education using a video program focusing on mother-infant interaction as well as health management of premature infants.
METHODS
1. Research design
This study was a methodological research study to develop an educational video discharge program for mothers of premature infants, utilizing Jung's (1999) Network-based Instructional System Design (NBISD) model. For program evaluation, pre-experimental study was conducted with mothers of premature infants.
2. Participants
The selection criteria for participants were mothers of infants of gestational age less than 37 weeks, mothers of infants with an appropriate weight for gestational age, while being born over 1000g and under 2500g, mothers who understood the purpose and process of the study and agreed upon volunteering, and mothers of infants expecting discharge in less than a week. Exclusion criteria for participants were mothers who were suffering from a chronic or acute health problem, mothers who would not be taking care of their infants after discharge, mothers of twins, mothers of infants with critical health problems such as neonatal asphyxia, respiratory distress, sepsis, feeding disorder, cerebral hemorrhage III or IV, mothers of infants with congenital malformation, or mothers of infants with hospitalization less than a week.
Twelve mothers of premature infants participated in program operation. However, one mother didn't take part in evaluation because she didn't want to answer questionnaire. Therefore, 11 participants included in evaluation.
3. Development of video discharge education program
This study employed the NBISD model (Jung, 1999) to develop the video discharge education program for mothers of premature infants. The NBISD model comprises the 5 phases; analysis, design, development, operating, and evaluation. The development process of each phase is summarized in Figure 1.
1) Analysis
Analysis phase includes analysis of content, technique and environment. For content analysis, 263 questions and concerns written by mothers of premature infants who were members of an internet community for parents of premature infant were used. Also, 11 sources of Korean and international literature were reviewed to analyze mothers' need for discharge teaching. For technique and environment analysis, a scenario writer, video production team, and studio for recording were procured as well as a model infant and necessary equipment such as video cameras and microphones.
(1) Content analysis of parental concerns of premature infants
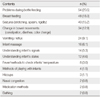
The most frequent concerns of parents before and up to a month after discharge as presented by the internet community (11,571 members in Oct. 2010) were related to basic infant care skills including problems during bottle feeding, breastfeeding, and bathing (39.6%), health problems and management such as seizure, change in bowel movements, vomiting or reflux, fever, methods for checking infants temperature, hiccups, nasal congestion, and medication methods (42.9%), and understanding infant's characteristics and interaction including infant massage, understanding infant's signals and state, and methods of playing with infants (17.5%) (Table 1).
(2) Content analysis of the existing discharge education programs
In the previous discharge education programs, the most frequent topics were on general care of infants such as, crying and infant colic, infant's behavior, and health management for seizures, cyanosis, vomiting, as well as determining the regularity of stool changes (Cho et al., 1997; Jang, 2005; Lagner, 1988; Scherf & Reid, 2006). On health management, the educational needs of parents of premature infants was identified as taking care of infants, their respiratory pattern, management during seizures, identifying abnormal symptoms, and preventing infection. Special concerns on care of premature infants such as oxygen therapy and fistula care were educational concerns in several studies (Choi & Kwon, 2000; Jang; Kwon, & Kwon, 2007; Lee et al., 2010; Lee & Kim, 2008; Song et al., 2007). In addition understanding infant's crying and ways to sooth, methods of playing with infants and improving mother-infant interaction have been areas where the need for discharge education has been identified (Cho et al.; Choi & Kwon; Song et al.). Therefore, the major educational needs and content of discharge education for mothers of premature infants can be categorized as caring skills, health problems and management, growth and development, and understanding premature infants' signs and states.
2) Design
According to Kolb's (1984) experiential learning model, a 4 step process; concrete experience, reflective observation, abstract conceptualization, and active experimentation; an information, interaction, motivation, and evaluation design was used.
For the informational design, the program's educational content included the video, narration, and captions. Most content was delivered through narration, and the video was edited according to the narration to support the content. Subtitles were for emphasis.
For the interaction design, a counseling and opinion sharing time were provided after viewing the video for interaction between the learners to enhance their understanding of the content. Additionally, contacts with the educator were provided for later questioning related to the content.
For the motivation design, the purpose of education was clearly delivered during the introduction, and the content was presented in a storytelling method following the daily timeline of a premature infant. To increase motivation for learning, a premature infant was used as the infant model, and the narration was read in a story telling method. The content was presented in two sessions to prevent boredom. According to the content and atmosphere, appropriate sound and symbols were inserted, and narration was read to enhance the learner's concentration. Additionally, a time to share the learner's opinion was provided for the learners to understand with flexibility according to their own personal situations.
Lastly, in developing the evaluation design, a self-evaluation based on Mercer's (1995) theory was conducted which included categories related to mother-infant interaction, maternal sensitivity, and maternal role confidence a month after the education.
3) Development
The process of developing the educational medium and content included the steps of development of themes, content, scenario, video, and model operating and evaluation.
(1) Development of themes for the program
As a result of the analysis of educational needs, the most frequently discussed educational content was identified as basic caring, health problems and management, and understanding infant's characteristics and interaction. Mercer (1995) has suggested that factors which have an effect on mother-infant interaction and becoming a mother are the infant's characteristics (signal delivery ability, sensitivity), and health. Therefore, the focus was on mother-premature infant interaction and premature infant health management in this study. The results of analysis of previous discharge education programs for enhancing mother-premature infant interaction were included (Kwon & Kwon, 2007; Lee & Kim, 2008; Shin & Lee, 2003) in theme development.
As a result of this process, sub-themes such as understanding infant's signals and states, playing with infants, and premature infant massage were added (Melynk et al., 2006) (Table 2). The selected sub-themes of the program and specific content were validated by the expert group for scenario development and 6 mothers of premature infants.
(2) Development of content for the program
Content for the program was from the analysis of previous booklets and lectures (Kwon & Kwon, 2007; Lee & Kim, 2008; Shin & Lee, 2003). Since all content cannot be dealt with in one program, hierarchy of the content was defined. Then, such content was reviewed twice by 4 nurse educators in child health nursing.
On consultation with the 4 nurse educators in child health nursing and 1 NICU head nurse, only content directly related with the subthemes was included in the program. In addition to the expert group, 5 NICU nurses with more than 5 years experience reviewed the content for validity. Through this process, the content was clarified and accuracy was confirmed.
The content validity was tested with an expert group of 1 neonatologist, 5 NICU nurses with more than 5 years of experience, and 24 pediatric nurses enrolled in advanced nurse practitioner programs. Examination showed that all 38 items a CVI higher than 0.87. Therefore, 38 options in 10 categories were all validated with a CVI of 0.99 (Table 2).
(3) Development of the scenario
An expert group of 4 nurse educators in child health nursing, 1 NICU head nurse, and a scenario writer with more than 5 years experience participated in the scenario development. Initial scenario was developed based on diary from a mother of premature infant, previous discharge education program, and a book on caring of premature infants written by nurse educators and a nurse at the NICU. The evaluation sessions were conducted three times, and each time modifications were made. The narration part was modified by the scenario writer twice to ensure a comfortable language was presented. The researcher, the scenario writer, and a professional voice actor developed the final scenario after the review.
(4) Video production
Infant model was recruited at an outpatient pediatric clinic with help from NICU head nurse. The model was a male infant with a gestational age of 35 weeks and 2 days, and birth weight of 2.1kg. His age at the production time was 39 weeks 24 days and weight was 2.8kg and he had no health problems. Despite the premature birth, the model reacted appropriately to the stimulation, which was effective in showing infants' signals or states. The purpose of the video and confidentiality were explained to the mother before she signed the permission. To record images of premature infants for the beginning and end of the video, the researcher and the two recorders visited the NICU and obtained the permission to video the infants.
The video production team included the researcher, 2 video recorders who were experienced in professional education videos, 2 video editors, and a professional voice actor. Before recording, 2 meetings were held between the researcher and recorders to construct continuity for each part of the education content. Recording equipments were prepared by researcher, while a 6mm camera and two microphones were rented for special recording. In preparation for the first recording, the recording team visited the infant model's house, checking the house structure for recording angles and lighting. Since strong lighting may cause discomfort for the infant, all artificial lighting was excluded and all recording was done during the day time. Three rehearsals were conducted a day before to decide the order of the recording according to the infant's daily life. To prepare for the second recording, recorders visited a hospital to examine the NICU structure and infants.
The recording took a total of 7 hours and was edited by 2 professional video editors. The editing took a week. The result was a video of 28 minutes and 42 second in total length; the first part on mother-infant interaction was 19 minutes and 27 seconds, and the second part on premature infant's health management was 9 minutes and 15 seconds.
Evaluation through model operation was done twice. The first edition was evaluated by 2 producers of broadcasting stations to determine the quality of video. The second edition was evaluated 24 pediatric nurses enrolled in advanced nurse practitioner program, and 6 mothers of premature infants for the quality of the video and appropriateness of content.
With the exception of degree of difficulty, all categories of educational content of the video were evaluated as inappropriate or very inappropriate. The main concerns were length (too long), presentation (boring), and the voice of narrator (not pleasant), all of which made it hard to concentrate. Following this evaluation, the video was modified by adding captions of the infant model's birth weight, gestational age, current weight, current age, so the viewers could relate to premature infants. Additionally, in the category of mother-infant interaction, captions were added to emphasize the importance and characteristics of infant signs and states.
The title of the final video was "Help my baby grow well", with a total of 21 minutes and 32 seconds. The first section was the part on understanding a premature infant's characteristics and enhancing mother-infant interaction and lasts 14 minutes and 39 seconds. The second section was the part on providing information for premature infant's health management and lasts 6minutes and 53 seconds. The video was made in the form of a DVD and a CD for user friendly.
4) Operation
The completed video program was presented to 12 mothers of premature infants who were scheduled to be discharged from a hospital located in Incheon, South Korea. These 12 mothers of premature infants participated in the actual use of the discharge education video. The mothers viewed the video three times, and after viewing the video, they had a question and answer session and a time for sharing opinions. A week before discharge is the discharge preparation period, which is an appropriate time for teaching (Lee et al., 2010). Kwon and Kwon (2007) have suggested that education periods need at least two buffering periods based on the retention curve of human's memory. Therefore, the program was conducted three times; 7, 4, and 1 day before discharge.
The program was conducted with small groups of 2 to 3 mothers, and the program started when mothers finished their visit to the NICU at 1:00 P.M., and took about 40 to 60 minutes. The first session took an additional 10 minutes to develop rapport and present a short introduction.
4. Measurements and data analysis
Measurements' validity and reliability were verified in original studies. To secure content validity of the measurements in this study, all contents of measurements reviewed by advisory team. Self-administered questionnaire and interview were conducted to assess the quality of video, appropriateness of the content and the method, and finally the effectiveness of the program.
1) Appropriateness of teaching method and content of the program
To evaluate of the appropriateness of teaching method and the content, Jeong's (2000) method was used with some modification. The tool consists with 17 items on a 5-point Likert scale of "Strongly agree" to "Strongly disagree." The scores range from a minimum of 17 to a maximum of 85; a higher score represents more adequacy.
2) Quality of video
To evaluate the quality of the video, Park's (2001) tool was used with minor revision. It includes 6 items, having a 5-point Likert scale of "Strongly agree" to "Strongly disagree." The scores range from a minimum of 6 to a maximum of 30, and a higher score represents a higher quality.
3) The self-evaluation program effects on improvement of mother-infant interaction
For self-evaluation of improvement in the mother-infant interaction, Hwang's (2003) measurement tool was used with some modification. The questionnaire has 9 items with answers from "Strongly disagree" to "Strongly agree." The scores range is a minimum of 9 to a maximum of 36; a higher score represents a more beneficial mother-infant interaction.
4) The effects of the self-evaluation program on improvement in maternal sensitivity
Han's (2002) questionnaire for self evaluation was modified to measure the effect of maternal sensitivity enhancement. The questionnaire includes 36 questions with answers ranging from "Strongly agree" to "Strongly disagree." The score is from a minimum of 36 to a maximum 180 points; a higher score represents a positive effect of increasing maternal sensitivity.
5) The effects of the self-evaluation program on improvement in maternal role confidence
Lee's (1992) translation of the postpartum self-evaluation questionnaire by Lederman et al. (1981) was used to measure of maternal role adaption. The focus of this tool is on cognitive and emotional factors, and questions were modified according to the self-evaluation of improvement of maternal role confidence. The questionnaire includes 14 questions with an answer range from "Strongly disagree" to "Strongly agree". The score range is from 14 to 56 points; A higher score represents more benefit for increasing maternal confidence.
5. Data collection procedure
The program was developed from October 2010 to January 2011. For program operation and evaluation, participants were recruited from among mothers of premature infants who were admitted between March and May 2011 to an NICU located in Incheon. Self-evaluation of the program effects in aspects of improvement of mother-infant interaction, maternal sensitivity, and maternal role confidence was conducted a month after discharge. Completion of questionnaire and interview was individually conducted at pediatric outpatient clinic.
6. Statistical analysis
For data analysis, SPSS 18.0 for Window was used. General characteristics of participants and questionnaire evaluation were analyzed using descriptive statistics. The adequacy of the discharge program was evaluated using CVI.
7. Ethical consideration
Permission to undertake this study was obtained from the Institute Review Board of Yonsei University, College of Nursing (IRB 2010-1036). Informed consent was obtained from each participant either verbally or in written form from mothers who agreed to participate in the study. The mothers were informed of the purpose of the research prior to the beginning of the study and were assured of their right to refuse to participate or to withdraw from the study at any stage.
RESULTS
1. General characteristics of participants
The participants in the evaluation of the discharge education video were mothers of 11 premature infants (Table 3).
2. Evaluation of video discharge education program
The program was evaluated by self-administered questionnaires which were developed by the researcher and semi-structured interview method. Eleven questionnaires and interviews were included.
Evaluation of the video quality, appropriateness as a teaching method, and content were done right after the discharge education. Additionally, self-evaluation of the effects of the program related to improvement of mother-infant interaction, maternal sensitivity, and maternal role confidence was conducted a month after discharge. The evaluation took about 30 minutes to an hour, and counseling was done if any participant requested it.
1) Appropriateness of teaching method and content of the program
The average score was 73.64 points, and scores ranged from 66 to 85. The 8 questions about the teaching method had an average of 4.42 points on a 5-point Likert scale, while the 9 questions related to content had an average 4.25 (Table 4).
Almost all participants evaluated the video as easier to understand than booklets or lectures. Also, all participants answered that the education content was easier to apply in actual care than education from books or lectures. All participants stated that the program clearly meets the education purpose, and were satisfied with the information provided. All participants stated that they would recommend the video to other mothers because the video has useful information for the first time mothers and because the program increases confidence by showing how easy it is to care for the premature infants. As information in this format was not available before, participants reported that the information was useful overall not only for mothers of premature infant but also for first time mothers, as it includes information on infants' characteristics and conditions, which are interest of all mothers.
2) Quality of video
All participants gave positive evaluation on content difficulty, language, video quality and audio quality. However, 8 mothers reported that the video length was somewhat long, and especially learning the two parts at once was difficult. It was suggested that two separate sessions would better to hold participants' attention (Table 4).
3) The effects of the program
The participants evaluated the effects of the program on their infant interaction, maternal sensitivity, and maternal role confidence.
The mean score on the effects toward the mother-infant interaction was 31.45 points, with a range from 23.00 points to 36.00 points (Table 4). During the interview, the mothers stated that they did not realize the importance of mother-infant interaction until the video education. They said that they spent more time talking to their infants and providing touch and eye contact.
The mean score on the effects for maternal sensitivity was 137.00 points, with a range from 119.00 points to 179.00 points (Table 4). The participants thought the video helped them to understand infant signs and it was much better than previous education media. Many mothers thought that infants' crying meant they were hungry. The mean score on effects for maternal role confidence was 39.71 points, with a range from 33.00 to 52.00 points (Table 4).
DISCUSSION
Mother of premature infants experience more difficulties with interaction than mothers of full term infants (Melynk et al., 2006). Therefore, an intervention is required to increase mother-infant interaction. However, the majority of existing education programs for mothers of premature infants focused only on basic caring skills and health management.
Based on the analysis of questions and concerns of mothers of premature infants, the mothers wanted education not only on skills in caring for their infants, but also on mother-infant interaction related issues such as understanding the infant's signals and states. According to Mercer's (1995) theory, mothers and infants respond to each other according to their characteristics, and such responses become the basis of becoming a mother and of the growth and development of infants. Thus, promoting the mother-infant interaction is imperative for the development of mothers and infants, as well as for their well-being (Johnson, 2008). Especially, once a negative formation of mother-infant interaction starts, it is difficult to modify such patterns and maintain a healthy mother-infant interaction (Johnson). Therefore, the initial mother-infant interaction is important, and nursing interventions before discharge are emphasized (Johnson). In this context, mothers of premature infants who evaluated the education program concluded that the program was beneficial to them in caring for their premature infants as mother-infant interaction had not been a topic which was systematically presented to them.
According to Melynk et al. (2006), the education content on premature infants' appearance and behavior, methods of increasing mother-infant interaction, and satisfying infant demands greatly affected maternal functional outcomes and parental role confidence such as the mother's quality of interaction with infants, overall appropriateness of interaction with infants, and sensitivity to needs of infants. Education related to premature infant behavior increased the level of knowledge of behavioral cues from the premature infant which enhanced the mother' s maternal role confidence (Maquire, Bruil, Wit, & Walther, 2007). Browne and Talmi (2005) noted that education related to infant reflex, attention, motor skill, and sleep wake states enhances the level of contingent and sensitive interaction between mother and infants. Such result can be deducted from Mercer's (1995) theory as well. Therefore, when considering Mercer's theory and previous study results, this program positively affects the mothers of premature infants in the mother-infant interaction, maternal sensitivity, and maternal role confidence.
The appropriateness and effectiveness of the teaching method was evaluated by a group of content experts, professional broadcasting producers, pediatric nurses enrolled in advanced nurse practitioner program, and mothers of premature infants. Pediatric nurses and mothers of premature infants responded that predominant features of this program were the focus on the premature infants' emotional and social aspects and on the use of a video as educational media. They recommended this program as also being helpful to mothers of full-term infants, because there was no education program focusing on mother-infant interaction.
The education program using a video media has rarely been used in previous discharge education programs. The reason for using the video is its efficiency, effect of memory improvement, and most importantly, the effect of video role modeling. Mothers of premature infants who participated in the evaluation process stated that the video program was more beneficial than previous media in terms of concentration, recollection of memory, understanding content, and practical application.
Gagliano (1988) claims that video modeling reduces anxiety, increases the knowledge level, correspondence skills, and cooperation of learners. Additionally, the video modeling increases not only emotional responses and education effects, but also compliance (Krouse, 2001). These strengths of video modeling directly affect and enhance the factors of the micro system introduced by Mercer's (1995) theory. Additionally, video modeling which displays appropriate behaviors and attitudes enhances the acquirement of skills, reinforces maternal role adaptation, and the process of becoming a mother by role modeling and role rehearsal (Gagliano). In addition, using a video in education results in increases in short term knowledge and compliance compared to other media such as booklets or lecturing (Gagliano). Thus, video education is an efficient teaching method for mothers of premature infants who need to learn practical and detailed caring skills and have responsibility for parenting of premature infants. Also, as people today are used to media that is viewed; video media is a comfortable method of education for today's mothers, and can provide standardized education which is unaffected by educator's preparations level or individual factors (Gagliano). Also it can be used from admission of premature infants because early mother-infant interaction is recommended and recently discharge education is started with hospitalization (Melynk et al., 2006). Because video education is available without an instructor, fixed time or place (Gagliano), this program can be operated wherever mothers want, their home, lobby of NICU, and so on. Therefore, every mother can be educated fully according to their learning ability.
One of the limitations of the program is that the infant model's age is closed to full-term since it was difficult to have a premature infant as a model. The captions were used to identify the characteristics of premature infants so mothers could relate to their babies. Suggestion is made to evaluate the program in different clinical settings. Also, to approve results of the study, a randomized controlled study should be conducted.
CONCLUSION
The results of the study show that the mother-premature infant relationship, such as mother-premature infant interaction, maternal sensitivity, and maternal role confidence is an essential education area in the development of becoming a mother. Also, video is appropriate media for education on mother-infant interaction. Because there is limited education focusing on mother-interaction, it is strongly recommended that this video discharge program be used in actual clinical settings including NICU and nurseries.
Also, videos have an advantage in economics with no limitation of time and place, improved modeling effects, short term memory, and compliance. Therefore, compared to written material or lectures, video education is a more appropriate media for mothers with premature infants who must care for their infants directly.
Finally, it is suggested that further development of education programs with various issues for mothers of premature infants should be done. Cooperation among multidisciplinary professional groups to develop standardized discharge education is necessary in the development process.




 XML Download
XML Download