

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
The use of levetiracetam as the first-choice antiepileptic drug is increasing.12 Levetiracetam seems to be an attractive option for autoimmune encephalitis because it can be administered rapidly via the intravenous route, has no significant drug–drug interactions, and shows a low rate of severe adverse reactions.3 However, levetiracetam often has serious psychiatric side effects, and they are sometimes confused with limbic symptoms or postictal psychosis.4 We report a case of psychiatric side effects of levetiracetam in a patient with anti-leucine-rich glioma inactivated 1 (LGI1) encephalitis, which was observed as mimicking the disease and gave the impression of a relapse.
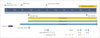
A 59-year-old man visited the department of neurology due to memory impairment (Fig. 1). His initial symptoms were odd sensations, which progressed to retrograde amnesia within 1 week. Cerebrospinal-fluid parameters were within the normal ranges (1 white blood cell/mL and 36.5 mg/dL protein), and brain T2-weighted magnetic resonance imaging revealed a high signal intensity in the left hippocampus. The patient was initially misdiagnosed as having viral encephalitis, for which he received acyclovir for 2 weeks. However, the treatment did not improve his confusion or memory impairment. A left facial muscle twitch subsequently developed, for which administration of oxcarbazepine at 450 mg b.i.d. orally had no effect. After 1 month he was finally diagnosed with anti-LGI1 encephalitis. Along with additional antiepileptics (levetiracetam 1,000 mg b.i.d. orally and valproic acid 600 mg b.i.d. orally), the patient received first-line immune therapy (500-mg methylprednisolone for 3 days, 0.4 g/kg intravenous immunoglobulin (IVIG) for 5 days, and IVIG boosting at 0.4 g/kg for 1 day) and second-line immune therapy (four cycles of 375 mg/m2 rituximab and four cycles of 8 mg/kg tocilizumab).
His memory impairment and confusion had partially improved at 6 months after the diagnosis of anti-LGI1 encephalitis. However, the patient and his family complained of aggravated psychiatric symptoms: he showed agitation, irritability, and aggressive behavior. He easily became angry during conversations and continuously tried to leave home, becoming violent when his family stopped him. Symptomatic management with antipsychotic medication (quetiapine and olanzapine) was not successful. We initially suspected the psychiatric symptoms to be a sequela or relapse of the anti-LGI1 encephalitis, and so we tried additional immune therapies (IVIG boosting at 0.4 g/kg for 3 days twice, two cycles of 375 mg/m2 rituximab, and 8 mg/kg tocilizumab). However, the anti-LGI1 antibody test produced a negative result for serum, and his mood-related problems became worse. We suspected that the psychiatric symptoms were related to levetiracetam and so stopped the medication; 2 days later his psychiatric symptoms showed dramatic improvements. The patient exhibited no recurrence of any psychiatric symptoms after the discontinuation of levetiracetam.
Psychiatric symptoms are among the most serious problems in patients with anti-LGI1 encephalitis as observed both by the patients themselves and by their families in clinical settings. According to our clinical registry, more than half of patients with anti-LGI1 encephalitis show at least one mood-related symptom. Moreover, the development of new psychiatric symptoms in patients with autoimmune encephalitis is critical, in that clinicians often consider this to indicate treatment failure or disease relapse.
The psychiatric side effects of levetiracetam may therefore confuse clinicians about whether they should proceed with the next step of immune therapy for patients with autoimmune encephalitis. Nine of the 17 patients with anti-LGI1 encephalitis in our clinical registry were prescribed levetiracetam to control their seizures. Eight of these patients experienced at least one psychiatric symptom during the course of the encephalitis. It was not possible to distinguish the patient with psychiatric side effects of levetiracetam described in this case report from these eight patients. The psychiatric side effects appeared unpredictably at 6 months after the first use of levetiracetam. This situation resulted in it taking 2 months before the correct diagnosis was confirmed and the patient receiving redundant immune therapies.
In conclusion, caution is required when selecting levetiracetam to control seizures in patients with anti-LGI1 encephalitis. Clinicians should be vigilant and watch for psychiatric side effects of levetiracetam when patients develop new psychiatric symptoms during the course of the treatment.
 XML Download
XML Download