

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The effectiveness of endovascular revascularization for stroke patients with acute large-vessel occlusion in the anterior circulation has been clearly established in several recent randomized controlled trials.12345 However, recent increases in life expectancy mean that older stroke patients possibly constitute the population with the highest stroke incidence6 but are excluded from some of these landmark trials; this is probably due to the prognosis for this age group being expected to remain poor even after reperfusion. The rate of favorable functional outcome in older patients who undergo endovascular therapy (EVT) reportedly varies widely, from 0 to 28%, which might be at least partially due to the application of diverse patient selection criteria in previous cohort studies.7891011121314
Reperfusion is futile in almost 50% of older stroke patients; that is, the 3-month modified Rankin Scale (mRS) score remains ≥3 despite successful reperfusion, with this percentage being almost double that for younger patients.15 This may be partly attributed to the higher incidence of comorbidities and lower restorative ability of the brain in such patients, which results in poor functional recovery.16 It may therefore be necessary to define stricter inclusion criteria for EVT for older stroke patients. The low restorative ability of the brain in older patients might imply that the threshold of baseline ischemia for recovery–which is one of the most-reliable surrogate markers of stroke outcome–171819 could be lower than that in their younger counterparts.
We hypothesized that the threshold for baseline ischemia as a predictor of good functional outcome is lower in older patients. To test this hypothesis, which was not been explored previously in the clinical literature, we examined the relationship between the degree of baseline ischemia and clinical outcome according to age.
METHODS
Between May 2006 and December 2014, patients were retrospectively selected from a prospectively maintained acute stroke registry at our institution. The criteria for inclusion in this study were as follows: 1) EVT performed due to acute anterior circulation stroke with proximal vessel occlusion [T- or L-type internal carotid artery (ICA), M1 segment of the middle cerebral artery (MCA), or ICA/M1 tandem occlusion], 2) arrival at our emergency center within 6 hours of symptom onset, 3) evaluable pretreatment diffusion-weighted imaging (DWI), and 4) prestroke mRS score of 0–2. The study protocol was approved by the local Institutional Review Board.
Eligible patients underwent transfemoral cerebral angiography with contrast agent injected into both carotid arteries and the dominant vertebral artery during the late venous phase under local or general anesthesia, in order to define the angioarchitecture of the occluded vessel and assess the extent of collateral flow from all possible sources. If the treatable ICA or MCA occlusion persisted, EVT was initiated. Treatment strategies were selected on the basis of therapies available at the time of angiography, and they included intra-arterial thrombolytic infusion (urokinase or recombinant tissue plasminogen activator), mechanical clot disruption, mechanical thrombectomy with forced arterial suction thrombectomy or Solitaire thrombectomy, placement of rescue intra- or extracranial stenting, or a combination of these approaches.202122 The angiographic collateral flow grade, as observed during pretreatment angiography, was evaluated according to the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology Collateral Flow Grading System. This angiographic scale assigns patients to grades 0 to 4 according to the completeness and rapidity of retrograde collateral filling.23 The reperfusion status was measured using the Thrombolysis in Cerebral Infarction (TICI) scale.23
Information on demographic and clinical characteristics, medical history, admission blood pressure, and blood glucose were collected at baseline. The onset of stroke was defined as the time when the patient was last observed to be without any abnormal signs or symptoms. Before the initiation of treatment, baseline stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS). All patients underwent a CT or MRI scan at 24–48 hours after the initiation of treatment. If evidence of hemorrhage was detected, the subtype of the stroke was classified as hemorrhagic infarction, parenchymal hematoma, subarachnoid hemorrhage, intraventricular hemorrhage, or mixed.24 Symptomatic intracranial hemorrhage was defined as any type of hemorrhage associated with an increase in the NIHSS score of 4 or more within 24 hours of treatment.25 The DWI findings at baseline were assessed using the Alberta Stroke Program Early CT Score (ASPECTS) for DWI by two raters (Y.W.K. and D.H.K.),26 with any disagreements resolved by consensus. The volume of the lesion on DWI was calculated using open-source image analysis software (OsiriX, Pixmeo, Geneva, Switzerland) by an experienced neurologist (Y.W.K.) who was blinded to the clinical status of the patient. Recovery of neurological function was assessed at 3 months using the mRS, with a favorable outcome being defined by an mRS score of 2 or less.2527
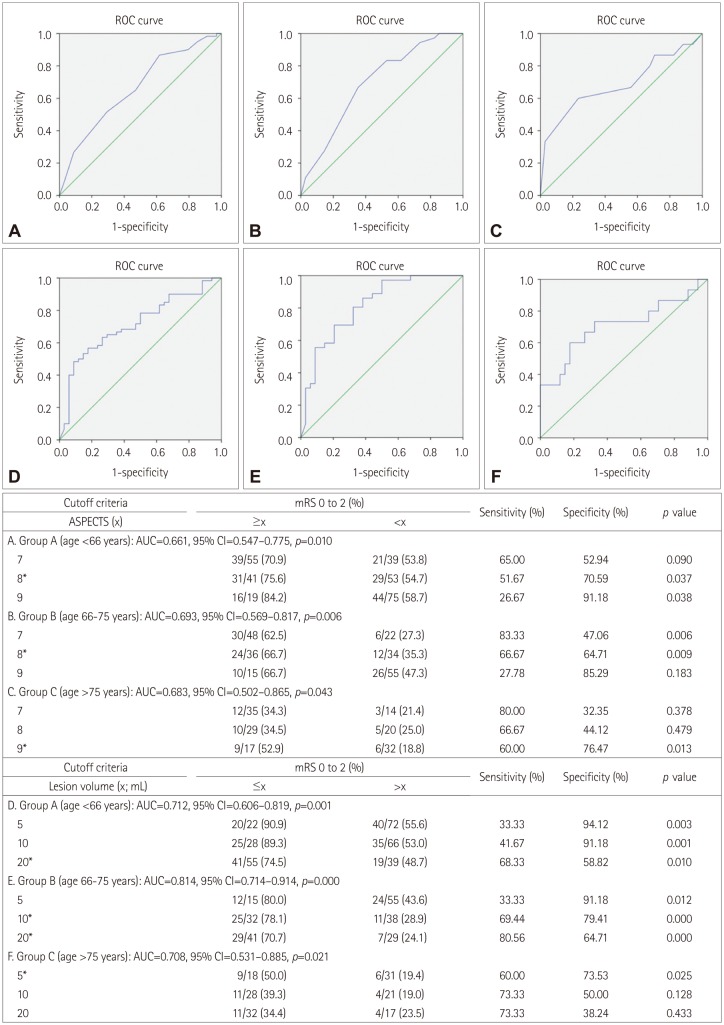
Statistical analysis was performed using the SPSS statistical package (version 20.0, SPSS Inc., Chicago, IL, USA). The statistical significance of intergroup differences was assessed using the chi-square test for categorical variables, one-way ANOVA for continuous variables, and the Kruskal-Wallis test for ordinal variables and continuous variables with skewed distributions. A receiver operator characteristic curve was plotted to calculate the sensitivity and specificity of the cutoff values for the DWI ASPECTS and lesion volume that predicted a favorable outcome. Multivariable regression analysis was performed to identify independent predictors of a favorable outcome relative to the prespecified cutoff ASPECTS and lesion volumes. The results were expressed as odds ratio (OR) estimates of the relative risk with a 95% confidence interval (CI). Probability values less than 0.05 were considered statistically significant.
RESULTS
Two hundred and fifty-seven patients who had proximal vessel occlusion in the anterior circulation and arrived within 6 hours of symptom onset were screened for inclusion in this study. Forty-four of these patients were excluded for the following reasons: nonavailability of pretreatment DWI (n=32), poor quality images (n=2), and prestroke mRS score of ≥3 (n=10). Thus, 213 patients were finally included in the analysis.
Clinical and imaging characteristics based on age groups
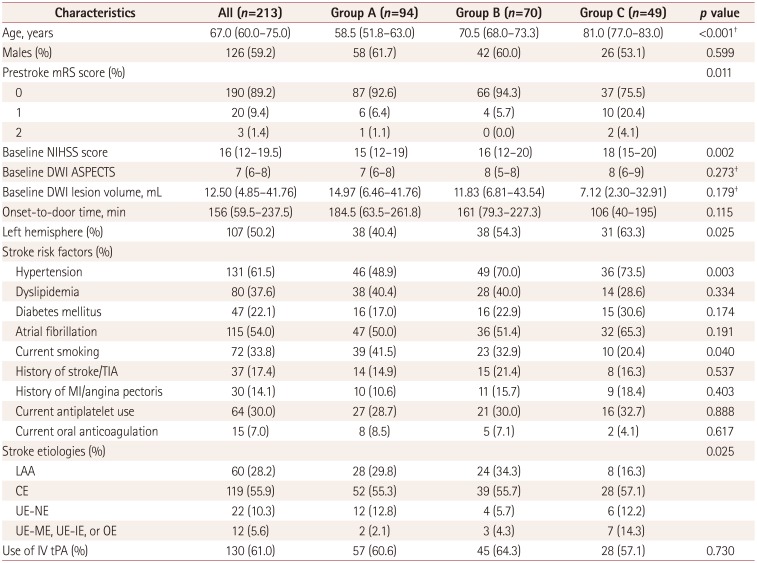
The following groups were defined based on the age at stroke onset to explore the trend between the degree of baseline ischemia and functional outcome relative to age: group A (n=94; <66 years), group B (n=70; 66–75 years), and group C (n=49; >75 years). At baseline and relative to the other two groups, group C had higher prestroke mRS and NIHSS scores, a different profile of stroke etiologies, a higher prevalence of left hemispheric involvement, a higher prevalence of underlying hypertension, and a lower prevalence of current smoking. The details of these baseline characteristics are provided in Table 1.
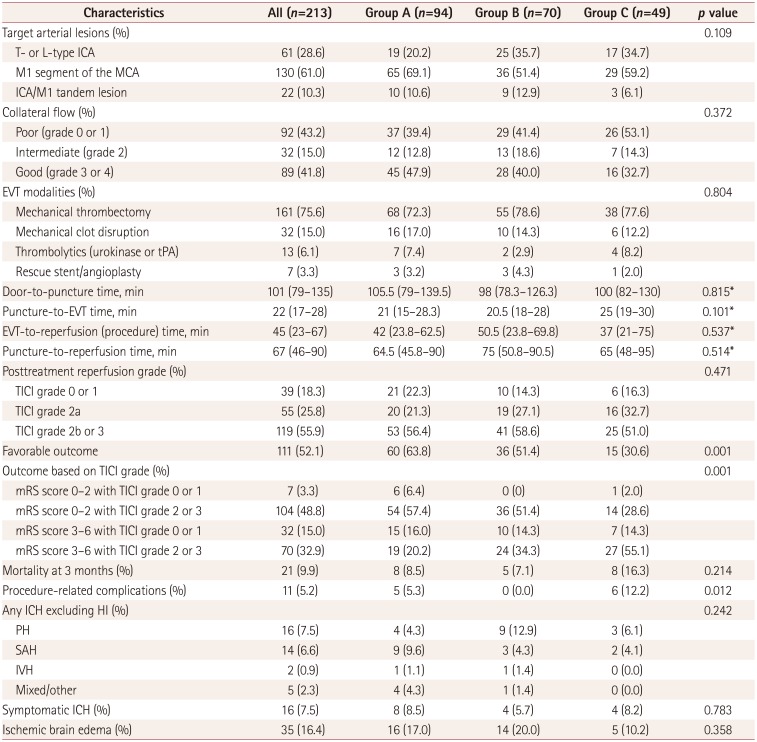
At baseline, the collateral-flow status tended to be worse in older patients [collateral flow grade 0 or 1: 26 of 49 patients (53.1%) in group C vs. 66 of 164 patients (40.2%) in groups A and B; p=0.112]. The duration from arterial puncture to the start of EVT tended to be longer in group C (p=0.101), which reflect the highest burden of vascular tortuosity and atherosclerosis in older patients during the preparation of EVT, but the total time spent on EVT (procedure time) was not different significantly in the groups, which may imply that the procedure itself was unrelated to the underlying vascular status. A favorable functional outcome was achieved in 111 of the 213 patients (52.1%) overall: in 60 of the 94 (63.8%) patients in group A, in 36 of the 70 (51.4%) patients in group B, and in 15 of the 49 (30.6%) patients in group C (p=0.001). The percentage of patients with TICI grade 2 or 3 reperfusion did not differ significantly in the three groups, but the percentage of patients with futile reperfusion was much higher in group C (55.1%, p=0.001). The rate of procedure-related complications was higher in older patients (12.2% in group C vs. 5.3 and 0% in groups A and B, respectively). The incidence rates of symptomatic intracranial hemorrhage and ischemic brain edema did not differ significantly in the groups. The details of angiographic and outcome characteristics are presented in Table 2.
Pretreatment DWI threshold for favorable outcome based on age groups
To determine the age-specific cutoffs for the pretreatment DWI ASPECTS and lesion volume, a receiver operating characteristic curve was constructed (Fig. 1). A DWI ASPECTS of 8 was found to predict a favorable outcome in groups A and B (sensitivity=51.67 and 66.67%, respectively; specificity=70.59 and 64.71%, respectively), while ASPECTS=9 was identified as favorable for group C (sensitivity=60.0%, specificity=76.47%). A DWI lesion volume of 20 mL was selected as the criterion for predicting a favorable outcome in groups A and B (sensitivity=68.33 and 80.56%, respectively; specificity=58.82 and 64.71%, respectively), while a volume of 5 mL was selected as for group C (sensitivity=60.0%, specificity=73.53%). After adjusting for age, prestroke mRS score, baseline NIHSS score, final TICI grade 2b or 3 reperfusion, and procedure time, age-specific DWI ASPECTS cutoff values remained statistically significant in predicting a favorable outcome (OR=2.387, 95% CI=1.219–4.676, p=0.011). Additionally, after adjusting for age, prestroke mRS score, baseline NIHSS score, final TICI grade 2b or 3 reperfusion, and procedure time, the age-specific DWI lesion volume cutoff values continued to remain statistically significant in predicting a favorable outcome (OR=3.595, 95% CI=1.789–7.223, p<0.001).
DISCUSSION
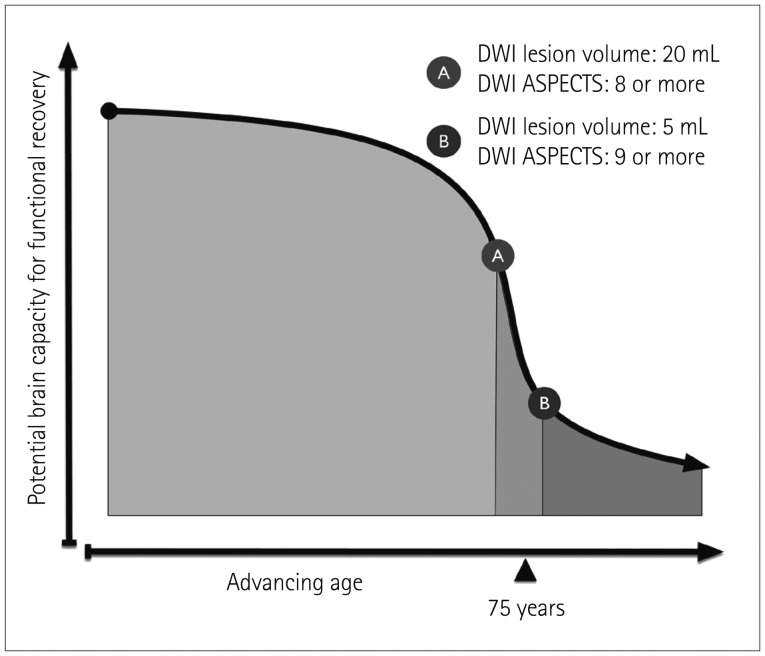
The novel finding in this study was that the baseline DWI ASPECTS and lesion volume cutoffs for a favorable outcome were much stricter in older stroke patients (≥9 and ≤5 mL, respectively) than in their younger counterparts (≥8 and ≤20 mL, respectively). Further, the rate of futile reperfusion exceeded 50% in group C (age >75 years). Both of these findings suggest that the restorative ability of the brain is weaker in older patients (Fig. 2).
In general, the risk of stroke is closely associated with age. A related finding is that the incidence of stroke is continuing to increase exponentially as an inevitable result of increased life expectancy. Older stroke patients have increased mortality and more-severe disability compared to their younger counterparts for a similar spectrum of stroke severity and pathology.28 This situation can result in physicians being reluctant to offer EVT to older stroke patients.
In our cohort, the rate of a favorable outcome was about 31% in older patients (>75 years), and the probability of them achieving a favorable outcome was much lower compared to their younger counterparts despite the similarity of their baseline characteristics and reperfusion rates. Previous studies have already shown that poor outcomes are more frequent in octogenarians.7891011121314 Poor outcomes in older patients have been attributed to higher levels of baseline disabilities, higher incidence rates of medical comorbidities and poststroke medical complications, less familial support, and withdrawal of care.29 Further, the poor restorative ability of the brain in older stroke patients (>75 years) can be a contributing factor.16 Also, a tendency for the collateral flow to be worse in older patients in our cohort could be a contributing factor to the endovascular outcome, with it being reported that the interaction between collateral adequacy and age could contribute to an adverse outcome.30
Our hypothesis that older stroke patients have a different ischemia cutoff for a favorable outcome can be investigated using baseline brain imaging. To accurately define the cutoff value for baseline ischemia, DWI is arguably superior to CT in predicting outcome.31 Ribo et al.19 examined follow-up CT images of patients obtained after 24–36 hours to determine the age-specific posttreatment infarct size predictive of a favorable outcome. They found that the target cutoff infarct volume that predicted a favorable outcome decreased with increasing age (49 mL for age <70 years, 32.5 mL for age 70–79 years, and 15.2 mL for age ≥80 years). However, that study did not examine the age-adjusted pretreatment infarct volumes. The present study examined the pretreatment lesion volume and ASPECTS, which were found to decrease and increase, respectively, with increasing age.
The limitations of this study include its retrospective design and the lack of control patients. Additionally, the type of acute treatment given or recommended to each individual patient varied considerably since it was based on the best available treatment at that time at our institute and the willingness of the patient's next of kin to proceed with the suggested active treatment approach. This means that the rate of TICI grade 2b or 3 reperfusion was lower than in recent endovascular trials, which may hinder the ability to define the optimal baseline ischemia threshold for clinical outcome despite TICI grades being adjusted in the statistical analyses. Another limitation is that the lower baseline infarct volume or higher DWI ASPECTS cutoffs for a favorable outcome might be related to a high prevalence of baseline intracranial atherosclerosis in our cohort. Finally, older patients were defined as those aged ≥76 years, which differs from many previous studies that analyzed patients aged ≥80 years.
In conclusion, our findings suggest that the age-adjusted pretreatment DWI lesion volume and ASPECTS are useful surrogate markers for functional outcome in older stroke patients. We further suggest that these results may help to define more-restrictive imaging criteria for older stroke patients in future trials. Further investigations of larger data sets from recent clinical trials would help to confirm our findings and justify their widespread clinical application.
 XML Download
XML Download