

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Problems related to the lack of knowledge exhibite by people with epilepsy (PWE) regarding their condition and its management have been reported.1,2 PWE themselves reported dissatisfaction with the information provided by medical personnel3 even when the information provided is considered to be adequate.2,4,5 This discrepancy may be attributable to medical personnel not fully understanding the educational needs of these patients and not addressing the issues that concern them.6 Due to the chronic nature of epilepsy, PWE should be provided with knowledge updates during the different stages of their lives. This requires ongoing assessment of their condition and the provision of necessary information based on their individual concerns and knowledge.
Furthermore, the level of knowledge is reported to be related to quality of life and to affect the level of stigma experienced by PWE. Baker et al. found that higher scores on an epilepsy knowledge questionnaire were associated with higher scores on the measure of psychologic adjustment.7 Moreover, a lack of medical knowledge was reported to be one of the factors predictive of an elevated stigma level.8
PWE in South Korea often have misconceptions and experience social bias associated with the disease.6,9 Although advanced Western style medicine prevails, traditional medicine, including herb medicine, remains very popular.10 This can result in the concerns and knowledge of PWE in South Korea differing from those of PWE in other countries. Nevertheless, few studies have investigated the levels of knowledge and understanding regarding epilepsy among PWE in South Korea.11 It is the responsibility of the health-care team to correct misconceptions, minimize the adverse effects of the chronic disorder, and promote the optimal quality of life in these patients.
This study was undertaken to determine the common misconceptions that PWE have about the disease, its management, and the use of antiepileptic drugs (AEDs). It also attempted to identify the factors influencing the level of knowledge in these patients.
MATERIALS AND METHODS
Of 102 consecutive patients who visited the outpatient epilepsy clinic of Seoul National University Hospital during the last week of June 2002, 23 were excluded because (1) they declined to participate (n=11) or (2) they did not understand the directions or content of the questionnaires (n=12). Thus, 79 subjects were included in this study.
The questionnaire obtained demographic data on age, gender, length of education, marital status, current employment status (currently employed vs not employed),6 and the seizure characteristics. The seizure characteristics as reported by the patients were verified by researchers in an independent review of the patients' medical records. When there were discrepancies between the patients' reported conditions and their medical records, we relied on the patient's medical records. The patients who came to the clinic every 1~3 months for epileptologist-recommended checkups were considered to have made regular hospital visits. For statistical purposes, the age, length of education, and duration of seizures were each dichotomized into two groups based on the respective mean values.
The questionnaire consisted of 27 questions in 3 categories on medical knowledge about epilepsy (11 items), lifestyle adjustments and safety issues of PWE (10 items), and AED treatment (6 items). Responses to item categories were used to calculate the correct-answer rates reflecting levels of knowledge about specific aspects of epilepsy. The questionnaire was developed based on information obtained by questioning the patients and their relatives, and on questions that experts consider that patients need to have answered. The experts in the field comprised epilepsy specialists, neurology residents, and nurses working in a neurology unit. Research nurses who counsel and educate PWE were also included due to their close contact with PWE. A content-validity index was obtained by asking the nine experts to rate the relevancy of each item on a 4-point scale12. The percentage agreement indicated that the content-validity index was 0.96. The data were analyzed with descriptive statistics, t-test, and ANOVA using the SPSS statistical package (version 11.0).
RESULTS
1. Characteristics of the patients
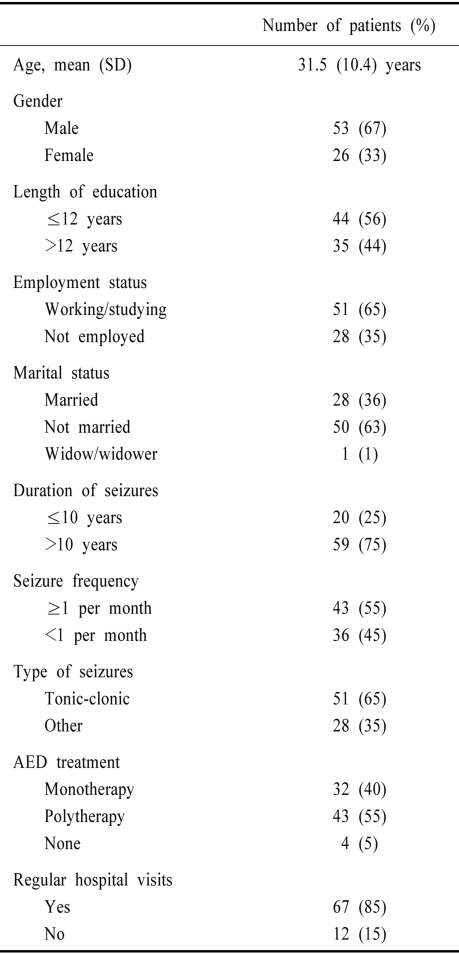
The mean age, gender, length of education, duration, type and frequency of seizures, types of AED treatment, and regularity of hospital visits are summarized in Table 1.
2. Knowledge level in the three questionnaire categories
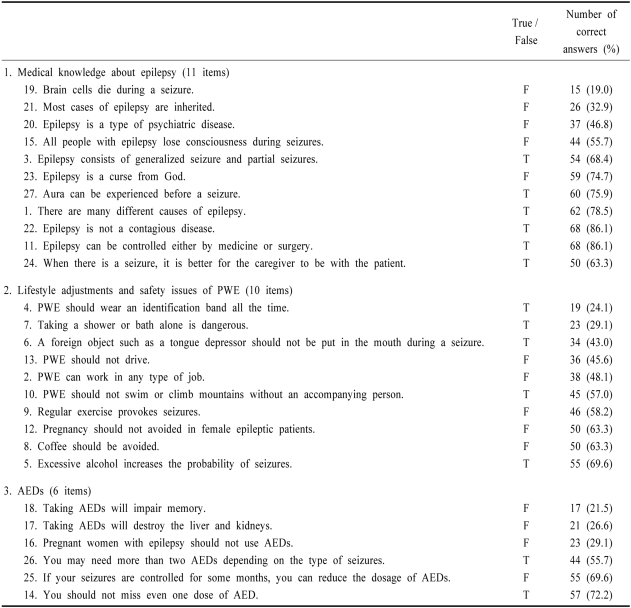
The correct-answer rates for all the items are summarized in Table 2. The mean overall correct-answer rate was 61%, and the mean correct-answer rates on questions related to medical knowledge regarding epilepsy, lifestyle and safety, and AEDs were 57%, 53%, and 48%, respectively. Sixty-four (81%) patients believed that brain cells die whenever there is a seizure. When asked about the possible causes of epilepsy, 67% responded that most cases of epilepsy are inherited, 53% attributed it to psychiatric disease, and 14% considered it to be contagious.
Regarding the lifestyles of PWE, the proportion of incorrect scores was highest in issues related to safety. Thirty-four (43%) of PWE stated that a foreign object such as a tongue depressor should not be put in the mouth during a seizure, 24% stated that epileptic patients should wear an identification band all the time, and 29% considered it dangerous to take a bath or shower alone.
Among the questions related to AED treatment, 78% believed that taking AEDs impairs the memory, 73% stated that taking AEDs destroys the liver and kidneys, 29% believed that pregnant women with epilepsy should not use AEDs since they may cause deformities of the fetus, and 72% were aware that they should not miss even one dose of AEDs.
3. Relationship between patients' characteristics and the level of knowledge about epilepsy
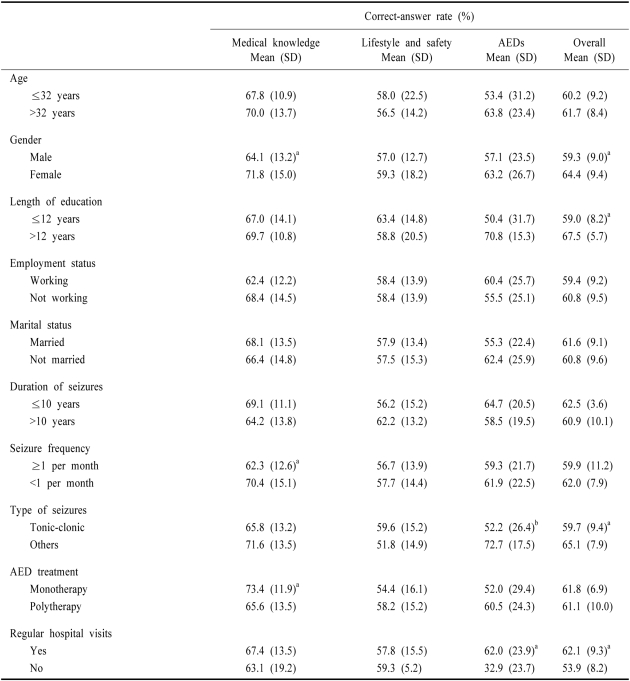
We attempted to determine the factors that were significantly related to the level of knowledge about epilepsy. As indicated in Table 3, the mean overall correct-answer rate was related to gender, length of education, type of seizures, and regularity of hospital visits (p<0.05).
The medical knowledge regarding epilepsy was significantly lower in subjects who were male, had a seizure more than once per month, and were receiving polytherapy (all p<0.05). No significant relationship was found between characteristics of patients and the correct-answer rates to questions related to the lifestyles of PWE. The correct-answer rates of answers related to AEDs were lower in subjects with the most common types of seizures (tonic-clonic) and who had not visited a hospital regularly (p<0.01). The correct-answer rate was not affected by age, duration of epilepsy, marital status, or socioeconomic status.
DISCUSSION
The aim of this study was to evaluate the knowledge of PWE regarding their disease, and also to examine the relationship between knowledge and demographic and clinical variables. The mean correct response rate was 61%, indicating that our respondents were reasonably well informed about their disease. However, poor knowledge of the cause of epilepsy, safety, and the side effects of AEDs was evident.
Although absence seizures are caused by genetic factors, our patients clearly overemphasized the role of heredity (with 67% responding that most cases of epilepsy are inherited), which is an even higher proportion than that for the general Korean population.9,13 However, this result is in agreement with previous studies from other Asian countries,14-16 and may be at least partly attributable to the influence of Chinese traditional medicine, which describes epilepsy as a genetic rather than a psychiatric illness.14
In our study, only 14% of PWE believed that epilepsy is contagious, which represents a higher level of knowledge than that exhibited by subjects in other Asian countries and Western countries.16-18 This may be due to characteristics specific to our patients. PWE who visited hospitals on a regular basis exhibited higher correct-answer rates on these items, which suggests that they received appropriate education from the medical personnel.
Most (81%) of the PWE thought that brain cells die during a seizure, indicating misconceptions regarding the nature of the disease. This may reflect the prevalent opinion in Korea that epilepsy is untreatable, as shown in a previous study.13 Similarly, other studies have found that patients express the fear that seizures could damage the brain.2,19
About half of our subjects believed that regular exercise could provoke a seizure. Although there are some anecdotal reports of patients being prone to exercise-induced seizures,20,21 most previous studies have indicated that physical exercise rarely triggers seizures,22 instead offering moderate seizure protection23 and decreasing the anxiety and depression that are common in PWE.24 However, careful guidance with respect to exercise is necessary, since accidents are reportedly fairly common in these patients.25,26
The PWE in our study displayed an obvious lack of knowledge related to safety issues associated with engaging in active sports. Only 57% correctly answered that PWE should not swim or climb mountains without an accompanying person, which is consistent with a previous Korean study.11 The correct-answer rate was low for the danger of taking a shower or bath alone, which may be attributable to PWE focusing on the risk of falling down. The low correct-answer rate for the continuous wearing of identification bands is in accordance with previous studies.1,17,27 Despite the obvious benefits of wearing a band, social prejudices in Korea may make this difficult for PWE.
Women with epilepsy consider knowledge of the specific problems and concerns to be essential, but recent data have revealed a lack of knowledge concerning women's issues and related topics.28 This was also the case in our study, where 37% of the patients responded that female epileptic patients should avoid pregnancy. Moreover, 71% believed that pregnant women with epilepsy should not use AEDs, which was much lower that the correct-answer rate in a previous study.17 This result may partly explain the results from a study involving the general Korean population, in which more than 50% of the respondents objected both to marrying epileptic people and pregnancies in epileptic women.13 This view was independent of the gender and age of the respondents.
Although 72% of our patients responded that there is a need for regular administration of AEDs, more than 70% believed that taking AEDs will impair memory. This may be attributable to some AEDs causing drowsiness, leading to the conclusion that AEDs have a harmful effect on brain function, particularly on memory. Although long-term memory has been reported to be impaired in PWE,29,30 and it is clear that some AEDs can impair memory and cognitive function, the magnitude of the effect in PWE is uncertain.31 Giovagnoli et al. also suggested that psychologic factors were correlated with subjective memory difficulties.29
More than half of our patients also believed that AEDs destroy the liver and kidneys. Considering that PWE have to take AEDs for an extended period, it is quite plausible for them to have misconceptions regarding their side effects. It is also possible that in Korea, which is still strongly influenced by traditional remedies, patients believe that AEDs damage the liver and kidneys in a way similar to herbal medicine. These results imply that the patients are fairly well informed on certain important issues, but still have specific misconceptions, and hence suggest that there is a need for further education of PWE regarding AEDs in order to improve their compliance with individual medication regimes.
In the present study, we found that gender, type and frequency of seizures, and length of education were important factors affecting both the overall and specific medical knowledge of epilepsy. Although multiple regression analysis was not performed in this study, female patients were found to be more knowledgeable than the male patients, independent of age and length of education. This is consistent with a previous study that found that women with epilepsy both want and need more information about their condition.32
Our results are also partly consistent with a previous study in which those with lower knowledge of epilepsy were more likely to have frequent seizures and be less educated.19 In contrast, Long et al. reported that the level of knowledge was not related to any characteristics of the patients.17 The reason for the discrepancy in these findings is unclear, but it may be attributable to the different characteristics and sociocultural context of the study populations. Considering that the present study involved a relatively small number of subjects, future studies involving larger samples should attempt to verify the factors related to differing levels of knowledge.
Our patients are not representative of PWE in general, or even PWE in Korea, because they were recruited from a tertiary teaching hospital and were relatively well managed and compliant. Moreover, it is likely that patients in unstable condition were underrepresented since we did not include cases for which only the carer of a patient visited the clinic. Thus, the level of knowledge about epilepsy in our patients may not reflect that of the general epilepsy population. Moreover, it is possible that the questionnaire did not encompass all the information that PWE should have on epilepsy.
Despite these limitations, the present study clearly suggests that PWE in Korea have misconceptions and limited knowledge on their condition, particularly on the issues of safety, exercise, women's issues, and the side effects of AEDs. Strategies to reduce misconceptions about the etiology of epilepsy and to improve understanding of safety issues and AEDs should be developed based on the characteristics of individual patients.
 XML Download
XML Download