

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometrial cancer (EC) is the most common gynecological malignancy among women in western countries [1]. Up to 25% of ECs demonstrate disruption of the DNA mismatch repair (MMR) pathway, manifesting as high levels of microsatellite instability (MSI-H) and/or loss of MMR protein expression by immunohistochemistry (IHC) (collectively termed ‘MMR-deficiency’) [23]. At the population level, up to 13%–25% of MMR-deficient EC cases have been reported to be caused by germline pathogenic variants in MLH1, MSH2, MSH6, or PMS2 genes (Lynch syndrome), while a large proportion (62%–73%) have been demonstrated to arise from somatic hypermethylation of the MLH1 gene promoter region [45]. In addition, consistent with findings from parallel studies in colorectal cancer, there is increasing evidence indicating that somatic causes, such as MMR deficiency, underlie the vast majority of EC cases without germline pathogenic variant identified by DNA testing. In addition to somatic MLH1 methylation, several studies have identified single or double somatic mutations in MLH1, MSH2, or MSH6 concordant with the loss of MMR protein expression observed in such pathogenic variant-negative cases [678].
Although previous studies have examined differences in EC risk factors by tumor MMR status, variation in study designs complicates comparisons. Both lower [9101112] and higher [13] body mass index (BMI) have been associated with MMR-deficient EC. No differences in risk associations by MMR status have been observed for menopausal hormone use, parity, age at menarche, menopause or first pregnancy, whereas oral contraceptive (OC) use was associated with reduced risk of MMR-deficient EC in one study [14].
The relationship between MMR deficient tumor and outcomes among women with EC has not been fully established yet. Some studies have reported significantly better survival among women with MMR deficient tumor, others have found unfavorable or no differences in outcome [1516171819202122], and a meta-analysis including 23 published studies found significant evidence of between-study heterogeneity [23]. Further, 2 studies have reported evidence that MMR status may be associated with response to adjuvant therapy [1824].
Importantly, to date, no studies assessing risk factors or survival by tumor MMR status have comprehensively discriminated between MMR deficient tumor from somatic alterations and that from germline variations in MLH1, MSH2, MSH6, or PMS2. Indeed, current evidence indicates that up to 55% of individuals defined as “probable mutation carriers,” based on tumor MSI-H status and/or MMR IHC loss with no MLH1 methylation, are likely to be non-carriers of a germline pathogenic MMR gene variant [45678]. Herein we report the findings from a large Australian population-based study of women with EC, characterized for tumor MMR protein expression and MMR gene pathogenic variant status, regarding possible differences in risk factors or survival by tumor MMR status.
MATERIALS AND METHODS
Details of the Australian National Endometrial Cancer study (ANECS) and molecular and genetic testing have been published previously [4]. Briefly, cases included Australian women aged 18–79 years, diagnosed with primary EC from 2005–2007. Population controls were randomly selected from the Australian Electoral Roll (enrolment to vote is compulsory in Australia), frequency-matched to cases by state of residence and 5-year age-group, and no history of hysterectomy. Informed consent was obtained from all participants. The study protocol was approved by Ethics Committees at QIMR Berghofer Medical Research Institute, participating hospitals, and cancer registries.
Sociodemographic, lifestyle and medical information was collected via structured interview. Clinical data including histological subtype (endometrioid, serous, clear cell, carcinosarcoma), tumor stage (II, II, III, and IV), grade (1, 2, and 3), lymphovascular space invasion (LVSI; yes, no/unknown) and adjuvant therapy (brachytherapy, chemotherapy, radiotherapy; yes for any one treatment, or no) were abstracted from medical/pathology records. Cases were re-staged using the International Federation of Gynecology and Obstetrics (FIGO) 2009 criteria. Vital status was determined from medical records and using probabilistic record data linkage to the Australian National Death Index. Survival time was calculated from date of first treatment to date of death or censored at 31 December 2013.
Women were included in risk analyses if they had completed a baseline interview (both cases and controls), and had tumor MMR IHC (cases only), and germline MMR gene test results (cases demonstrating tumor MMR protein loss of expression). After excluding women with incomplete risk factor (n=55 controls, n=58 cases), risk analysis included 691 controls and 698 cases separated into 3 groups defined by tumor MMR status: 1) MMR-proficient (n=544); 2) MMR-deficient, pathogenic variant identified (termed “germline MMR-deficient,” n=20); and 3) MMR-deficient and no germline pathogenic variant identified (termed “somatic MMR-deficient,” n=134). The latter included cases with MLH1-methylated tumors (proven somatic cause of MMR deficiency, n=104) and also cases with no somatic alteration identified as yet (assumed somatic cause of MMR deficiency, n=30).
Cases were eligible for survival analyses if they had tumor MMR IHC and results from germline MMR gene testing directed by pattern of IHC loss. After excluding women with synchronous cancers (n=15 ovarian, n=2 other), who did not have surgery (n=5), or missing information about adjuvant treatment (n=7), survival analysis included 728 women with EC (MMR-proficient, n=565; germline MMR-deficient, n=21; somatic MMR-deficient, n=142; 109 proven somatic MMR-deficient due to MLH1 methylation, 33 with assumed somatic causes of MMR deficiency).
IHC was performed on formalin-fixed paraffin embedded tumor material for cases when possible, MLH1 methylation testing was conducted for all cases with MLH1/PMS2 loss and tumor DNA available, and germline DNA genetic testing performed for individuals with tumors showing loss of expression of one or more MMR proteins [4]. Individuals with no germline DNA available for genetic testing (n=18), or identified to carry a MMR gene variant of uncertain significance (n=4), were excluded from risk and survival analyses. The pattern of MMR protein loss and MMR pathogenic variant status for cases included in analyses are detailed in Table 1.
Table 1
Details of genetic and molecular testing results for patients included in risk and survival analysis

IHC, immunohistochemistry; MMR, DNA mismatch repair; N/A, not applicable.
*Subgroups were collapsed as follows for analysis, unless otherwise stated: somatic MMR-deficient included both proven and assumed somatic MMR-deficient groups; germline MMR-deficient included germline MMR-deficient groups irrespective of pattern of IHC loss.
We used polynomial logistic regression to estimate adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for associations between known epidemiological factors and risk of EC by MMR status as defined above. Models assessing risk of EC and known epidemiological factors by MMR-proficient and somatic MMR-deficient status were adjusted for age, education, smoking status, BMI, age at menarche, OC use, parity, hormone replacement therapy (HRT) use and diabetes. As women with EC germline MMR-deficient tumors were much younger than our controls, these models were stratified by age in 5-year groups, in addition to adjusting for other factors noted above.
Cox proportional hazards regression models were used to estimate the hazard ratio (HR) for association between tumor MMR status and overall or EC-specific survival. Models were adjusted for age (continuous), histologic subtype and grade (termed histologic group), FIGO stage, LVSI, and adjuvant therapy. Because the outcome for women with EC differs by histologic subtype, additional survival analyses were restricted to women with endometrioid tumors, adjusting for tumor grade (1, 2, and 3) and other variables as above. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
The Cancer Genome Atlas (TCGA) EC patient clinical data, and gene-based, RNA-seq by Expectation-Maximization (RSEM) raw expression counts (Illumina GA platform) from EC tumor tissue were downloaded from Broad's Firebrowser server (http://firebrowse.org/). For this dataset, MMR deficiency was based on tumor MSI-H status: tumors were considered MMR-deficient if they were MSI-H, or MMR-proficient if they exhibited low/indeterminate MSI or were microsatellite stable (MSS). Our previous analysis of TCGA germline exome sequencing data [25] was used to exclude patients carrying a MMR gene variant of uncertain significance, and assign tumor status as germline or somatic MMR-deficient — with the caveat that pathogenic copy number variation was not detected by our previous sequence analysis. Analyses included patients stratified into 3 groups: 1) MMR-proficient — non-carrier of a germline MMR pathogenic variant and tumor profile was not MSI-H (n=246); 2) assumed somatic MMR-deficient — non-carrier of a germline MMR pathogenic variant and tumor MSI-H profile (n=115); and 3) germline MMR-deficient — carrier of a germline MMR pathogenic variant and tumor MSI-H profile (n=6). Differential tumor gene expression analyses were performed using the DESeq2 package in R (R Foundation, Vienna, Austria) [26] and associations adjusted for multiple testing by Benjamini-Hochberg correction [27]. Genes were considered to be significantly differentially expressed if there was >2-fold difference and the adjusted p-value was <0.05. Functional enrichment analysis was performed using the Database for Annotation, Visualization and Integrated Discovery (DAVID) website [2829].
Note, the TCGA EC dataset was not used to conduct comparable survival analysis for replication purposes, since assignment of pathogenic variant status was considered incomplete (see above), and key prognostic variables (LVSI status, adjuvant therapy treatment) were unavailable. However, we note that no deaths were observed at time of last follow-up among TCGA cases carrying germline MMR gene pathogenic variants.
RESULTS
Cigarette smoking was significantly associated with reduced risk of MMR-proficient EC (OR for ever-smoking=0.64; 95% CI=0.49–0.83), with non-significant inverse associations also seen for MMR-deficient cancers (Table 2). Higher BMI (BMI ≥35 kg/m2) was associated with significantly increased risk of MMR-proficient and somatic MMR-deficient EC (OR=7.65; 95% CI=5.09–11.50 and OR=5.28; 95% CI=2.81–9.91, respectively). Younger age at menarche was associated with increased risk of MMR-proficient, but not with somatic MMR-deficient EC. Increased duration of OC use was significantly associated with reduced risk of MMR-proficient and somatic MMR-deficient ECs (OR for 120+ months=0.36; 95% CI=0.25–0.51 and OR=0.26; 95% CI=0.14–0.50, respectively), as was increasing parity (OR for ≥3 children=0.27; 95% CI=0.17–0.41 and OR=0.34; 95% CI=0.18–0.65, respectively). A history of diabetes was associated with an increased risk of somatic MMR-deficient EC (OR=3.29, 95% CI=1.77–6.12) and a non-significant increased risk of MMR-proficient EC (OR=1.60, 95% CI=0.99–2.58), with suggestive evidence for a difference in these estimates (p heterogeneity=0.07). Neither education nor HRT use were associated with risk of MMR-proficient or somatic MMR-deficient EC. The risk estimates for the 20 germline MMR-deficient EC cases were consistent with a protective effect for smoking, OC use, parity, and increased risk for younger age at menarche, however given the small number of cases none of these results were significant. No pathogenic variant carriers reported a history of diabetes.
Table 2
Adjusted ORs and 95% CIs for the association between demographic, hormonal, lifestyle factors and endometrial cancer risk according to tumor MMR status

BMI, body mass index; CI, confidence interval; HRT, hormone replacement therapy; MMR, DNA mismatch repair; OC, oral contraceptive; OR, odds ratio; SD, standard deviation.
*Models adjusted (where appropriate) for age (continuous), education, cigarette smoking, BMI, age at menarche, oral contraceptive use, parity, hormone replacement therapy use, diabetes; †Models adjusted (where appropriate) for education, cigarette smoking, BMI, age at menarche, oral contraceptive use, parity, hormone replacement therapy use, diabetes, stratified by 5-year age groups; ‡None of the pathogenic variant carrier cases reported diabetes.
To further explore the relationship observed between tumor MMR status and diabetic status, we investigated differences of endometrial tumor gene expression among the three comparison groups defined by germline pathogenic variant status and tumor MMR proficiency/deficiency. Comparison of germline MMR-deficient versus somatic MMR-deficient tumors identified 79 significantly differentially expressed genes (Supplementary Table 1), and 31 falling into the metabolic disease class, but there was no evidence for significant functional enrichment after Benjamini-Hochberg adjustment (Supplementary Table 2). There was significantly different expression of 1,218 genes between MMR-proficient and somatic MMR-deficient tumors (Supplementary Table 3), with genes in the metabolic disease class (Supplementary Table 4) identified as the most significantly enriched (Benjamini-Hochberg adjusted p-value=2.98×10−10). Results were similar when restricting to tumors of endometrioid subtype only. There were 92 differentially expressed genes between germline MMR-deficient versus somatic MMR-deficient (Supplementary Table 5) and nominal evidence (Benjamini-Hochberg adjusted p-value=0.01) for enrichment of genes in the metabolic disease class (Supplementary Table 6). Comparison of MMR-proficient and somatic MMR-deficient tumors identified 876 differentially expressed genes (Supplementary Table 7), and genes in the metabolic disease class (Supplementary Table 8) were again identified as most significantly enriched (Benjamini-Hochberg adjusted p-value=3.27×10−9).
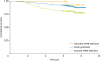
Among women with MMR-proficient and somatic MMR-deficient ECs, >70% had early stage grade 1/2 endometrioid tumors (Table 3). Women with germline MMR-deficient EC were somewhat more likely to have high grade endometrioid or non-endometrioid tumors, and higher stage disease. LVSI and use of any adjuvant therapy were more common in both MMR-deficient groups, compared to women with MMR-proficient EC. Overall, 125 (17%) women died during the follow-up period (range, 3.0–8.5 years), 89 of EC. None of the 21 women who carried a germline MMR pathogenic variant died as a result of their EC. Five-year survival in the cohort was 87%. As expected, older age at diagnosis, increasing tumor stage, high grade endometrioid and serous/clear cell /carcinosarcoma histologic subtypes and presence of LVSI had clear adverse effects on survival (Table 4). After adjustment, no significant association was observed between MMR status and overall or EC-specific survival. However, in analysis restricted to women with endometrioid histologic subtype, there was evidence of a survival disadvantage for women with somatic MMR-deficient EC versus MMR-proficient EC (Fig. 1). After adjusting for age, tumor grade, stage, LVSI and adjuvant therapy, the HR for overall survival (OS) was 1.50 (0.91–2.47) and for EC-specific survival 2.18 (1.19–4.01) (Table 4). This association remained when restricting analysis to the subgroup with MLH1 methylation only (OS HR=1.59; 95% CI=0.94–2.70; EC-specific survival HR=2.10; 95% CI=1.10–4.00, respectively).
Table 3
Descriptive characteristics of the cohort (n=728) included in the survival analysis, by MMR status
Table 4
Association between clinical and pathologic factors, tumor MMR status and overall and EC-specific survival

CI, confidence interval; EC, endometrial cancer; HR, hazard ratio; MMR, DNA mismatch repair.
*Adjusted for age (continuous), stage, histologic group, lymphovascular space involvement, adjuvant therapy; †Adjuvant therapy = brachytherapy or radiotherapy or chemotherapy; ‡None of the pathogenic variant carrier cases died from EC; ∥Adjusted for age (continuous), stage, grade, lymphovascular space involvement, adjuvant therapy.
DISCUSSION
We examined the association between EC tumor MMR status, lifestyle and hormonal risk factors and clinical outcomes in a large group of Australian women, characterized for tumor MMR expression and MMR gene pathogenic variant status. Consistent with most previous research, our results suggest that factors generally associated with risk of developing EC (e.g., parity, OC use, obesity and diabetes) were associated with MMR-proficient and also MMR-deficient EC known/most likely to be due to somatic MMR gene inactivation. We did not observe significant associations among the small group of women with MMR-deficient EC due to a germline pathogenic MMR gene variant, but direction of associations was generally consistent with those for somatic MMR-deficient patients.
Interestingly, the diabetes-EC association was particularly strong among women with somatic MMR-deficient EC, with a threefold increased risk of somatic MMR-deficient EC among women who reported a history of diabetes. There is consistent epidemiological evidence for an independent association between diabetes and increased EC risk, and observational studies have shown that insulin resistance, hyperinsulinemia, hyperglycaemia, inflammation and disturbances in the IGF-1 pathway may contribute to carcinogenesis among diabetics [3031]. Mendelian randomization analysis, which uses genetic markers to overcome some of the biases affecting conventional studies, supports a causal association between EC risk and genetic risk of higher insulin levels independent of BMI, but not a causal association with genetic risk of type 2 diabetes or higher fasting glucose [32]. Our analysis of the public TCGA endometrial tumor dataset identified differential gene expression between tumors from germline MMR-proficient and somatic MMR-deficient patients, when considering tumors of all subtypes (1,218 genes) or endometrioid subtype only (876 genes). These genes were significantly enriched for pathways related to the metabolic disease class (including diabetes mellitus, gestational diabetes, hyperinsulinemia, insulin resistance, hyperglycemia), providing support for an association between diabetic-related traits and somatic MMR-deficient patients.
Despite the high proportion of EC with tumor MMR deficiency, the impact on prognosis is unclear. A 2013 systematic review of 23 EC studies (median sample size 112) noted considerable differences in the methodology used to designate MMR-deficiency, differences in analytic approaches with respect to inclusion of covariates, and identified marked inter-study heterogeneity for risk estimates; meta-analysis of the 6 studies reporting associations with OS yielded a non-significant association between MSI-H tumor status and poor OS (HR=2.02; 95% CI=0.85–4.83; I2=82%) [23]. The largest study in the meta-analysis [15] (n=473) included non-endometrioid endometrial tumors known to have worse clinical outcomes and lower rates of MMR-deficiency, and when this study was excluded from the meta-analysis, MSI-H status was associated with worse overall (HR=2.91; 95% CI=1.24–6.80; p=0.010) and disease-free survival (HR=2.55; 95% CI=0.57–11.38; p=0.220). Findings have varied from subsequent studies of varying design assessing survival using multivariate analysis: no association was detected between tumor MMR-deficiency and survival from analysis of 109 EC patients (endometrioid and non-endometrioid subtypes; MSI-H=0.46; 95% CI=0.05–4.77) [33], improved survival (HR=0.2; 95% CI=0.1–0.7) was reported for MMR-deficient EC based on IHC results from 191 EC patients [24]; no association between tumor MMR class and outcome was observed for 1,024 patients designated as epigenetic MMR defective EC (HR=0.78; 95% CI=0.43–1.41) or “probable MMR mutation” (HR=0.91; 95% CI=0.40–2.07) [18]. The most recent study of 466 women reported that endometrioid MLH1-methylated MMR-deficient EC cases had significantly reduced recurrence-free survival in univariate analysis (p<0.001) [22]; a recent study of 385 Thai women reported improved survival for patients exhibiting tumor MMR deficiency [34], although it should be noted that MMR loss of function was observed for a relatively large proportion of their cohort (55%, 33% ascribed to loss of MLH1 function) compared to what has been previously reported for largely Caucasian cohorts.
Importantly, no studies to date have separated proven germline MMR-deficient EC from known/assumed somatic MMR-deficient EC. Further, for the largest single study [18] and the most recent [22], categorization of MMR-defective cases due to presumed MMR pathogenic variants was inappropriate, with “probable MMR mutation” cases defined as MSI-H and/or MMR IHC loss with no MLH1 methylation. Based on current evidence, up to 55% of individuals in this category are likely non-carriers of a germline pathogenic variant, resulting in misclassification of up to 5% of cases overall, and up to 15% of MMR-deficient cases [45678]. Our study separated MMR-deficiency proven to be due to germline pathogenic variants in MMR genes [4] from tumor MMR-deficiency due to known or assumed somatic causes [4678]. MMR-deficiency was enriched in tumors with poor prognostic markers, with some differences between somatic MMR-deficient tumors and the small number of germline MMR-deficient tumors. Compared to MMR-proficient tumors, higher tumor grade and stage, and presence of LVSI were more common in germline MMR-deficient tumors, whereas only higher grade and LVSI were slightly more common in somatic MMR-deficient tumors. MMR-deficient cases (somatic and germline) were also more likely to have received adjuvant therapy, consistent with the higher proportion with poor prognostic features.
The number of women with germline MMR pathogenic variants detected in our population-based study was small, and the overall frequency is consistent with that reported in other unselected EC studies [5]. Notably, 20/21 pathogenic variant carriers were alive at follow-up, and the remaining patient was reported to be deceased from another cause. In multivariate analysis of patients with all EC subtypes, there was no evidence for an association between somatic tumor MMR-deficiency and overall or cancer-specific survival. However, after restricting analysis to the most common endometrioid subtype, we did observe an increased hazard for women with somatic MMR-deficient endometrioid subtype EC (EC-specific survival HR=2.18), observed also for the subset of women with proven MLH1-methylated basis for MMR-deficiency (EC-specific survival HR=2.23). This latter finding is consistent with a recent study reporting reduced recurrence-free survival associated with MLH1-methylated MMR-deficiency in univariate analysis [22].
We highlight that no women in our study with germline MMR-deficient EC died due to their EC, compared to 18/109 (16.5%) women with MMR deficiency due to somatic MLH1 methylation, and 4/33 (12.1%) women with no germline MMR pathogenic variant identified and tumor MMR deficiency highly likely to be due to other somatic causes. These observations suggest that previous studies which did not separate out proven pathogenic variant carriers, or inappropriately assigned individuals exhibiting tumor loss of expression for MSH2/MSH6, MSH6, or PMS2 as pathogenic variant carriers, may have masked differences in survival between MMR-proficient and other MMR-deficient groups.
Further studies will be required to confirm our findings, and investigate a biological basis to support differences in survival between germline and somatic MMR-deficient EC cases, and MMR-proficient cases. A recent study compared tumor expression of protein markers of immune response in EC specimens stratified into 3 categories: MSS (n=96), pre-screened to exclude samples with POLE somatic alterations known to be associated with good prognosis; “sporadic” MSI-H (n=38); and “hereditary” MSI-H (n=20), with misclassification of 4 cases with no pathogenic MMR variant identified by genetic testing, and no genetic testing performed for another case [35]. Compared to MSS tumors, immune cell infiltration was increased in MSI-H tumors, but with a difference in immune response between so-called sporadic and hereditary tumors. Our analysis of TCGA mRNA expression data delineating cases as germline MMR deficient, somatic MMR-deficient or MMR proficient, did not highlight differential expression of genes in the immune pathway. Genes in the metabolic disease class were by far the most significantly differentially expressed between somatic MMR-deficient and MMR-proficient tumors for all tumor subtypes (p=2.98×10−10) or endometrioid subtypes only (p=3.27×10−9), with nominal evidence for enrichment of genes in the immune pathway (p=0.050; p=0.030 endometrioid only).
Major strengths of our population-based study include its large sample size, examination of 3 different MMR end-points with clear separation of MMR-deficiency due to germline alterations, a high case-response rate (67% of those invited) [4], and comprehensive control of other risk/prognostic factors. We acknowledge that the subgroup termed somatic MMR-deficient included a proportion of cases with assumed (but not proven) somatic MMR deficiency, but we note that our survival results of interest were essentially unchanged when restricting to cases with proven somatic MMR-deficient cases. Although we did not perform MMR gene testing for controls, assuming a MMR gene pathogenic variant carrier rate of <1/250 in the general population, we would expect at maximum misclassification of 3 control individuals for the risk analysis component of our study. Despite the large size of our study, few cases were proven germline MMR-deficient, limiting power to detect differences in risk and survival for this group, and we acknowledge that such analyses should be considered exploratory.
Further, we had no information on other tumor somatic markers known to be associated with prognosis [36], namely POLE and TP53 status. We cannot exclude the possibility that “good-prognosis” POLE somatic alterations may be enriched in patients with MMR-proficient tumors, since review of the reported EC TCGA data [36] for endometrioid subtype cancers indicates that tumors with POLE somatic alterations and ultramutated phenotype associated with good phenotype (17/28 endometrioid tumors denoted as carrying a POLE somatic mutation) comprised 14/119 (12%) of MSS versus 3/68 (4%) of MSI-H endometrioid tumors (p=0.100). However, unmeasured TP53 status is unlikely to have confounded our observed associations with MMR status for endometrioid subtype cancers; TP53 status is strongly correlated with non-endometrioid histology and high grade, factors considered in our analysis.
In summary, while EC risk associations do not differ substantially by tumor MMR status, separation of germline from somatic causes of MMR-deficiency indicates that patients with endometrioid subtype somatic MMR-deficient tumors may have poorer EC-specific survival than those with MMR-proficient tumors.
 XML Download
XML Download