

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cancer in Indonesia is positioned as the fifth of cause of death, due to increasing number of cancer patients year by year by the increasing life expectancy of Indonesian women. Life expectancy corresponds with the improvement of socioeconomic condition. More than 40% of female malignancies are gynecological cancers. Data about this in international publication is very rare or not appear. Therefore the purpose of this paper is to give information more about gynecological cancer in Indonesia.
DEMOGRAPHY
Indonesia is an archipelago with a big and dense populated area. The natural increase rate of population is still high since the birth rate is much greater than the death rate. The female population is slightly less than the male population, but the life expectancy of the female is longer than the male. Indonesia is categorized as a poor country or developing country especially after the economic crises hit Indonesia in 1998. The gross national product (GNP) and the personal GNP is lower among Asian countries (Table 1).
CANCER REGISTRY
Up to now, we do not have a body or institution of cancer registry such as in the developed country. What we have is a pathological cancer registry run by Indonesian Association of Anatomic Pathology in Collaboration with Indonesian Cancer Society. They collect the data from 13 laboratories of anatomic pathology spreading over several regions or provinces. While cancer data from hospitals is part of the disease reporting, reported by provinces and districts hospitals organized by Department of Health. Beside that Indonesian Society of Gynecologic Oncology now also develop a registry adopted from reporting system made by the International Federation of Gynecology and Obstetrics (FIGO). The reports come from academic hospitals where one or several gynecologic oncologists practice. An academic hospital is also as a top referral hospital at a respective region or province.
EPIDEMIOLOGY OF GYNECOLOGIC CANCER IN INDONESIA
1. Incidence
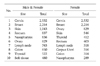
Since we do not have an established cancer registry, Department of Health assumes cancer incidence to be 100 per 100,000 people. Based on pathology, there were 10 most frequent cancer in male and female together i.e. cancer of the cervix, breast cancer, skin, rectum, nasopharynx, ovary, lymph nodes, colon, thyroid, and soft tissue. Cancer of the cervix also appears as the most frequent cancer among female, and its position was the first rank, followed by breast, ovary, skin, thyroid, rectum, lymph nodes, uterus, colon, nasopharynx.1,2 There were slight differences between pathological and hospital-based data (Table 2). Cancer of the cervix was about 75% among gynecological cancer and they were mostly diagnosed at advanced stages (Table 3).
2. Age
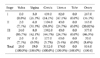
The peak age group in gynecologic cancer especially cervix, uterus and ovary was between 45-54 years old as shown in Table 4.
CERVICAL CANCER
1. Human Papilloma Virus
We have already known that Human Papilloma Virus as a causative agent of the lower genital tract malignancy, especially cancer of the cervix. We have biopsy specimens from 76 patients with cancer of the cervix, and HPV DNA was detected in around 96% and especially HPV 16 and 18 were found in 83%.3 This figure was only slight different from those found in Netherlands and Suriname (Table 5).
2. Risk factors
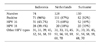
There was a hospital-based case control study at Dr Cipto Mangunkususmo Hospital (the top national referral hospital) that involved 143 cases of cervical cancer and 143 control cases. It reveals that risk factors in cervical cancer were age > 50 year, lower education, unemployment, age at first intercourse < 20 years, number of partners > 1, and parity ≥ 6 (Table 6).
SURVIVAL
It was very difficult to obtain 5-year survival rate nationally because our follow-up system is very poor. Many patients did not come regularly or failed to be followed up, or they frequently moved from one place to another place.
Studies of cervical, ovarian (178 cases) and endometrial cancer (72 cases) at the Dr Cipto Mangunkusumo Hospital found that the survivals at five years were as follow: 1) five-year survival rate in cervical cancer stage I, II, III, IV were 50%, 40%, 20% and 0% respectively. 2) Overall five-year survival rate of carcinoma of the ovary was 54.8%. If sub-classified by stage, five-year survival rates were 94.3%, 75.0%, 31% and 11.7% for stage I, stage II, stage III, and stage IV respectively. 3) Five-year relapse-free survival rate of endometrial cancer was 71.9%.
CANCER CONTROL PROGRAM
1. Program of Department of Health
Collaboration program JHPIEGO and Department of Health cover some regions in West Java, Central Java and East Java. This program consisted of training for the trainers and then trains the health providers such as general doctors, midwives and nurses. The activities are screening the women at risk at some region. The examination is with visual inspection with acetic acid (VIA).
2. See and Treat Program
This program is in collaboration with Female Cancer Program University of Leiden. The program initiated with three centers i.e. Jakarta, Tasikmalaya and Bali and then extended to North Sumatra, South Kalimantan and North Sulawesi.4 Table 7 shows the preliminary results. VIA positive rate was 4.5%, and as result, 1,346 of 1,556 women were treated. Therefore, the coverage in single visit is 86.5%.
SUMMARY
Indonesia is the biggest archipelago with a dense population but the income per capita still low (poor country). The most gynecologic cancer is cervical cancer, followed by ovary and uterine cancer. These cancers are included in the most ten cancers in Indonesia. The five-year survival rates are comparable with world report.




 XML Download
XML Download