

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Approximately 17 million new cases of breast cancer (BC) each year are expected to occur worldwide, and BC is the second most common cancer among Korean women.1 In Korea, 46.6% of all women newly diagnosed with BC during 2012 were premenopausal, and the largest proportion of newly diagnosed BC patients that year were aged between 40 and 49 years (34.5%).1 The proportions of both estrogen receptor (ER)-positive and progesterone receptor (PR)-positive BC patients have increased steadily since 2002, from 58.2% in 2002 to 74.1% in 2014 (27.3% increase) for ER-positive disease and from 50.7% in 2002 to 62.4% in 2014 (23.1% increase, p=0.001) for PR-positive BC.2
Unquestionably, tamoxifen use as an adjuvant endocrine therapy has been effective in reducing recurrence and increasing survival of ER-positive BC patients.34 Recently, several studies have shown that continuing tamoxifen therapy for 10 years is associated with lower recurrence and mortality rates than treatment for 5 years in patients with ER-positive BC.56 With the growing number of younger BC patients, the use of tamoxifen, as well as concurrent gonadotropin-releasing hormone (GnRH) agonists, has increased. As a result, surveillance for endometrial pathologies in younger BC patients is an important issue.
While older age, menopausal status, longer duration of tamoxifen use, and the presence of abnormal uterine bleeding are known risk factors for endometrial cancer in tamoxifen-treated women, few studies have evaluated risk factors for endometrial pathology in premenopausal women treated with tamoxifen. Moreover, all women (both before and after menopause) involve an increased risk of developing endometrial polyps secondary to tamoxifen use,7 and it has been suggested that postmenopausal patients treated for more than 2 years have a higher frequency of endometrial pathologies.8 Considering the high proportion of premenopausal BC women and their unique characteristics in Korea, it is critical to define the characteristics of tamoxifen-treated premenopausal women and identify any potential endometrial effects that may arise from this treatment. To date, endometrial surveillance strategies are not age based. Thus, the purpose of the present study was to investigate the prevalence of endometrial pathologic lesions in premenopausal tamoxifen-treated BC patients and to evaluate risk factors associated with the development of these lesions.
MATERIALS AND METHODS
This study included all premenopausal BC women treated with adjuvant tamoxifen who had undergone ultrasonography and endometrial biopsy with or without hysteroscopy at Seoul National University Hospital from January 2013 through December 2016.
We excluded patients with any of the following characteristics from our analysis: 1) lack of regular menstrual cycles or menstruation within 3 months before the first day of chemotherapy; 2) no tamoxifen treatment; 3) serum follicle-stimulating hormone level >40 mIU/mL at the outpatient visit; and 4) insufficient clinical and/or pathologic data. Transvaginal or transrectal ultrasonography was performed regardless of the menstrual cycle day. All patients had undergone BC surgery and were treated postoperatively with tamoxifen. Other treatments included a GnRH agonist, chemotherapy, and/or radiotherapy. This retrospective study was performed with approval from the Institutional Review Board of Seoul National University Hospital (No.1911-159-1082).
The usual clinical approach at our institution is as follows. Most asymptomatic patients treated with tamoxifen undergo yearly ultrasonography examinations. If a patient has abnormal bleeding with or without endometrial thickening, we perform hysteroscopic evaluation. Additionally, endometrial biopsy is performed if endometrial thickness is greater than 10 mm or if a new or enlarging polypoid lesion is observed, even in the absence of symptoms.
As previously described,9 diagnostic hysteroscopy was performed in the outpatient clinic using a 5-mm hysteroscope (Richard Wolf Medical Instruments Corp., Vernon Hills, IL, USA). If an endometrial lesion was identified, immediate resection of the lesion was performed. Deferred inpatient surgical hysteroscopy was performed in patients unable to tolerate the outpatient procedure and in patients with cervical stenosis or large lesions. A 10-mm resectoscope (Karl Storz Endoskope, Tuttlingen, Germany) was used for surgical resection of endometrial lesions, and Urosol (CJ Cheiljedang, Seoul, Korea) was used as the distension fluid. Hysteroscopic findings and clinicopathologic data were obtained retrospectively from the medical records. Information regarding the following variables were collected: age, body mass index (BMI), parity, stage, duration of tamoxifen treatment, other nonsurgical treatment (chemotherapy, radiotherapy, GnRH agonist), presence of menstruation, occurrence of chemotherapy-induced amenorrhea, endometrial thickness, and presence of abnormal uterine bleeding.
Statistical analysis was performed using IBM SPSS ver. 23.0 software (IBM Corp., Armonk, NY, USA). Age, BMI, parity, duration of tamoxifen treatment, and endometrial thickness were compared using Student's t-test. Stage, history of chemotherapy treatment, and presence of abnormal uterine bleeding were compared using the chi-square test. Univariate and multivariate analyses were performed to identify risk factors associated with the presence of endometrial pathology (endometrial hyperplasia or endometrial cancer). Two-sided p values less than 0.05 were considered statistically significant.
RESULTS
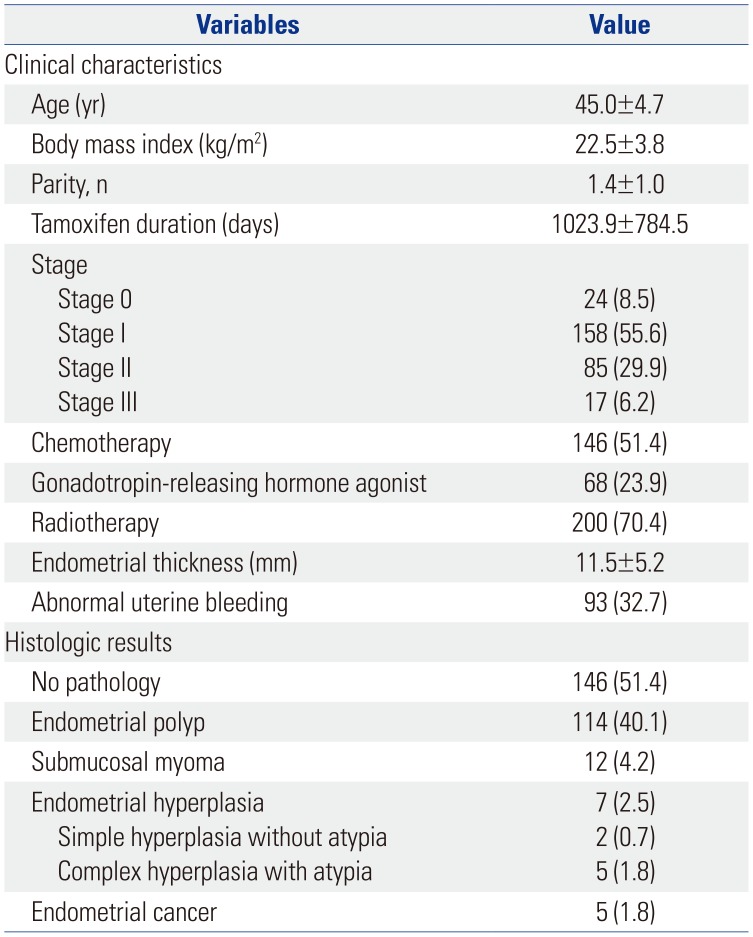
A total of 284 patients were included in this study. Table 1 shows the patients' characteristics. Their mean age was 45 years (range, 27–57) and mean BMI was 22.5±3.8 kg/m2. The mean duration of tamoxifen treatment was 1023.9 days (2.8 years). Most patients were diagnosed with BC at an early stage: stage 0, 8.5% (n=24); stage I, 55.6% (n=158); stage II, 29.9% (n=85); and stage III, 6.2% (n=17). Moreover, 51.4% of patients received cytotoxic chemotherapy before or after breast surgery; 95.8% of these patients experienced chemotherapy-induced amenorrhea. Mean endometrial thickness on ultrasonography was 11.5±5.2 mm, and 32.7% of patients experienced abnormal uterine bleeding.
The final histologic outcomes of 284 endometrial biopsies are presented in Table 1. Endometrial polyp was the most common abnormal histology (n=114, 40.1% of biopsies). Endometrial hyperplasia was present in 7 patients (2.5%), and endometrial cancer was observed in 5 patients (1.8%). Atypia was present in all biopsies exhibiting complex endometrial hyperplasia.
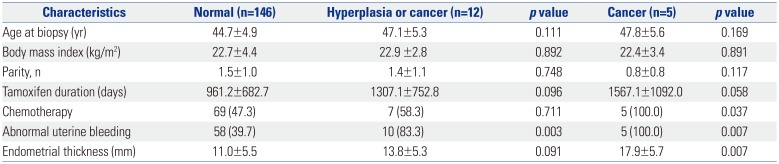
Table 2 shows the factors potentially associated with the presence of endometrial pathology in our tamoxifen-treated patients. A histologic diagnosis of endometrial hyperplasia or cancer was not significantly associated with age, BMI, parity, duration of tamoxifen use, treatment with chemotherapy, or endometrial thickness. Meanwhile, however, the rate of abnormal uterine bleeding was significantly higher in patients with endometrial hyperplasia or cancer than in those with normal endometrium (p=0.003). Moreover, a histologic diagnosis of endometrial cancer was significantly associated with the presence of abnormal uterine bleeding, treatment with chemotherapy, and endometrial thickness. The rate of abnormal uterine bleeding was significantly lower in women with endometrial polyps than in those with endometrial pathology (p<0.001) (Supplementary Table 1, only online). In addition, treatment with chemotherapy, abnormal uterine bleeding, and endometrial thickness were associated with endometrial cancer. Age, BMI, and duration of tamoxifen use did not differ between women with endometrial hyperplasia or cancer and women with endometrial polyps.
Univariate and multivariate analyses were performed to explore associations between endometrial pathology and the following potential risk factors: age, duration of tamoxifen use, endometrial thickness, presence of abnormal uterine bleeding, and treatment with chemotherapy. The results showed that only abnormal uterine bleeding was significantly associated with the presence of endometrial hyperplasia or cancer (hazard ratio, 7.3; 95% confidence interval, 1.417–37.668; p=0.017) (Table 3).
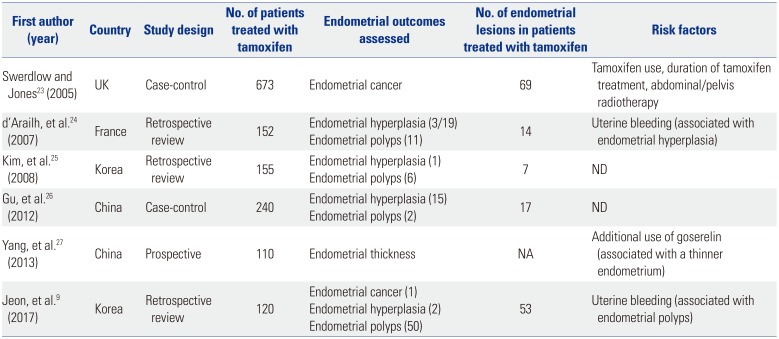
We also reviewed six previous studies that assessed the endometrium in premenopausal women receiving tamoxifen treatment. The characteristics and results of these studies, which included 1450 women in total, are presented in Table 4. Four of these studies reported risk factors associated with endometrial changes. Two studies identified symptoms (uterine bleeding) as a risk factor, and one study identified duration of tamoxifen treatment as a risk factor.
DISCUSSION
In this study, we found that the presence of abnormal uterine bleeding was the most important factor associated with the presence of endometrial pathology (hyperplasia or cancer) and that abnormal uterine bleeding, treatment with chemotherapy, and increased endometrial thickness on ultrasonography were risk factors associated with endometrial cancer in premenopausal women with BC treated with tamoxifen.
Previous studies have reported that tamoxifen is associated with dose- and time-dependent increases in the risks of endometrial proliferation, polyps, hyperplasia, and invasive carcinoma, as well as uterine sarcoma.71011121314 In the current study, the mean durations of tamoxifen use in women with normal endometrium and endometrial hyperplasia or cancer were 2.6 and 3.5 years, respectively. However, duration of tamoxifen use was not associated with the presence of endometrial pathology. Previous studies reported significantly increased risks of endometrial cancer after 2 years of tamoxifen use.15 Large prospective research is required to clarify the role of tamoxifen as a potential risk factor for the development of endometrial cancer.
Menopausal status and older age have previously been reported to increase the risk of endometrial cancer in tamoxifen users,161718 whereas premenopausal women exhibit a lower risk of endometrial cancer, even if they are symptomatic.19 Although the actual risk of endometrial pathology in premenopausal women was not assessed in the present study, our findings suggest that appropriate surveillance is important in premenopausal tamoxifen users.
Another well-known risk factor for both breast and endometrial cancers is obesity.20 However, BMI was not associated with the presence of endometrial pathology in our study. The overall lower BMI in Asian women, compared with Western women, and the small number of patients with endometrial pathology might explain the discrepancy between our results and those of previous studies.
Endometrial polyps are the most common uterine pathology in postmenopausal tamoxifen-treated BC patients. However, there is limited research on the risk of malignant transformation of endometrial polyps in premenopausal tamoxifen-treated BC patients. We found that the prevalence of endometrial polyps in premenopausal women receiving tamoxifen was 40.7%, and the majority of these patients were asymptomatic. Moreover, the presence of abnormal uterine bleeding was significantly higher in patients with endometrial hyperplasia and cancer than in those with endometrial polyps.
Evaluation of endometrial thickness by ultrasonography is the most commonly used tool for gynecologic surveillance in tamoxifen-treated BC patients. However, the diagnostic accuracy of this method is not particularly great, even when setting the cut-off value at 10 mm.2122 Establishing an appropriate cut-off value in premenopausal women is difficult because the appearance of the endometrium varies in relation to the menstrual cycle. Therefore, endometrial appearance or presence of abnormal uterine bleeding should be considered in conjunction with endometrial thickness when performing gynecologic surveillance in women treated with tamoxifen.
According to guidelines from the American Congress of Obstetricians and Gynecologists, premenopausal patients with a history of tamoxifen use involve no known increased risk of endometrial cancer and do not require any further monitoring beyond routine gynecologic examinations.7 However, resection of endometrial polyps diagnosed by ultrasonography in postmenopausal tamoxifen-treated BC patients is recommended because of the relatively high risk of malignancy in these women. Although the potential for malignant transformation is lower in premenopausal patients than in postmenopausal BC patients, we suggest that removal of endometrial polyps ought to be considered in premenopausal tamoxifen-treated BC patients. This may be important for patients with a relatively thick endometrium (e.g., ≥12 mm) and abnormal uterine bleeding, as these factors further increase the probability of endometrial cancer.
We identified six previous studies involving endometrial assessments in premenopausal women treated with tamoxifen.92324252627 Most were retrospective or case-control studies. The single prospective study assessed only endometrial thickness and did not report the presence of, or risk factors for, endometrial pathology. Very limited evidence from the other five studies suggested that abnormal uterine bleeding and tamoxifen duration are risk factors for endometrial hyperplasia or cancer in premenopausal women treated with tamoxifen.
There are a few limitations to this study. Because this was a retrospective study, endometrial thickness results were not available for the majority of patients before starting tamoxifen treatment. However, most of our asymptomatic patients treated with tamoxifen underwent annual ultrasonography examinations after beginning therapy, often with subsequent hysteroscopic evaluation. Another limitation of the study was that the number of patients with endometrial pathology was insufficient to allow estimation of endometrial thickness cut-off values for predicting the development of endometrial pathology. However, the endometrium was significantly thicker (mean, 17.9 mm) in patients with endometrial cancer than in those endometrial polyps or hyperplasia. To confirm our findings, it will be necessary to conduct a large-scale, multicenter study assessing endometrial pathology in premenopausal BC patients treated with tamoxifen use.
In conclusion, our study demonstrated that the presence of abnormal uterine bleeding, but not age, BMI, or duration of tamoxifen use, may be the most important factor associated with the occurrence of endometrial hyperplasia or cancer during tamoxifen use in premenopausal women with BC. This finding provides useful information for endometrial surveillance and counseling during tamoxifen use in premenopausal BC patients.

 XML Download
XML Download