

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Bacteroides fragilis group isolates are the most commonly encountered among the anaerobes in clinical specimens and are more virulent and resistant to antimicrobial agents than most other anaerobes.1 Among the B. fragilis group, B. fragilis was most common, followed by B. thetaiotaomicron, B. ovatus, and B. vulgatus.2,3 The taxonomy of Bacteroides has undergone significant changes in the past few years. Recently, several novel Bacteroides species were isolated from the microbiota of human feces. Bakir, et al.4,5,6 reported three novel species, B. finegoldii, B. dorei, and B. intestinalis from human feces in 2006. After that, additional cases of bacteremia caused by B. finegoldii and B. doreii were reported.7 Furthermore, B. nordii and B. salyersiae were first reported in 2004, and both isolates were recovered from human clinical specimens of intestinal origin such as peritoneal fluid, appendix tissue, and intra-abdominal abscess.8 B. faecis was isolated from human feces and was proposed to be a novel species in 2010.9 However, to our knowledge there have been no reported cases of infections caused by B. faecis or B. intestinalis.
In this study, recently identified Bacteroides species, including two cases of B. faecis (case no. 1 and 2) and one case of B. intestinalis (case no. 3), were recovered from clinical specimens of 3 inpatients at a Korean tertiary-care hospital in 2011 (Table 1). A 55-year-old man (case no. 1) with a history of sigmoid colon cancer presented with a high fever of 38.4℃ on the second day after surgery. On the third postoperative day, emergency reoperation was performed after anastomotic leakage was confirmed on an abdominal computed tomography (CT) scan. The patient recovered from peritonitis after treatment with piperacillin-tazobactam for 5 days. Additionally, a 70-year-old man (case no. 2) with a history of rectal cancer presented with a fever of 38.1℃ on the fifth postoperative day. Fluid collection in the pelvic cavity was observed on a CT scan and an intra-abdominal infection was suspected. A course of piperacillin-tazobactam was administered for 9 days, and the fever subsided. Peritoneal fluid cultures of the above two patients were performed when they were febrile.
The patient in case no. 3 was a 65-year-old woman with underlying hepatocellular carcinoma and thyroid cancer. She presented to the emergency department with abdominal pain as well as chills and fever. After admission, empirical treatment with teiocoplanin and imipenem was started for suspected biliary sepsis. Approximately 24 days after admission, an abdominal paracentesis was performed due to her increasing ascites volume. The patient underwent ascites fluid culture and cell count determinations. At that time, an antibiotic was infused once daily, and there was no evidence of high fever.
Peritoneal fluids were inoculated on blood culture medium or conventional culture medium including 5% sheep blood agar, MacConkey agar, phenylethyl alcohol blood agar, and thioglycollate broth. Cultures grew 2-4 bacteria strains including Bacteroides spp. (Table 1). All isolates were identified by Rapid ID 32A (bioMérieux, Marcy-l'Etoile, France) and the VITEK MS (bioMérieux) and matrix-assisted laser desorption ionization (MALDI) Biotyper (Bruker Daltonics, Bremen, Germany) MALDI-time of flight mass spectrometry (MALDI-TOF MS) systems. For further identification of the bacterial species, 16S rRNA gene sequencing was performed. Antimicrobial susceptibility testing was performed using the Clinical and Laboratory Standards Institute agar dilution method as previously described.10,11 Piperacillin and tazobactam (Yuhan, Seoul, Korea), cefoxitin (Merck Sharp & Dohme, West Point, PA, USA), cefotetan (Daiichi Pharmaceutical, Tokyo, Japan), clindamycin (Korea Upjohn, Seoul, Korea), imipenem and metronidazole (Choong Wae, Seoul, Korea), meropenem (Sumitomo, Tokyo, Japan), chloramphenicol (Chong Kun Dang, Seoul, Korea), and moxifloxacin (Bayer Korea, Seoul, Korea) were used.
Two isolates (case no. 1 and 2) were identified as B. faecis by 16S rRNA gene sequencing; however, the Rapid ID 32A system identified the isolates as B. ovatus/B. thetaiotaomicron (Table 2). Additionally, MALDI-TOF MS systems identified B. thetaiotaomicron rather than B. faecis, as the latter species was absent from MALDI-TOF MS databases. The B. intestinalis (case no. 3) isolate was misidentified as B. ovatus with Rapid ID 32A. The VITEK MS system showed B. uniformis, but the MALDI Biotyper did not identify a specific strain. It is difficult to identify the novel Bacteroides spp. isolates by conventional methods using biochemical-reaction and MALDI-TOF MS systems, given that these strains were only recently described and few data have been accumulated on these species. Only 16S rRNA gene sequencing identified the newly discovered species.
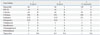
Two B. faecis isolates were susceptible to piperacillin-tazobactam, imipenem, meropenem, moxifloxacin, chloramphenicol, and metronidazole, but non-susceptible to piperacillin, cefoxitin, cefotetan and clindamycin (Table 3). The antimicrobial susceptibility pattern of B. intestinalis (no. 3) isolate was similar to that of the B. faecis isolates in this study, except that B. intestinalis isolate showed nonsusceptibility to moxifloxacin. Antimicrobial susceptibility patterns of Bacteroides spp. isolates in this study were similar to those of B. fragilis group isolates, as shown in previous reports from Korea.11
This is the first report of B. faecis and B. intestinalis strains isolated in clinical specimens. We were unable to demonstrate the clinical significance of B. faecis and B. intestinalis isolates in our patients due to their postoperative status and polymicrobial infections. However, the isolation of anaerobic bacteria from clinical specimens is a necessary cause for concern, as anaerobes detected in polymicrobial infections can occasionally spread to the bloodstream and have serious consequences.
In conclusion, the recently named B. faecis and B. intestinalis isolates were recovered from clinical specimens; thus, it is necessary during the assessment of infections to consider these new Bacteroides spp. isolates as possible causes.


 XML Download
XML Download