

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thyroid ultrasonography (US) is a useful diagnostic tool in the evaluation of thyroid disease including thyroid nodules and diffuse thyroid disease (DTD).1-9 Hashimoto thyroiditis (HT) and Graves disease (GD) are included in DTD, and known US features of DTD are decreased or increased diffuse heterogeneous parenchymal echogenicity, a coarse echotexture, micronodulation, and scattered microcalcifications.4,6,7,10,11 US can provide valuable information on the course of subclinical hypothyroidism (SCH) and is also being used in the evaluation of DTD in patients with thyroid functional abnormality with thyroid autoantibodies such as thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TgAb).5,12,13 Rosário, et al. analyzed 117 patients with SCH, and reported that both diffuse hypoechogenicity on US and the presence of TPOAb increase the risk of SCH developing into overt hypothyroidism.13
US elastography is a newly developed dynamic technique that provides information about tissue hardness by using a degree of distortion under the application of an external force or by using shear acoustic waves remotely induced by a focused ultrasonic beam.14-16 This method has been applied in the differentiation of benign and malignant thyroid lesions.14-17 Previous studies have demonstrated the diagnostic role of US used in DTD diagnosis.5,7 However, to the best of our knowledge, no reports have shown the interobserver agreement of US or the diagnostic performances of shearwave elastography in DTD diagnosis. In this study, we investigated the role of conventional US and shearwave elastography in the diagnosis of asymptomatic patients with DTD.
MATERIALS AND METHODS
Patients
The institutional review board of our institution approved this retrospective study and required neither patient approval nor informed consent for the review of images and records.
This study was performed at our institution (a referral center) during October 2010. During this period, 94 consecutive patients underwent US-fine needle aspiration (FNA). Twenty nine patients were excluded from the original 94 patients because they did not undergo shearwave elastography. Among these patients, 28 patients made the personal choice not to undergo any additional examinations, while 1 patient did not have shearwave elastography performed due to an insufficient amount of underlying thyroid parenchyma being observed as there were multiple nodules in both thyroid glands. Eight additional patients were also excluded because they did not undergo thyroid autoantibody tests. The final study included 57 patients. All patients were initially referred not just for evaluation of thyroid function abnormality, but also for US-FNA on thyroid nodules. Patient age ranged from 26 to 72 years (mean, 49.9 years). Mean age of male patients was 50.4 years (range 44-55 years) and that of female patients was 49.8 years (range 26-72 years).
Conventional US and shearwave elastography of the thyroid
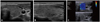
Real-time conventional US and shearwave elastography were performed using a linear transducer with a central frequency of 4 to 15 MHz (ShearWave™ Elastography, Supersonic Imagine, Aix-en-Provence, France). Real-time US was performed by one of three board-certified radiologists with 5 to 13 years of experience in thyroid imaging. First, a careful evaluation of the underlying echogenicity of the thyroid on conventional US was made. After examinations using conventional US, shearwave elastography was performed by the same radiologists who had performed the conventional US. Regions of interest for elasticity images were set to include more than 1/3 of a thyroid lobe for sufficient amount of the underlying thyroid parenchyma and not to include thyroid nodule or nodules on either transverse or longitudinal plane (Figs. 1 and 2). By measuring the speed of shearwave propagation at every point in the image, a quantitative elasticity value was expressed in kilo-Pascals (kPa). We prospectively recorded the quantitative elasticity value of the underlying thyroid gland on shearwave elastography, without considering the US features of the thyroid nodules targeted for US-FNA. Data were entered in a computer database both for patient care and this study.
Thyroid parenchyma was retrospectively analyzed for US features of DTD when the thyroid gland showed one or more of the following suspicious findings: diffuse heterogeneous echogenicity or diffuse hypoechogenicity with/without micronodules, thyroid enlargement [anteroposterior (AP) diameter of thyroid on longitudinal scan >2 cm], multiple linear echogenicity, and scattered microcalcifications6,7,18,19 by three radiologists, (E.J.S, H.J.M, and E.K.K.) with 5 to 13 years of experience in thyroid US independently. They were fully blinded to the serologic test results for all patients. Each blinded reader evaluated the patients' images separately and independently.
Measurement of anti-thyroid autoantibodies
In all patients, thyroid function was evaluated using venous blood samples. Thyroid autoantibodies as well as thyroid function were routinely measured at our institution to evaluate thyroid functional status. Serum thyroid peroxidase antibody (TPOAb), thyroglobulin antibody (TgAb) and thyroid-stimulating hormone (TSH)-binding inhibitory immunoglo-bulins (TBII) levels were measured by radioimmunoassay (Brahms, Hennigsdorf/Berlin, Germany). The existence of each TPOAb and/or TgAb was defined with a serum concentration of thyroid autoantibody >60 IU/L. Patients with HT were defined as those who were positive for TPOAb and/or TgAb.5 Activity of TSH receptor antibody (TRAb) was measured using a first generation TRAb kit prepared by Brahms (Brahms, Hennigsdorf/Berlin, Germany). A value of TBII exceeding 10% was considered positive. Patients with GD were defined as those who were positive for TBII. In this study, we evaluated patients with DTD including both HT and GD.
Statistical analysis
Patient medical records were reviewed for clinical characteristics. The Fisher's exact test was used to compare gender to DTD. We also evaluated the association of age and the values of mean and maximum elasticity on shearwave elastography to DTD using the independent two-sample t-test. Interobserver variability was estimated using the generalized kappa statistic of Landis and Koch.20 The degree of agreement was categorized in terms of kappa values: 0 corresponds to no agreement, 1.00 to complete agreement, less than or equal to 0.20 to slight agreement, 0.21-0.40 to fair agreement, 0.41-0.60 to moderate agreement, 0.61-0.80 to substantial agreement, and 0.81-1.00 to near perfect agreement.20
The diagnostic performances (sensitivity, specificity, accuracy, positive predictive value, negative predictive value) for diagnosing DTD on conventional US were calculated. The area under the receiver operating characteristic curve (Az) was calculated by the three radiologists on conventional US.
We compared the mean and maximum elasticity values between the patients of the DTD group and the patients of the normal serology group. To evaluate diagnostic performances of diagnosing DTD on shearwave elastography, the cut-off value was calculated by using the Youden's index.21 The Az was calculated by using the continuous data of the mean and maximum elasticity.
All statistical analysis was performed with SAS software (version 9.1.3; SAS Institute, Cary, NC, USA). Statistical significance was assumed when the p value was less than 0.05. All reported p values are 2-sided.
RESULTS
Of the 57 patients, DTD was diagnosed in 22 patients using serum TPOAb or TBII. The mean age (50.1±11.6 years) of patients with DTD was older than that (49.7±10.4 years) of patients without DTD (p=0.887). Gender was not associated with DTD (p=0.639).
Reproducibility of conventional US observations was assessed between three observers who analyzed the same images. If only patients diagnosed with heterogeneous echogenicity by all three radiologists were considered, the generalized kappa value was 0.27, which means a fair degree of agreement.
The sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of the three radiologists were 18.2-59.1%, 57.1-94.3%, 57.9-66.7%, 44.4-71.4% and 62.5-69.0%, respectively, on conventional US for the identification of DTD. The Azs were 0.52-0.585 on conventional US by three radiologists. Also, the Azs were not statistically different between the three radiologists (p=0.387) (Table 1).
In the 35 (61.4%) patients consisting of the normal serology group, mean elasticity value was 23.4±10.8 kPa (range, 9.0 kPa to 54.5 kPa), and mean maximum elasticity value was 33.7±12.4 kPa (range, 11.0 kPa to 61.4 kPa). In the 22 (38.6%) patients of the DTD group, mean elasticity value was 24.1±10.0 kPa (range, 9.3 kPa to 53.6 kPa), and mean maximum elasticity value was 36.4±13.3 kPa (range, 15.1 kPa to 70.6 kPa) (Fig. 3). Although the mean values of mean and maximum elasticity were higher in patients with DTD than those in the normal group, there were no statistically significant differences between the two groups (p=0.802 and p=0.452).
The cutoff values of shearwave elastography in DTD diagnosis were 27.6 kPa and 41.3 kPa using the mean and maximum elasticity, respectively. When using the mean elasticity value as a diagnostic criterion for DTD, the sensitivity and specificity were 40.9% and 82.9%, respectively. And when the maximun elasticity value was used as a diagnostic criterion for DTD, the sensitivity and specificity were 40.9% and 77.1%, respectively. Using the mean and maximum elasticity values as a diagnostic criteria for DTD, Az values were 0.619 and 0.59, respectively (Table 1).
DISCUSSION
Shin, et al.5 indicated that thyroid US in SCH has a significant predictive value in treatment outcome, which was comparable to other well-known prognostic parameters such as TPOAb or high TSH levels. Recently, Kim, et al.7 prospectively evaluated the efficacy of thyroid US in the identification of asymptomatic DTD, and concluded that real-time thyroid US is useful in differentiating DTD from normal thyroid parenchyma in asymptomatic patients.
However, US is very subjective and dependent on the performer, which causes interobserver variability between examiners.22,23 There are several reports on the interobserver agreement in US assessment of thyroid nodules.22-25 These reports conclude that if US is performed by experienced radiologists, relatively good agreement can be expected.22-24 However, there were no reports on the interobserver variability of US in the evaluation of echogenicity of the underlying thyroid gland. In this study, fair agreement with a kappa value of 0.26 was observed on the heterogeneous echogenicity on conventional US by three radiologists. This result showed that in diagnosing DTD, conventional US had poor reproducibility even when all images were simultaneously reviewed by three experienced radiologists. Also, diagnostic performances were variable among the observers. The sensitivity, specificity, accuracy, PPV, and NPV of three radiologists were 18.2-59.1%, 57.1-94.3%, 57.9-66.7%, 44.4-71.4% and 62.5-69.0% on conventional US when identifying DTD (Table 1). These results are different from those of other studies.7,26 We speculate that the reasons for the differences7,26 are different gold standards, patient populations, and interobserver variability among radiologists and pathologists. Especially, lymphocytic thyroiditis, of which the pathologic hallmark is lymphocytic infiltration, can show a certain pathologic spectrum, ranging from lymphocytic thyroiditis only to atrophic and eosinophilic change of thyroid cells with fibrosis.27 Depending on which stage of lymphocytic thyroiditis is being observed, there will be variations in diagnostic performances that will, in turn, affect the results. Therefore, the pathologic stage of disease is thought to be a important factor that decides what kinds of results US elastography obtains.
US elastography is based on the deformity formed by external compression,17 and the diagnostic performances of US elastography in general greatly depend on the quality of the freehand compression applied.28 Shearwave elastography is a technique which characterizes tissue structure by using shear acoustic waves remotely induced by a focused ultrasonic beam.29 Because shearwave elastography produces the radiation force in the probe, this may be more reproducible than conventional elastography, in which radiating force is produced by repetitive external compression by an operator.16 Furthermore, shearwave elastography shows quantitative tissue elasticity within a given region of interest.30 This reproducibility and quantitative information are very useful advantages of shearwave elastography. In the present study, we performed a quantitative measurement of thyroid tissue stiffness employing shearwave elastography, using mean and maximum elasticity values, and found that the mean values of mean and maximum elasticity in patients with DTD were not significantly different from those in the normal group (mean 24.1±10 kPa versus 23.4±10.8 kPa and maximum 36.4±13.3 kPa versus 33.7±12.4 kPa, respectively, p=0.802 and p=0.452) (Table 1). The specificity was higher when the mean elasticity value was used instead of the maximum elasticity value, however, the sensitivities of shearwave elastography were same when both indices were used in diagnosing DTD.
Our study has some limitations. First, the number of patients included in our study was relatively small to generalize reproducibility of conventional US and diagnostic performance of shearwave elastography. Future studies with larger populations are needed. Second, final diagnosis of the patients included in this study was based on the serologic levels of autoantibodies. False-negative and false-positive serologic results might have an effect on our results, nevertheless, they were not considered. Third, this study was a retrospective analysis to evaluate a reproducibility of conventional US between three observers using only static captured images. To resolve and validate our result, real time US might be helpful in further studies. Lastly, this study did not evaluate diagnostic performances of US and elastography according to pathologic spectrum of DTD. For example, hepatitis has variable US results, depending on liver fibrosis stage, because stiffness changes by stage.31 Thus, for a more insight, studies are needed on how US elastography results vary by pathologic stages of DTD to understand the full potential of its practical use. In conslusion, conventional US did not show a reliable interobserver agreement in the diagnosis of DTD. Although not statistically significant, shearwave elastography may provide additional information for the diagnosis of DTD. Therefore, larger prospective studies are needed to define the values of shearwave elastography in diagnosing DTD.



 XML Download
XML Download