

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prompt screening of high risk subjects for PTSD following major traumatic events is essential. However, most acute care workers treating traumatized victims usually have little expertise in psychological trauma, and are rarely trained to identify survivors at high risk for PTSD. Several reports suggest that early intervention in high risk populations, such as with cognitive behavioral therapy, may help prevent later aggravation of PTSD symptoms.1,2
Unlike measures used for diagnostic purposes, PTSD screening instruments should have simple rules for ruling in or ruling out, be relatively brief, and easy to administer. Furthermore, they should contain a minimal number of items and alternative scale points, use language that is easily understood by both respondents and non-specialists, and have content that is acceptable to respondents, with minimal stigma or labeling.3 A number of screening tools have been developed to assess PTSD symptoms, such as the Impact of Events Scale (IES),4 the Mississippi Scales for Combat and Non-combat,5 the Short Form of the Mississippi Scale,6 the Post-traumatic Stress Diagnostic Scale (PDS),7 the Davidson Trauma Scale (DTS),8 the Trauma Screening Questionnaire (TSQ),9 and the SPAN.10
The SPAN is a four-item screening measure for PTSD derived from the DTS. The SPAN consists of four symptom items - Startle, Physiological arousal, Anger, and Numbness. Because scores on individual DTS items were highly inter-correlated, Meltzer-Brody, et al.10 developed a shorter four-item version and evaluated its diagnostic accuracy in a sample of 243 patients. They reported favorable screening performance of the SPAN that was comparable with the original DTS. Other studies evaluating the SPAN's psychometric properties also reported high diagnostic accuracy when screening early trauma survivors.11,12 These results suggest that the SPAN has a comparable efficacy to longer questionnaires but with the advantages of simplicity and brevity. This study aimed to develop a Korean version of the SPAN (SPAN-K). We assessed the reliability and validity of SPAN-K and examined its diagnostic accuracy.
MATERIALS AND METHODS
Subjects
This study was approved by the Institutional Review Board of St. Mary's Hospital and The Catholic University of Korea. The subjects were PTSD patients (PTSD group), patients with non-psychotic mood or anxiety disorders (psychiatric control group), and healthy participants (normal control group). Patients and healthy controls between the ages of 18 and 65 years were recruited from 18 psychiatric institutes across Korea. Diagnosis of PTSD and other psychiatric disorders was performed via the Mini International Neuropsychiatric Interview (MINI)13 using DSM-IV criteria.
The Korean version of MINI underwent a validation study and was shown to have good reliability and validity.14 The kappa value of major depression was 0.74 and those of anxiety disorders were ranged from 0.62 to 0.81.14 The psychiatric control group included patients with major depressive disorder, panic disorder, generalized anxiety disorder, phobic disorder, adjustment disorder, and undifferentiated somatoform disorder. Healthy controls participated in a semi-structured interview to confirm they had no lifetime history of psychiatric and medical disorders. All procedures were explained in detail; the study participants were volunteers and gave informed consent.
Assessment instruments
The SPAN consists of four items taken from the DTS.8,10 The original DTS is composed of 17 items related to PTSD symptoms, as listed in the DSM-IV, and was designed to assess the severity and frequency of PTSD symptoms. The DTS has been applied to a wide range of populations and types of trauma, and is sensitive to treatment-induced symptom changes.8,15 The SPAN assesses the severity of four symptoms - 'Startle' (DTS item 17), 'Physiological arousal' (DTS item 5), 'Anger' (DTS item 14), 'Numbness' (DTS item 11) - using five-point Likert scales ranging from 0 (not at all distressing) to 4 (extremely distressing). The SPAN-K was adapted from the DTS-K, which was translated into Korean with the back-translated content.16 The reliability and validity of the DTS-K have been previously reported, and the scale has an internal consistency of 0.97. We used the Clinician-Administered PTSD Scale (CAPS)17 and the State-Trait Anxiety Inventory (STAI)18 to analyze the concurrent validity of the SPAN-K. The CAPS is a structured clinical interview designed to examine seventeen core symptoms of PTSD that cover the B, C, and D criteria of the DSM-IV, in addition to symptoms commonly associated with PTSD, such as guilt and dissociation.17 This scale assesses the severity and frequency of symptoms, and their impact on overall functioning. There are several versions of CAPS based on the time period of assessment, such as the CAPS-1, which is the current and lifetime diagnostic version, and the CAPS-2, which is the 1 week symptom status version. We used the CAPS-1 to further examine SPAN-K concurrent validity. The Korean version of CAPS has a high internal consistency value of 0.95.19 The State-Trait Anxiety Inventory (STAI)18 is a self-reporting questionnaire designed to evaluate the severity of anxiety symptoms. It consists of 20 questions for measuring temporary or state anxiety and 20 questions regarding chronic or trait anxiety. The Korean version of STAI (STAI-K) has excellent psychometric properties and an internal consistency of 0.91.20 The raters in this study were seven experienced, board-certified psychiatrists. They participated in formal consensus meetings that consisted of reviews about evaluation tools to be used in this study, observing the administration of CAPS by an experienced supervisory psychiatrist, and videotaped administrations featuring standard PTSD patients. The interrater reliability of the Korean version of CAPS was high, with an intraclass correlation coefficient of 0.76.
Data analysis
Kruskal-Wallis test and χ2 analyses were used to compare continuous and categorical variables, respectively, between groups. The Mann-Whitney test was used for post hoc analysis. The internal consistency of SPAN-K was evaluated by calculating Cronbach's α coefficient. Test-retest reliability was estimated by Spearman's correlation coefficient of SPAN-K scores obtained two weeks apart. The concurrent validity of the SPAN-K was estimated by Spearman's correlation coefficient with other clinical measures, including the CAPS, DTS, and STAI. Test sensitivity (the probability that someone who is diagnosed with PTSD will have had a positive test result), specificity (the probability that someone who is not diagnosed with PTSD will have had a negative test result), positive predictive value (PPV, percentage of patients with positive test results who are diagnosed with PTSD), negative predictive value (NPV, percentage of patients with negative test results who are not diagnosed with PTSD), and efficiency (overall percentage of correct classification) were calculated for all possible cutoff scores. To determine the accuracy of SPAN-K discrimination, receiver operating characteristic (ROC) analysis was applied using PTSD diagnosis via MINI, and the area under the curve (AUC) was calculated using standard formulae.
RESULTS
Demographic and clinical characteristics
A total of 254 subjects were recruited into the study (Table 1), including 93 PTSD patients (PTSD group), 73 patients with non-psychotic mood or other anxiety disorders (psychiatric control group), and 88 healthy participants (normal control group). The mean participant age was 44.9 (SD, 15.7) in the PTSD group, 44.6 (SD, 14.6) in the psychiatric control group, and 43.0 (SD, 13.2) in the normal control group. There were 45 women in the PTSD group (48.4%), 45 women in the psychiatric control group (62.5%), and 38 women in the normal control group (43.2%). No significant differences in age, sex or marital status were found between groups; however, there were significant group differences in economic status (χ2=10.48, p=0.026).
Among PTSD subjects, the mean duration of symptoms was 5.4 years (SD, 10.9; range, 0.1-52.0 years). The most significant trauma experienced by the subjects included car accidents or other man-made disasters (n=54, 58.1%), physical assault (n=11, 11.8%), combat experience (n=7, 7.5%), imprisonment (n=4, 4.3%), sexual assault (n=3, 3.2%), disease (n=2, 2.2%), and witnessing an accident (n=1, 1.1%). Eleven subjects described their worst trauma as of a mixed nature.
Internal consistency and test-retest reliability
Cronbach's α of the SPAN-K was 0.80 in the 93 subjects with PTSD. Test-retest reliability was examined in 65 respondents who reported no change in symptoms in the two-week interval. The correlation coefficient of the two trials was 0.80 (p<0.001).
Concurrent validity
The mean SPAN-K scores were 10.06 (SD, 4.20; median score, 12; range, 0-16) for the PTSD group, 4.94 (SD, 5.00; median score, 4; range, 0-16) for the psychiatric control group, and 1.42 (SD, 1.87; median score, 1; range, 0-11) for the normal control group (Fig. 1). The PTSD group had significantly higher SPAN-K scores compared with the psychiatric and normal control groups (Kruskal-Wallis test, F=107.96, p<0.001; post hoc test, vs. psychiatric control group, p<0.001; vs. normal control group, p<0.001).
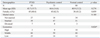
We also assessed the convergent and divergent validity of SPAN-K with other scales in the PTSD group (Table 2). The correlation coefficients were 0.86 for SPAN-K vs. DTS-K scores (n=93, p<0.001) and 0.87 for SPAN-K vs. CAPS total scores (n=48, p<0.001). Additionally, the correlation coefficients were 0.31 and 0.42 for SPAN-K vs. STAI-S and STAI-T, respectively.
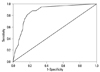
ROC analysis
Fig. 2 shows the SPAN-K ROC curve. SPAN-K score generally showed good diagnostic capacity, with an area under the curve (AUC) of 0.87 (95% CI 0.82-0.91). Table 3 shows six different cutoff scores and their sensitivity, specificity, PPV, NPV, and efficiency, evaluated according to PTSD diagnosis with MINI. A cutoff score of 7 yielded the highest efficiency, with a sensitivity of 0.83 and a specificity of 0.81. The positive and negative predicative values at the cutoff score of 7 were 0.88 and 0.73, respectively.
DISCUSSION
Here we report that SPAN-K demonstrated good reliability and validity, as well as overall diagnostic accuracy, and was comparable to the original SPAN. Cronbach's α of the SPAN-K was 0.80 in the current study, which was lower than the value of 0.97 obtained for the DTS-K. This suggests that the SPAN-K had less internal consistency than the DTS-K, which may be attributable to the fact that the selection of items reflects different types of PTSD symptoms from the DTS-K. A previous report revealed that the Chinese version of SPAN (SPAN-C) had a Cronbach's α value of 0.77.11 The ideal value for Cronbach's α is thought to be between 0.70 and 0.90, as values over 0.90 indicate that many items address the same question in different ways.11,21,22 The test-retest reliability of the SPAN-K was 0.80 over a 2 week interval. Although this value is lower than that reported for the SPAN-C (0.90 over a 1 week interval), this result is generally satisfactory, considering that a 2 week interval is a relatively long period over which to expect no change in symptoms. The results regarding concurrent validity suggest that the SPAN-K has substantial specificity for PTSD. In the current study, correlation analysis revealed a strong correlation between the SPAN-K and CAPS (r=0.87), which was comparable to that between DTS-K and CAPS (r=0.87). The SPAN-K also showed a significant correlation with the DTS-K (r=0.86). The correlation between SPAN-K and STAI was also significant, but weaker than that of CAPS and DTS-K (r=0.31 for STAI-S and r=0.42 for STAI-T). This weak correlation with STAI could be associated with anxiety and depression, which are easily comorbid with PTSD.2
The SPAN-K showed good diagnostic accuracy according to the ROC analysis, with an AUC value of 0.87. The AUC is an overall index of the discrimination accuracy of diagnostic measures, and AUC values of above 0.85 are generally considered to reflect good diagnostic capacity. Supporting our results, in a prospective study, Sijbrandij, et al.12 reported an AUC value of 0.89 for the original version of the SPAN.
SPAN-K had the best diagnostic efficiency (82%) with a cutoff point of 7. This cutoff point is slightly higher than the score of 5 used in both the original version of SPAN and the SPAN-C.10,11 The upward shift in cutoff scores in our study may reflect the need to distinguish PTSD patients not only from normal controls but also from other psychiatric patients. The difference in mean SPAN-K scores between the three groups supports this hypothesis (Fig. 1). SPAN-K efficiency was also comparable with the original SPAN and SPAN-C, which had maximum efficacies of 87% and 80%, respectively.10,11 SPAN-K sensitivity and specificity (0.83 and 0.81, respectively) as well as PPV and NPV (0.88 and 0.73, respectively) were also globally satisfactory at the cutoff score of 7. However, the cutoff score is not absolute and can vary in different clinical situations according to the criteria used to define the case, the timing of assessment, and the severity of the disorder in the study population.23 A previous prospective study using the SPAN yielded an optimal cutoff score of 10, with a sensitivity of 0.86 and a specificity of 0.86. However, the NPV in this study was 0.22, a very low value compared with those obtained by Meltzer-Brody, et al. (0.87), the SPAN-C (0.85), and the SPAN-K in our study (0.73).10,11 This low NPV value may contribute to the low prevalence rate of 4.7% reported in that study; all other studies using SPAN variants reported prevalence rates greater than 35%. Screening tools where cutoff values are set to obtain high specificity, even with moderate sensitivity, are particularly useful when prevalence is high because they can identify subjects requiring more intensive assessment.24 Additionally, highly sensitive tests with moderate specificity are still useful even when prevalence is low, as they can exclude the individuals who do not require further assessment. It is important to set cutoff thresholds that maintain a reasonable balance between sensitivity and specificity; further studies in other populations will help determine the optimal cutoff value for the SPAN-K.
Comparison of SPAN-K and DTS-K in the same population revealed the AUC to be 0.87 and 0.90, the sensitivity to be 0.83 and 0.87, and the specificity to be 0.81 and 0.84 for the SPAN-K and DTS-K, respectively.16 These findings suggest that the SPAN-K is comparable with the DTS-K, its simple composition notwithstanding. Previous studies also support this finding; though assessed in different patient populations, the efficiency and specificity at the cutoff score were 0.88 and 0.91 for the original SPAN, and 0.83 and 0.95 for the original DTS.8,10 Moreover, the efficiency and specificity were 0.80 and 0.80 for the SPAN-C and 0.85 and 0.81 for the DTS-C in the same study population.11,15 In a prospective study, Sijbrandij, et al.12 found that SPAN had an even higher specificity than DTS in the same study population. Taken along with other prior reports, these data strongly suggest that brief screening measures can perform as well as longer-term instruments.9,25,26 Furthermore, our current results also suggest that screening instruments evaluating a subset of PTSD symptoms have the advantage of brevity, while maintaining accuracy, as compared to those attempting to evaluate all PTSD symptoms.
Our study has some limitations, which necessitate cautious interpretation of the data. Although it is advantageous that our study sample includes patients with various types of trauma, our current data cannot fully assess the prognostic accuracy of SPAN-K because of the limitation of its cross-sectional design. To fully utilize the advantages of SPAN-K in the clinical practice, the predictive usefulness of SPAN-K should be confirmed from prospective studies using a homogeneous population with same trauma at the initial phase. A non-randomized sampling process might also affect the reliability of results that are sensitive to the prevalence in the population, such as PPV and NPV.24 In addition, the SPAN-K was not administered as a separate questionnaire but was rather derived from the DTS-K, similar to previous studies.10-12 The presence of other items during assessment might influence SPAN-K scoring due to contextual effects. Although the utility of independent SPAN administration was confirmed in a recent study, further validation of the SPAN-K is required in the future.27
In conclusion, our results indicate that the SPAN-K has acceptable psychometric properties and may constitute a promising alternative to relatively long questionnaires for screening for PTSD risk in Korean patients with trauma. Further studies are needed to prospectively evaluate SPAN-K diagnostic accuracy, and to compare the screening ability of SPAN-K with that of other commonly used screening measures.



 XML Download
XML Download