

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastroesophageal reflux disease (GERD) is a disease caused by chronic exposure of the esophagus from retrograde flow of gastric juice and/or duodenal contents, which noticeably deteriorate patient's quality of life. It is a well known pathologic condition in Western countries with a prevalence ranging from 25 to 27%.1,2 Because the term "heartburn" has no identical counterpart in the Korean language, its symptomatology is poorly defined by patients and probably less recognized by physicians, however, the prevalence of this disease in Korea is thought to be around 7.1 to 14.6%,3,4 mostly as a result of "westernized" life styles. Heartburn, regurgitation, and dysphagia are typical symptoms of this entity, but in a minority of patients, atypical or extraesophageal symptoms, such as hoarseness, throat pain, globus sensation, cough, and bronchial asthma appear.5 A characteristic of this entity in Asian populations is that atypical symptoms are more frequent than Western patients, the reasons for which are not completely understood.6 The aim of this study is to analyze our experience with laparoscopic Nissen fundoplication.
PATIENTS AND METHODS
From Sep. 2003 to Mar. 2008, 31 adult Korean patients diagnosed with GERD underwent laparoscopic Nissen fundoplication at our institution. Indications for surgery were patients with failed medical therapy, frequent recurrences in spite of medication, particularly if dose escalation was required, laryngopharyngeal and/or respiratory symptoms, complications of GERD, such as esophageal stricture, erosive esophagitis, esophageal ulcer, and/or Barrett's esophagus. Patients were referred from gastroenterologists, otorhinolaryngologists, or came directly for consultation to our Department. All patients were taking antireflux medications, including proton pump inhibitors. Preoperative studies consisted of upper gastrointestinal endoscopy, esophagogram, esophageal manometry, and ambulatory 24-hour esophageal pH monitoring.
Three hundred sixty degree laparoscopic Nissen fundoplication was carried out in all patients. Briefly, a 5-port technique was used with two 10-mm trocars and three 5-mm trocars (Fig. 1). Division of phrenoesophageal ligament allowed us to obtain at least 3 cm of abdominal esophagus, and crural closure was done using 2 or 3 stitches using #2-0 non-absorbable suture materials (Ethibond®, Ethicon, Somerville, NJ, USA). After division of short gastric vessels, complete mobilization of fundus was achieved and "shoeshine" maneuver was done for verification undue tension of the wrap. Thereafter, a floppy and short wrap of approximately 2 cm in length, guided by the metallic part of a laparoscopic instrument, was constructed over the esophagogastric junction with a bougie placed in the esophagus with the above mentioned suture materials (Fig. 2). Size of the bougie ranged from 50 to 54 Fr., according to patient's body type. At the end of the procedure, a laparoscopic grasper was introduced underneath the wrap to verify whether it was floppy.
Patients' demographics, symptoms, results of preoperative studies, operative data, postoperative complications, and surgical outcomes were collected from medical records. Data were analyzed using SPSS software (SPSS, ver. 12.0, Chicago, IL, USA). Chi-square test or Fisher's exact test was used for comparison, as needed. A p value less than 0.05 was considered as statistically significant. Results were expressed as mean ± SD.
RESULTS
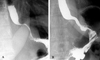
There were 19 males and 12 females with an average age of 46.8 ± 17.0 years. Mean time of duration of symptoms was 9.0 ± 10.6 years. Median duration of antireflux medications, including proton pump inhibitors, was 5 years (range from 4 months to 20 years). Typical symptoms were present in 15 patients (48.4%), and atypical symptoms in 16 (51.6%). Both typical and atypical symptoms were present in 4 patients (12.9%). Preoperative studies showed hiatal hernias (type I) in 13 patients (41.9%). Barrett's esophagus was present in 10 (32.3%), and reflux esophagitis in 18 (58.1%). Mean preoperative DeMeester score was 17.4 ± 16.7. Fourteen patients (45.2%) had history of previous abdominal surgeries, and two patients among those had cholecystectomies. One patient underwent concomitant laparoscopic cholecystectomy. Mean operative time was 206.1 ± 47.8 min, and mean hospital stay 5.2 ± 2.1 days. Perioperative complications occurred in 5 patients (16.1%), including 1 major, 2 moderate, and 2 minor complications. Major complication was gastric perforation due to forceful insertion of bougie. Two moderate complications were atelectasis and prolonged ileus. Two minor complications were subcutaneous emphysemas. There was no conversion to open surgery and no mortality was observed. Mean follow-up period was 13.3 ± 16.7 months, ranging from 4 to 30 months. Gastroesophageal junction stenoses causing dysphagia that required subsequent endoscopic balloon dilations were present in 5 patients (16.1%). After dilatation, postoperative dysphagia was controlled in nearly all patients. In 1 out of 5, dysphagia was not controlled completely, therefore, subsequent repeated dilatation was necessary for relief of symptom (Fig. 3).
After surgery, GERD symptoms were completely controlled in 16 patients (51.6%), partially controlled in 13 (41.9%), and not controlled in 2 (6.5%). Overall symptomatic improvement was observed in 29 patients (93.5%) (Table 1). Nine patients (29%) were again on proton pump inhibitor regimen due to objective or subjective reflux symptoms.
When subdivided by type of preoperative symptoms (typical or mixed symptoms vs. atypical symptoms only) and analyzed according to symptomatic improvement (complete or partial symptom control vs. no symptom control), no statistical difference in surgical outcome was found (p > 0.05). When analyzed the surgical outcome based on the presence of hiatal hernia, no statistical difference in symptomatic improvement was found between groups (p > 0.05). Similarly, no statistical difference was found between those with and without Barrett's esophagus. The presence of reflux esophagitis did not influence the outcome as well (Table 2).
DISCUSSION
Evidence of laparoscopic antireflux surgery is scarce in Korea, and the first report of laparoscopic fundoplication in adult was published in 1996.7 Reasons for the scarcity of laparoscopic fundoplication is that medical treatment with proton pump inhibitors is regarded as the mainstay of treatment in Korea, and surgical options for treating GERD is not well known, even for many surgeons. We have noticed a similar situation in our neighbor country, Japan, where the disease pattern is quite similar.8 To our knowledge, this is the largest series recruited to date in our country.
In concordance with other Asian authors,6 the prevalence of atypical symptoms was predominant in our series. In a study from the UK, the predominance of atypical symptoms was 21.2% and the surgical outcome in the majority of patients with atypical symptoms was effective.8 In our experience, patients with only atypical symptoms showed complete symptom control in 47.1%, partial symptom control in 41.2%, and no symptom control in 11.8%. It is noteworthy that the 2 patients in whom the surgery had no effect were those having atypical symptoms only. Therefore, patients with only atypical symptoms should be carefully evaluated, including full otorhinolaryngologic evaluation to exclude entities other than GERD.
Some of the complications pertaining to surgery were preventable, such as gastric perforation due to forceful insertion of bougie by the anesthesiologist. We suture-closed the perforation site laparoscopically and the patient had an uneventful recovery. Allowing anesthesiologist to watch the passage of the bougie on the laparoscope monitor during its insertion and to discuss the position of the bougie with surgeon should minimize the risk of perforation. Subcutaneous emphysemas covering up to the neck were developed in 2 patients, who were self-limited and managed conservatively, however, we did not see any case of pneumothorax in spite of taking chest x-rays in immediate postoperative setting.
As a mid- to long-term complication, dysphagia becomes a problem. As fundoplication per se brings the problem of dysphagia, we adopted a wait-and-watch attitude and reassurance for dealing this problem. Many patients were relieved from symptoms after a dietary counseling on soft meals. Those patients with persistent symptoms underwent endoscopic balloon dilatations. Four of 5 patients were relieved from symptoms, nonetheless, 1 patient complained of persistent dysphagia and underwent a second endoscopic session approximately 3 months after the first dilatation. Luckily, we did not have to surgically revise this patient, and the patient is now tolerating regular diet well. Other common side effects of the surgery include inability to belch and gas bloating, which are very debilitating sometimes. For some patients, these symptoms are so disturbing that they even wish to have the surgery reversed. Fortunately, dietary counseling with the addition of antiflatulents, such as simethicone and prokinetic agents, is usually useful for ameliorating these complaints.
Contrary to some authors, who advocate partial fundoplication when esophageal dysmotility is encountered,9,10 our belief is that complete fundoplication works well for those with either normal or impaired esophageal motility. Studies comparing total vs. partial fundoplication support our belief.11,12 In our series, 2 patients had abnormal esophageal motility and both patients underwent complete fundoplication with satisfactory outcomes. One of these patients was suffering from scleroderma and symptoms were relieved after fundoplication, however, persistent dysphagia was noted, for which endoscopic balloon dilation was required. Watson et al. reported 6 patients with systemic scleroderma who underwent laparoscopic fundoplications; four complete types and 2 partial types with an acceptable outcome.13
Long-term outcome of fundoplication is much debated. This is even truer nowadays, when less invasive endoluminal technologies are available.14 The limitation of our study is that the number of patients is small and follow-up period is relatively short. Studies with a larger number and longer follow-up period are expected to show favorable outcome of fundoplication. Long-term patient's satisfaction rate ranged from 43 to 71% and percentage of patients taking antireflux medication was 21 to 43%.15,16 Similarly, 9 patients (29%) in our series were taking proton pump inhibitors again due to objective or subjective reflux symptoms. A randomized clinical trial comparing proton pump inhibitors with surgical treatment demonstrated that surgery was more effective in controlling overall symptoms.17
In conclusion, laparoscopic Nissen fundoplication in our experience is an efficacious method of controlling symptoms of GERD in Korean patients, even for those who have atypical symptoms. Since our experience is still limited, a study of larger scale could define more clearly the efficacy of this treatment modality.




 XML Download
XML Download