

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The QT interval, measured from the beginning of the QRS complex to the end of the T wave on a standard ECG, represents the duration of the action potential of heart ventricles.
The corrected QT interval (QTc) varies with the heart rate (HR). Faster HR (the shorter the RR interval) results in a shorter QTc, and vice versa. Therefore, the QTc is usually corrected for HR using Bazett's formula (QTc = QT/√RR, with all intervals in seconds) which remains the gold standard for clinical use despite some limitations at particularly fast or slow HRs. Sevoflurane, desflurane, thiopental and propofol have been shown to prolong the QTc intreval.1,2 In healthy patients, this prolongation seems to have no harmful effects. However, those who are at risk, including those suffering from hypokalemia, those with a genetic predisposition or those who have taken two or more drugs that lengthen QTc, may be predisposed to fatal ventricular arrhythmia.3
Fentanyl, the mu(µ)-opioid agonist, is the most frequently used opioid in anesthesia. Review of literature has shown that fentanyl interferes with K+ currents in human cardiac cells transfected with the human ether-a-go-go-related gene (HERG) potassium channel gene,4 and that fentanyl may shorten the QTc in congenital long QT syndrome as well as in healthy patients.5,6
Remifentanil, the most recently released opioid agonist, is widely used in anesthesia because of its desirable pharmacokinetic property, specifically in the field of day case anesthesia. Remifentanil induces a dose-dependent decrease in HR, arterial blood pressure and cardiac output.7 However, there are few reports describing the effect of remifentanil on QTc changes during anesthesia.8,9
One microgram per kilogram of remifentanil was shown to reduce the prolongation of QTc following laryngoscopy and intubation in one study.8 However, the efficacy of remifentanil in attenuating QTc response to laryngeal mask airway (LMA) insertion is unknown.
Therefore, the aim of this study was to investigate the effects of a single bolus of remifentanil administered prior to LMA insertion on QTc interval during sevoflurane induction in healthy, unpremedicated women undergoing minor gynecological day case surgery in a placebo-controlled, randomized, double-blinded study environment.
MATERIALS AND METHODS
After obtaining approval from the Hospital Research Ethics 334Committee, women of American Society of Anesthesiologists physical status 1 (ASA PS1), aged between 25 and 49 years, and scheduled for elective gynecological day case surgery were included in the study and upon receipt of their written informed consent. All of the surgeries were performed between 8:00 a.m. and 11:00 a.m. to minimize the influence of the circadian variation in cardiac autonomic nervous activity. Patients were excluded from the study if any of following criteria were present: 1) use of any QT-prolonging drug for 14 days; 2) idiopathic or acquired prolonged QT interval in preoperative ECG (QTc > 440 ms); 3) existence of arrhythmia, bundle branch block pattern or preexcitation; 4) structural heart disease; 5) endocrine disorder; 6) malignancy; 7) electrolyte abnormality; 8) obesity (body mass index > 30); 9) pregnancy; 10) contraindications for the use of LMA.
The patients were randomly placed into one of the two groups based on a computer-generated sequence of numbers. Fig. 1 provides a summary of the study protocol.
No anti-cholinergic drugs were given because they can cause increases in the QT interval. Vital signs were measured when the patients arrived in the operating room, which included ECG monitoring, non-invasive arterial pressure and pulse oximetry. After 10 minutes of stabilization, digitalized 12-lead ECGs were recorded on a Philips Pagewriter (Pagewriter Trim III, Philips, Netherlands) that simultaneously acquired the 12-lead readings for 10 seconds at a sampling rate of 100 Hz with a resolution of 5 µV
The anesthetic circuits were pre-filled with 5% sevoflurane for 3 minutes. All patients received pre-oxygenation for 3 minutes with 6 L min-1 oxygen from another oxygen source. Then patients exhaled residual volume and took three maximum vital capacity breaths of a gas mixture of sevoflurane through a mask connected to the pre-filled anesthetic circuit, as they had previously been instructed. Thereafter ventilation was assisted with positive pressure ventilation to keep the end tidal CO2 between 30-35 mmHg. After loss of eyelash reflex, 0.05 mg.kg-1 of vecuronium was given to facilitate the insertion of LMA. After 2 minutes of induction, the remifentanil group received 0.25 µg.kg-1 of remifentanil in 10 mL of saline over a 30 second period, and the placebo group received the same volume of saline. The remifentanil dose was chosen based on doses from our preliminary studies. The inspiratory concentration of sevoflurane was set at 2%. 1 minute after administration of the study drug an anesthesiologist who was blinded to the study inserted the LMA. If insertion was not completed within 40 seconds, the patient was excluded from further study. The QTc, HR and mean arterial pressures (MAP) were noted at the following stages: pre-induction, 2 minutes after sevoflurane induction, and 1 and 3 minutes after LMA insertion. Hypotension (Systolic arterial pressure < 80 mmHg for > 60 s) was treated with IV administration of 3 mg of ephedrine. Bradycardia (HR < 45 beat min-1 for > 60 s) was treated with 0.5 mg dose of atropine after QTc data collection. The case was excluded from the study if rescue drug had to be given before completion of the study period. Once the study was completed, the surgery was allowed to proceed and anesthesia was maintained with sevoflurane.
QT intervals were estimated manually from the onset of the QRS complex to the end of the T wave (defined as the junction of the isoelectric line and the tangent of the maximal downward limb of the T wave) by a cardiologist who did not aware of study group assignment. QTc values were calculated according to Bazett's formula. Percentage of patients with prolonged QTc over 450, 480 and 500 ms in both study groups were compared.10
The data were analyzed by GraphPad Prizm version 5.0 for Windows (San Diego, CA, USA). The variables were expressed as mean ± SD. A sample size of 14 patients per group was necessary based on calculations with 80% power (p = 0.05, β = 0.2) to detect a mean QTc interval difference of 22 ms between groups and a standard deviation of 20 ms using a t-test. Intergroup comparisons were performed using Student's t-tests or Chi-square tests for independent data. Differences within groups were evaluated using repeated measures ANOVA with post-analysis of the Dunnett test. A p value of < 0.05 was considered to be statistically significant.
RESULTS
Forty-six patients were recruited to participate in this study. In the remifentanil group, two patients were excluded due to the need for more than one attempt at LMA insertion, and one was excluded due to the use of rescue drugs before obtaining an ECG curve. In the placebo group, two patients were excluded due to prolonged LMA insertion time, and one was excluded because of the poor quality of the ECG curve obtained. Therefore, both groups consisted of twenty patients at the end of the study.
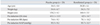
The patients in both groups were comparable in age, weight, height, pre-induction HR, pre-induction MAP and pre-induction QTc (Table 1).
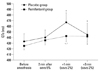
In the placebo group, significant increases in QTc values were observed one minute after LMA insertion as compared to the values obtained before anesthesia and to the corresponding time points in the remifentanil group (467.8 ± 16.5 vs. 442.7 ± 21.3 ms, p < 0.001)(Fig. 2). Three minutes after LMA insertion, the QTc values remained prolonged as compared to the corresponding baseline values in both groups. The numbers of patients with QTc prolongation over 450 ms in each study group are compared as shown in Table 2. In the remifentanil group, there were significantly fewer patients with prolonged QTc of over 450 ms. In the placebo group, QTc values > 480 ms were noted in four patients. In remifentanil group, QTc values > 480 ms were noted in two patients. There were no observations of QTc values > 500 ms in either group.
HR in the placebo group was significantly higher at one minute after insertion of LMA than before administration of anesthesia (p < 0.05)(Fig. 3). In the remifentanil group, HR was significantly lower at 1 and 3 minutes after LMA insertion than before anesthesia administration (p < 0.05).
MAP decreased significantly 2 minutes after sevoflurane anesthesia in both groups, compared with the values before anesthesia (p < 0.05)(Fig. 4). In the remifentanil group, MAP was significantly lower one minute after LMA insertion than before anesthesia administration, whereas MAP had increased significantly in the placebo group.
In both groups, MAP values returned to the pre-anesthesia values within 3 minutes after LMA insertion.
DISCUSSION
The main purpose of this study was to evaluate the addition of a small dose of remifentanil before LMA insertion during inhalation induction with 5% sevoflurane in terms of its effects on QTc intervals and hemodynamic effects. Because LMA insertion is far less stimulating than direct laryngoscopy and endotracheal intubation,11 LMA may be a more desirable airway instrument for patients with known long QT syndrome (LQTS) who may present for incidental minor surgery or may require anesthesia for insertion of a pacemaker or implantable automatic defibrillator.
A few studies have investigated the effect of this relatively new opioid agonist, remifentanil, on QTc intervals. Kweon, et al.8 reported that 1 µg.kg-1 of remifentanil is effective in preventing intubation- related QTc prolongation in healthy patients. Continuous infusion of 0.1 µg.kg-1min-1 of remifentanil has been shown to prevent fatal arrhythmia in patients with a long QT syndrome.9 In an animal study, remifentanil depressed sinus node and AV nodal function, but it did not affect QTc at doses typically used in clinical settings.12
In this study, we tried to evaluate the efficacy of low dose remifentanil in attenuating QTc intervals during LMA insertion with sevoflurane induction.
The remifentanil dose required to facilitate LMA insertion has been estimated to be 0.25 to 0.3 µg.kg-1 in association with propofol, without the need for neuromuscular blocking agents.13,14
Suzuki, et al.15 reported that taking multiple deep breaths of 5% sevoflurane with 67% N2O was comparable to 2 mgkg-1 of propofol for insertion of LMA. Our pilot studies suggested that the lowest dose of remifentanil prevents unwanted bradycardia.
In this study, we used three vital capacity breaths with the priming circuit technique as the inhalation induction method because it provided faster induction time as compared to the conventional stepwise increase in the dose of sevoflurane.16 A rapid method may be more practical in a busy day surgery unit setting because it requires only a few minutes to establish adequate anesthetic depth for airway instrumentation.
There are reports in the literature analyzing various measures for preventing increases in QTc following tracheal intubation. Lidocaine, esmolol, fentanyl, alfentanil and remifentanil have been studied in this capacity.6,8,17,18 However, there have been few studies reporting QTc interval change following LMA insertion. A remifentanil bolus has peak effect of 1-1.5 min and action duration of 3-4 min.19 We hypothesized that remifentanil by bolus injection may be useful for controlling transient cardiovascular stimulation and QTc change.
Prevention of prolonged QTc with remifentanil administration could be related to various mechanisms of the drug's action.
Tracheal intubation itself prolongs the QTc interval by activating the sympathetic nervous system. A supraglottic tissue irritation following direct laryngoscopy is reason for hemodynamic change after tracheal intubation. Therefore, we anticipated that avoiding stimulation of laryngeal tissue with the LMA may cause less of an increase in the QTc intervals. However, in our study, 75% of patients in the placebo group, and 20% of patients in the remifentanil group, showed prolongation of QTc to over 450 ms during the study period.
Inadequate pharyngeal analgesia may have a role in increasing sympathoadrenal response and QTc changes in the absence of laryngeal muscle stimulation. Sevoflurane and remifentanil may show synergy in their antinociceptive action.20
The predominant and usual effect of opioids on the HR is induction of bradycardia through stimulation of the central vagal nucleus. Vagal-cardiac activation with remifentanil may attenuate the effects of sympathetic stimulation during LMA insertion.
Diverse types of potassium channel exist in myocardial cell membrane. The rate of repolarization of action potential are mostly controlled slowly activating (iKs) and rapidly activating (iKr) delayed rectifier channels during phase 2 and 3 of the electrical cardiac cycle. Inhalation anesthetic agents prolong the QTc through blocking the iKr channel.
Effects of opioids on potassium channels was not clearly known. Katchman, et al.4 reported fentanyl could block cardiac human ether-go-go related gene currents at a very high dose. This was consistent with the finding that during induction of anesthesia in patients undergoing coronary artery bypass graft surgery, the QT interval increased significantly after injection of fentanyl.21 Though chemically related to the fentanyl family of short-acting phenylpiperidine derivatives, remifentanil is structurally unique because of its ester linkage. We were not aware of previous studies describing the effects of remifentanil on K+ currents.
This study has some limitations. Considering that muscle rigidity or inadequate relaxation may affect measurements of QTc, we used small dose of vecuronium. However, previous works have suggested that vecuronium has no effect on QTc and cardiac conduction.22
QT interval is influenced predominantly by heart rate. Thus, a rate-corrected QT (QTc) interval should be calculated. Bazett's formula is the most popular in clinical practices. This formula may exaggerate drug-induced QT prolongation.
Generally, QT is considered to be prolonged when the QTc interval is greater than 440 ms in men and 460 ms in women, although arrhythmias are most often associated with values of 500 ms or more.23
The other limitations of this study are that it was performed only on women and on patients without a known cardiac disorder. Women have longer QT intervals and are more prone to drug-induced QT prolongation. The changes we found may less extensive in men. Also, it would be better to do later studies on patients with repolarization disorders.
In conclusion, remifentanil reduced the prolongation of corrected QT interval induced by LMA insertion in patients undergoing minor gynecological study during inhalation induction with sevoflurane. A low bolus dose of remifentanil and LMA may be acceptable for patients with proarrythmogenesis.




 XML Download
XML Download