

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Over the past 30 years, the introduction of preoperative chemoradiotherapy (CRT), advances in surgical techniques, and new imaging modalities for selecting treatment and surgical planning have resulted in dramatic improvements in local recurrence rates and quality of life in patients with rectal cancer. In this context, baseline magnetic resonance imaging (MRI) in patients with locally advanced rectal cancer (LARC) has an undeniable role in the determination of neoadjuvant CRT through risk stratification by the evaluation of circumferential resection margin (CRM), T3 sub-classifications, and assessment of extramural vessel invasion, nodal status, and sphincter invasion (1). Therefore, there is a uniform consensus on the value of baseline MRI in the preoperative evaluation for patients with rectal cancer (2). After CRT, most LARCs demonstrate variable degrees of tumor response, including pathologic complete remission (pCR) in 4–31% of patients (3). Patients with complete remission (CR) by CRT can achieve excellent local tumor control and a better quality of life with organ-preserving treatments such as local excision or even watchand-wait management (4). Therefore, an evaluation of tumor responses may become a key factor in determining the treatment strategies for individual patient after CRT.
Post-CRT MRI is also considered to be the first choice for evaluating treatment response after CRT. However, whether post-CRT MRI evaluation for tumor response can inform treatment strategies remains controversial. Surgeons are often reluctant to deviate from initial plans because of concerns about residual viable tumor cells in the rectal wall or the mesorectal nodes, even in patients with clinical complete response (cCR) after preoperative CRT (5). Furthermore, the diagnostic outcomes and clinical impacts of post-CRT MRI have not been satisfactory for deciding the more radical surgical dissection or the organ-preserving strategy because of insufficient reliability for differentiating residual tumors from CRT-related changes such as edema, necrosis, and particularly fibrotic change after CRT. Therefore, radiologists should be aware that their interpretation might result in a faulty decision for organ-preserving treatment or conversely unnecessary radical surgery which compromises patients' quality of life.
In this review, we will introduce recent advances in the treatment of LARC and describe the role of post-CRT MRI in the clinical restaging of rectal cancer after CRT concerning improving local control and patient quality of life. Finally, we will discuss the issues faced by radiologists in determining tumor response after CRT.
Treatment Options after Chemoradiotherpy for Locally Advanced Rectal Cancers
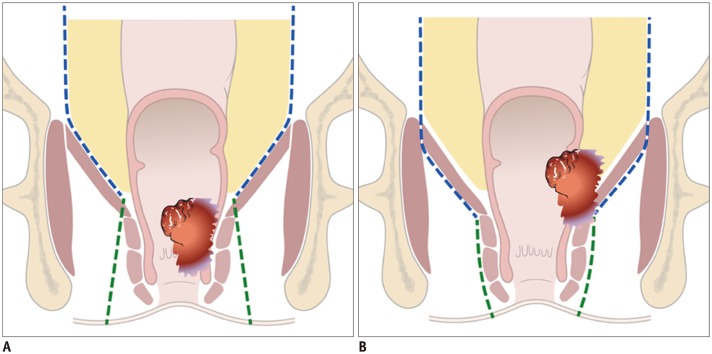
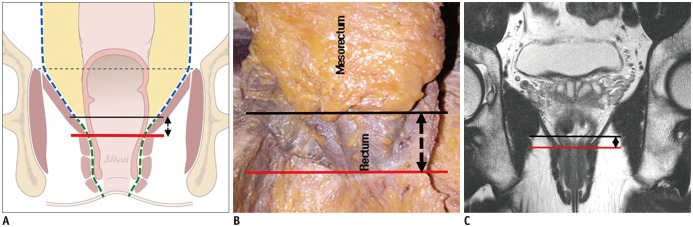
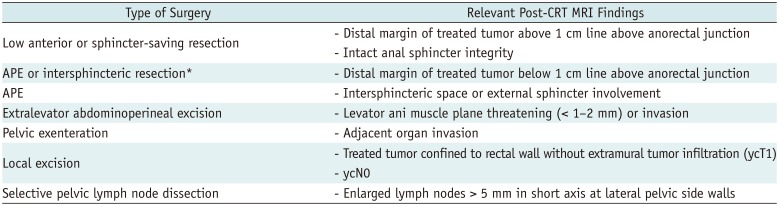
Total mesorectal excision (TME) is the standard treatment for the majority of patients who underwent CRT for rectal cancer. It emphasizes en-bloc resection of the mesorectum which refers to the fatty tissue envelope of the rectum, containing blood and lymphatic vessels (6). TME can be performed as a component of low anterior resection (LAR) or abdominoperineal excision (APE) procedures. The decision to perform either LAR or APE is based on the tumor location in relation to the anal sphincter complex. LAR is any sphincter-preserving resection with anastomosis beneath the anterior peritoneal reflection. LAR can be further divided into LAR and ultra-LAR including intersphincteric resection based on the level of dissection and anastomosis (above or below the mesorectal end, respectively) (7). While LAR is performed for tumors that are distant from the anal sphincter, APE is defined as an enbloc removal of a tumor with the anal sphincter and anus, accompanying a permanent colostomy (Table 1, Fig. 1) and is usually performed for tumors that are near to or involve the anal sphincter (intersphincteric plane or external sphincter involvement). Therefore, the distance between the distal end of the tumor and anorectal junction should be provided in the post-CRT MRI evaluation. In the era of neoadjuvant CRT, distal surgical margin even ≤ 1 cm appear sufficient (8). Anatomically, there is no mesorectal fat up to approximately 1 cm above the anorectal junction (upper end of intersphincteric plane) (Fig. 2) (9). Treatment failure is common at this level because the tumor penetrating the muscle proper directly abuts levator ani muscle without intervening mesorectal fat (1011). Therefore, the information about whether the distal level of a tumor is located above or below the level of the mesorectal end (approximately upper end of intersphincteric plane) 1 cm above the anorectal junction is important for determining the salvage of anal sphincter.
APE can be classified into traditional APE or extralevator abdominoperineal excision (ELAPE) (Fig. 1). Unlike traditional APE, because ELAPE includes the en-bloc removal of the levator muscles, ELAPE is considered to be a more radical approach and thus increases CRM clearance, particularly in patients whose levator plane is still threatened on post-CRT MRI (Figs. 1, 3) (12). For T4b tumors which invade other organs such as urinary bladder, prostate, uterus, or sacrum, pelvic exenteration can be performed (13).
Recently, organ-preserving strategies have also been deployed to avoid rectal excision in patients in whom complete tumor shrinkage without residual tumor tissue has been identified after neoadjuvant CRT. These strategies are divided into local excision and watch-and-wait strategy. Patients showing clinical downstaging to cT0-1N0 after CRT may be candidates for local excision. Local excision procedures include transanal excision (TAE), transanal endoscopic microsurgery (TEM), and transanal minimally invasive surgery (TAMIS) (14). TAE is indicated for tumors that lie below the level of peritoneal reflection. TEM or TAMIS are performed for tumors that lie above the peritoneal reflection. With these local excision techniques, resection of full tissue layers including mucosa, submucosa, and muscle proper can be performed. However, the complete dissection of the lymph nodes is impossible. Therefore, careful evaluation to guarantee the absence of extramural tumor infiltration and residual metastatic lymph node on post-CRT MRI is crucial for oncologic safety.
Surgical planning should be conducted to accurately assess the extent of the local tumor and the relationship between residual tumors and the anal sphincter on post-CRT MRI. However, distinguishing residual viable tumors from fibrotic changes following CRT is often challenging on post-CRT MRI. Although fibrotic changes appear as decreased signal intensity (SI) on T2-weighted images, even the dense dark fibrotic tissue on MRI could have microscopic viable residual cancer cells. The possibility of a viable residual tumor in the dark fibrotic tissue is known to be approximately 50% (15). Determining tumor relationships with the surrounding structures (e.g., the anal sphincter) on the basis of T2 SI changes only according to the hypothesis that only the intermediate T2 SI portion within the treated mass is viable cancer and the dark SI portion is exclusively fibrotic change, may jeopardize oncologic safety (Fig. 3). Furthermore, the relationship between tumors and surrounding organs or sphincters on post-CRT MRI should be determined on the basis of the whole treated tumor including any fibrotic tissues, except for fibrotic spiculations. The possibility of residual cancer cells within the fibrotic spiculation on post-CRT MRI is known to be extremely rare (16).
Timing of MRI for Evaluation of Treatment Response after Chemoradiotherapy
The optimal timing of post-CRT MRI for the evaluation of tumor response depends on the timing of surgery after CRT. However, surgical timing with respect to CRT varies due to a lack of consensus on the optimal interval. Because tumoricidal effects of CRT increase over time (Fig. 4), it is possible that more cases achieving pCR would be identified with a longer waiting time after CRT (17). However, because surgeons are reluctant to delay operation beyond eight weeks due to concerns about radiation-induced pelvic fibrosis and related surgical complications, surgery is generally performed at approximately 6–8 weeks after the completion of CRT (18), although delaying surgery more than eight weeks after completion of CRT may be more beneficial (19). Therefore, post-CRT MRI should be performed 6–8 weeks after the termination of CRT, and immediately before surgery.
Reported Items on Post-Chemoradiotherapy MRI
After neoadjuvant treatment, reports of rectal MRI should include the following items: local tumor status, mesorectal fascia (MRF) involvement, lymph node involvement, and extramural venous invasion (EMVI) status (20).
Local Tumor Status
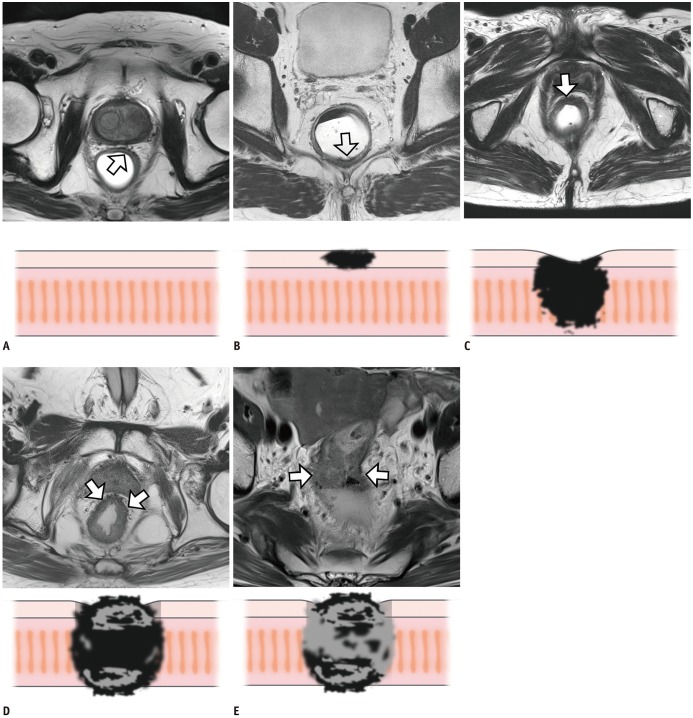
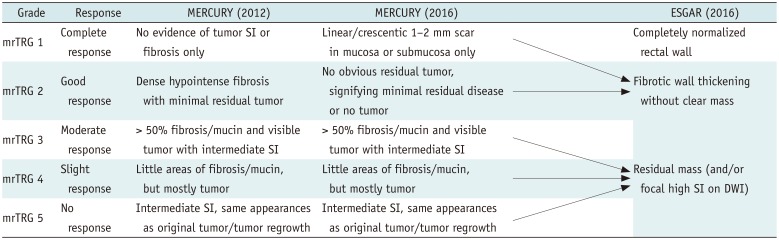
Accurate preoperative assessment of local tumor status following CRT is essential for deciding an appropriate treatment strategy. Tumor response after CRT can be evaluated by assessing MRI-based tumor regression grade (mrTRG) using an established scoring system and post-treatment T staging (ymrT) (21). Scoring systems established by the Magnetic Resonance Imaging and Rectal Cancer European Equivalence Study (MERCURY) study group and the European Society of Gastrointestinal and Abdominal Radiology (ESGAR) are mostly similar but differ most notably in their definitions of good responders (Table 2, Fig. 5) (202122). mrTRG scores developed by the MERCURY study group were derived from pathologic TRG (pTRG). mrTRG was defined according to whether fibrous or tumor SI predominates within the entire tumor (23). In other words, mrTRG is determined by the proportion of presumed residual tumor and fibrotic change on T2-weighted images. On post-CRT T2-weighted imaging, the fibrotic portion shows dark SI similar to that of the muscularis propria, whereas the portion of the residual tumor shows intermediate SI similar to that of baseline tumor (24). mrTRG scoring system and the definition of TRG 1–2 have been changed between 2012 and 2016 (20). Grade 1 now indicates a complete radiologic response with a linear/crescentic 1–2 mm scar in the mucosa or submucosa on MRI (Fig. 5B). Grade 2 is indicated by a good response and MRI findings include dense fibrosis without obvious residual tumor, suggesting minimal residual disease or no tumor (Fig. 5C). Grade 3 is indicated by a moderate response, with more than 50% of areas with fibrosis/mucin and visible intermediate tumor signal on MRI (Fig. 5D). Grade 4 suggests a slight response to treatment, with MRI findings of few areas with fibrosis/mucin and mostly tumor-derived MRI signal (Fig. 5E). Grade 5 indicates no response to therapy, showing a similar tumor to the baseline or significant tumor regrowth. These mrTRG scores have significant implications for clinical care and outcomes. According to a previous study, disease-free survival and overall survival differed significantly between mrTRG 1–3 (good response) and mrTRG 4–5 (poor response) (25). Recently, the definition of good responder has been evolved in mrTRG scoring system due to an introduction of organ-preserving approach. It requires a higher positive predictive value (PPV) for pCR or near-pCR. Therefore, recent reports suggest only mrTRG 1 and 2 as good responders or candidates for organ-preserving treatments (2627).
Different from a 5-point mrTRG scoring system, ESGAR consensus meetings have suggested a three-stage classification: completely normalized wall, fibrotic wall thickening only, and residual mass. They proposed that an identification of a normalized two-layered wall after CRT is suggestive of CR on T2-weighted imaging (Fig. 5A) and fibrotic residue without an isointense mass may indicate CR or near-CR (Fig. 5B, C). However, the item related to a normalization of the rectal wall is not included in mrTRG scoring system proposed by MERCURY group. Therefore, the actual threshold for defining radiologic CR is somewhat different between the two scoring systems. Considering that complete normalization of the rectal wall after CRT is extremely rare in clinical practice, ESGAR group seems to take a stricter position in defining radiologic CR.
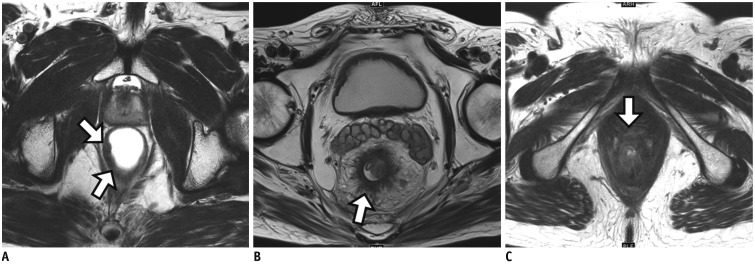
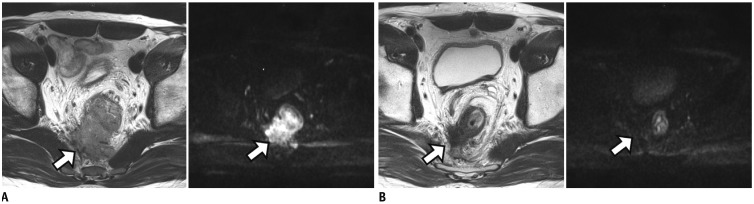
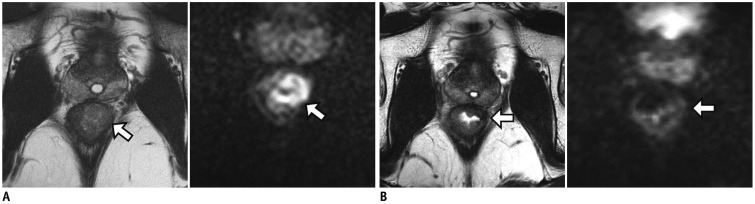
Local tumor status can also be assessed by post-treatment T staging (ymrT). On post-CRT MRI, yT stage can be defined as yT1–2, yT3, and yT4. yT3 can be further divided into yT3a or 3b with ≤5 mm extramural tumor depth and yT3c or 3d with > 5 mm extramural tumor depth. yT4 is designated when the tumor invades into the visceral peritoneum or adjacent organs/structures (Fig. 6). Reported overall sensitivity of T2-weighted imaging in a meta-analysis is unsatisfactory (approximately 50%) (28). Overstaging is the main source of staging error because CRT-induced fibrotic change at the interface between the tumor and the mesorectal fat can usually be mis-interpreted as viable tumor. The meta-analysis also revealed that restaging with diffusion-weighted imaging (DWI) demonstrated an improved mean sensitivity without a decrease of specificity. Therefore, DWI may be the solution for overcoming such overstaging issue (Fig. 7).
For tumors located in the far distal rectum, it is important to evaluate the relationship between the tumor and anal sphincter complex, particularly when deciding whether sphincter-saving surgery is possible or not (20). In such cases, a precise description regarding the relevant anatomical relationships may provide more valuable information than ymrT stage alone. Following findings are usually recommended to be described for lower tumors near the anal sphincter complex: 1) distal margin of the tumor whether it is located at above or below from the line 1 cm above the anorectal junction, 2) sphincter involvement by the tumor whether the tumor invades only to the internal sphincter muscle or extends to the intersphincteric fat plane/external sphincter muscle, and 3) involvement of levator ani muscle. The line 1 cm above the anorectal junction (black line in Fig. 3A) is approximately identical to an upper margin of the intersphincteric plane where is vulnerable to levator threatening (910). Therefore, it is important to report the relationship between this line and distal margin of the tumor. For lower rectal cancers that threaten the levator ani muscle or involve the intersphincteric plane/external sphincter muscle, sphincter-saving surgery is not feasible. However, if the tumor shows a favorable response such as mrTRG 1 or 2 after CRT and no extramural tumor spread such as nodal metastasis is present on post-CRT MRI, organ-preserving surgery such as intersphincteric resection or TAE may be considered (26).
Circumferential Resection Margin Involvement
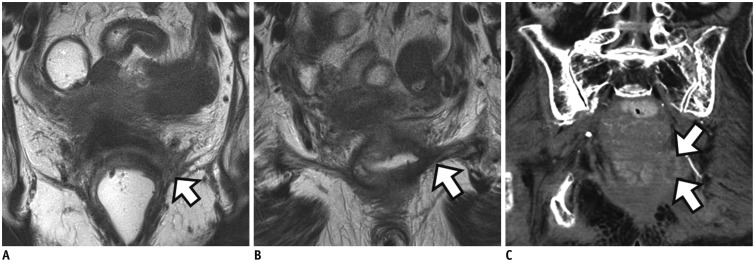
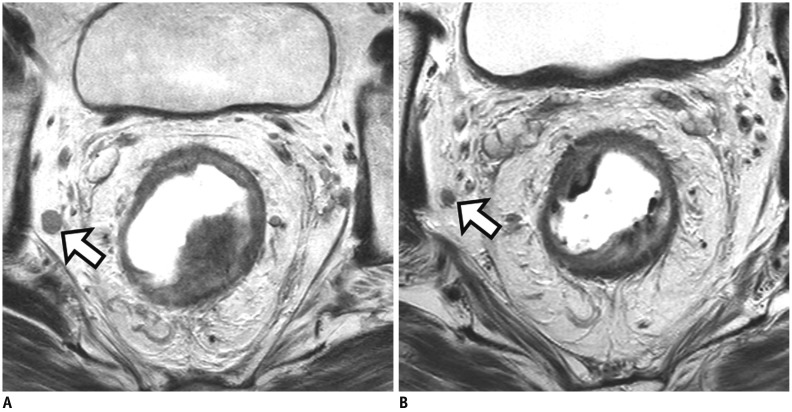
Pathologic circumferential resection margin (pCRM) is one of the key components for the determination of local tumor recurrence in patients who undergo TME with or without preoperative CRT (2529). Prospective trials have reported a local recurrence rate of 25–26% after CRT in patients with pCRM involvement (2530). The definition of positive pCRM in most studies is the presence of tumor cells within 1 mm from resection margin (31). On baseline MRI, when the shortest distance between the tumor and MRF is ≤ 1–2 mm, potential CRM is considered to be threatened or involved. However, an interpretation of MRF involvement after CRT is problematic because hypointense fibrotic change frequently remains at the initial tumor area (Fig. 7). Such limitations result in a low PPV (44–57%) and high negative predictive value (NPV) (91–100%) of post-CRT MRI for positive pCRM (163233) with an area under the receiver operating characteristic curve (AUC) of 0.73–0.89 (163435). Although high NPV of post-CRT MRI may guarantee the oncologic safety after TME, low PPV prevents the decision for performing more aggressive or additional treatments. To overcome this issue, a few groups have suggested specific morphologic patterns on MRI for determining MRF involvement after CRT in addition to applying the distance from MRF (1–2 mm) (1634). Specifically, if MRF infiltration/penetration by fibrotic or tumor tissue is present along with fibrotic thickening of MRF itself, a higher risk of pCRM involvement after CRT is suggested compared to MRF threatening only by spiculated fibrotic change or treated tumor without thickening of MRF itself (Fig. 8). Some investigators have also reported the potential value of DWI to predict tumor clearance at the MRF after CRT (36). In this study, the PPV for MRF involvement was significantly higher with combined T2-weighted imaging and DWI (82–91%) than with T2-weighted imaging alone (30–45%) (p ≤ 0.025) (36). If high-risk patients with positive pCRM even after CRT can be accurately selected, an evidence for introducing additional treatment options such as extramesorectal excision or multivisceral resection, boost radiotherapy at the site of MRF invasion, or upfront chemotherapy may be provided in these highly selected patients.
Lymph Node Involvement
Considering local excision may be a suitable option for patients with good tumor response to CRT without residual positive lymph nodes, radiologic nodal restaging after CRT is crucial for the assessment of these patients. MRI criteria used to determine lymph node involvement may differ between before and after CRT. Before CRT, morphologic findings such as border irregularities and heterogeneous SIs are better predictors than the size of lymph nodes (37). On the other hand, after CRT, these morphologic criteria were found to be unreliable predictors for determining malignant nodes (3839). Moreover, decreased nodal size (e.g., < 3 mm) after CRT can limit the evaluation of these morphological features; thus the size criteria (e.g., a short axis > 5 mm) may be more reliable.
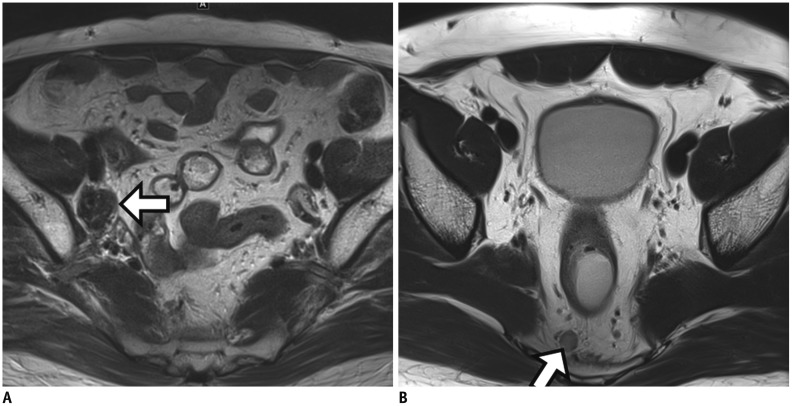
Previous studies have indicated that size measurement after CRT shows better performance with an AUC of 0.85–0.90 than primary staging (AUC = 0.75) (4041). A possible explanation for such better performance of size criteria after CRT is that the size and number of lymph nodes harvested after CRT are reduced (4243), decreasing the potential for interpretation errors in the remaining small lymph nodes. On histology, many lymph nodes after CRT reveal fibrous capsular thickening and sclerosis within the medulla (44). In addition, radiologists should be aware that a decrease in size of nodes after CRT cannot always guarantee malignant nodes because benign as well as malignant nodes can show decrease in size after CRT (4344) (Fig. 9).
In lateral pelvic lymph nodes, the same size criteria (a short axis > 5 mm) can be used to reliably identify malignant nodes after CRT (4546) (Fig. 10). Persistently enlarged lateral pelvic nodes > 5 mm on post-CRT MRI are significantly associated with residual nodal metastasis and the size of lateral pelvic node on post-CRT MRI is an independent predictor for lymph node metastasis (46). Therefore, the decision of selective lateral pelvic node dissection should be made on the basis of nodal response to CRT (e.g., via size of lateral pelvic node on post-CRT MRI) (Table 1) (4546). For patients with responsive lateral pelvic nodes (short axis < 5 mm) after CRT, lateral pelvic node dissection may not be necessary although there has been still a debate on this issue.
Extramural Venous Invasion
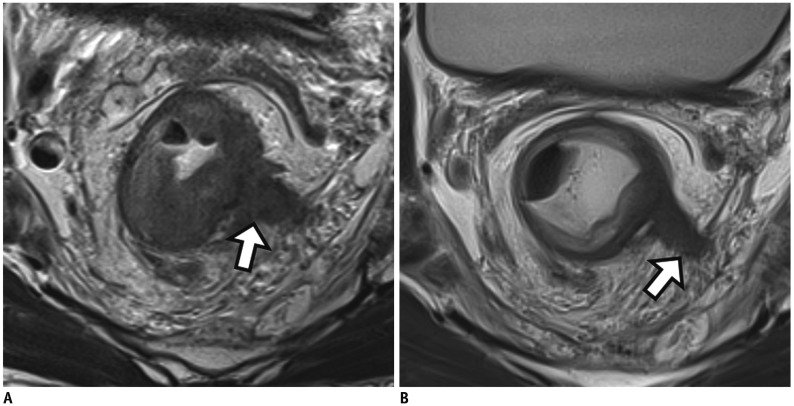
EMVI is pathologically defined when tumor cells invading the veins beyond the outer walls of the muscularis propria are present (47). After CRT, EMVI can be assessed either by histopathology (ypEMVI) or by MRI (ymrEMVI). ymrEMVI is defined as positive when minimal or less than 25% fibrotic change is detected on treated tumor component within the extramural venous structure (Fig. 11) (4849).
Lee et al. (48) reported that the diagnostic performance of MRI for determining EMVI after CRT was comparable to that on pre-CRT MRI (AUC, 0.830 versus 0.778, p = 0.076) when using the same scoring system for mrEMVI. According to another study by Chand et al. (47), positive EMVI after CRT was more frequently detected on MRI than on histopathology (53% versus 19%) and both ymrEMVI (hazard ratio 1.97) and ypEMVI (hazard ratio 2.39) were significant predictors for decreased survival. Considering the advantages of MRI such as multiplanar imaging capability and visualization of the entire rectum (50), radiation-induced fibrosis and destruction of venous endothelium after CRT may be responsible for a higher false-negative rate of EMVI on histopathology (51). As persistent ymrEMVI after CRT may increase the risks of metastatic disease, it is an independent negative prognostic marker for disease-free survival and implicit potential benefits of adjuvant chemotherapy (47).
Determining Complete Response on Post-Chemoradiotherapy MRI
Most LARCs show variable tumor response, including pCR in up to 33% of patients (2152). Patients who achieved CR after CRT may potentially achieve excellent local tumor control and superior quality of life with organ-preservation strategies such as local excision or even a watch-and-wait approach (535455). If patients who have achieved pCR after CRT can be accurately identified before surgery, organ-preservation treatment strategies might be considered as an option in those selective patients. By avoiding radical surgery in these patients, the need for a permanent stoma may be avoided (535455). However, if an inaccurate assessment for pCR status was made, the patients may lose the chance of standard radical TME surgery. Resultantly, oncologic safety of those patients may be severely jeopardized. Consequently, an increasing interest in organ-saving treatments can be met only if a reliable method to identify pCR is developed (5657). In reality, however, an accurate identification and prediction of pCR is still challenging, as a reliable and non-invasive method is not yet fully available (58). Limited ability of post-CRT MRI to predict pCR also leaves a gap in the clinical process of determining a reasonable treatment strategy. The ideal balance between the sensitivity and specificity of MRI for the prediction of pCR is an ongoing issue of debate. Considering that a false-positive prediction of pCR can lead to an inappropriate use of organ-preserving treatments, potentially resulting in devastating outcomes, a conservative decision for cCR should be made to maximize the PPV of post-CRT MRI for the prediction of pCR when the results are equivocal.
Recently, a large-scale registry study investigated the clinical outcomes of patients with cCR, reporting a 2-year cumulative local regrowth rate of 25.2% (59). Among cCR patients with local regrowth, 97% of local regrowth was detected at the bowel wall while distant metastasis occurred in 8% of cCR patients. Based on this result, unsalvageable disease is rare even in cCR patients with later tumor regrowth (59). Therefore, this data support that a watch-and-wait strategy or deferred curative surgery can be performed as reasonable treatment options for cCR patients if an adequate clinical surveillance is guaranteed.
T2-Weighted Imaging
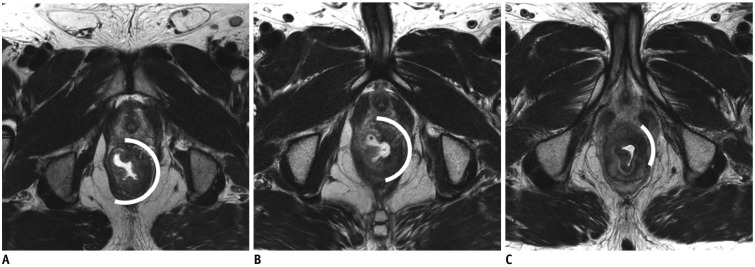
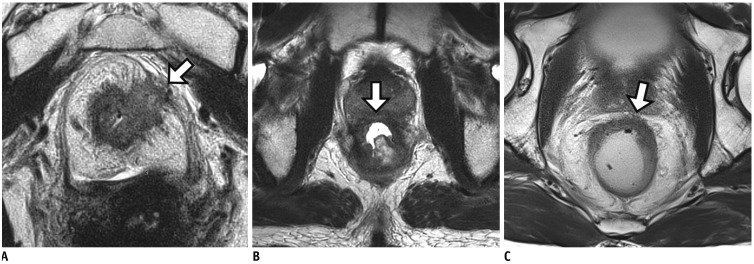
Pathologic CR can be theoretically achieved in patients with mrTRG 1 and 2 (MERCURY classification) or complete normalization and fibrotic tissue (ESGAR classification) (Table 3). Clinical CR on T2-weighted MRI can be diagnosed when intermediate tumor signal disappears with or without fibrotic residues (Fig. 12). However, characterizing residual tumor with MRI is challenging because a distinction between fibrosis with and without residual tumors is difficult. Although a signal drop of the tumor on T2-weighted image is widely accepted as a hallmark of CRT-induced fibrosis, fibrosis frequently intermixes with viable tumor tissues and distinguishing these two components is often a difficult task (23). Furthermore, hyperintense mucin on T2-weighted image makes the prediction of residual tumor viability more challenging (60). Intermingled tumor cells with fibrosis and the presence of mucin may be responsible for low level of agreement between mrTRG and pTRG, rendering mrTRG as an inappropriate surrogate for the prediction of pTRG (61). Indeed, the reported sensitivity and specificity for diagnosing pCR are 74.4% and 62.8%, respectively even in patients showing good response on post-CRT MRI (mrTRG 1 or 2) (61).
MR Tumor Volumetry
There have been several reports regarding the usefulness of MR volumetry for the prediction of tumor response after CRT (6263). In those studies, investigators used both quantitative SI and volume of the tumor in order to selectively measure the volume of viable tumor tissues on post-CRT MRI. They performed SI-selective volumetry with an exclusion of non-viable tissue components (fibrosis with low SI and mucin with high SI) using an intensity threshold. For example, pelvic muscle was used as an internal reference to define a threshold of fibrotic tissue. This approach seemed to improve the diagnostic performance of MRI for pCR assessment, compared with simple qualitative assessment or whole tumor volumetry (6263).
Diffusion-Weighted Imaging
Recently, DWI has been increasingly used and is routinely included in rectal MRI protocols (20). A few studies have reported encouraging results on DWI, describing its usefulness in aiding conventional MRI to improve the diagnostic accuracy for predicting pCR after CRT (Figs. 7, 12) (6465).
Even though DWI offers several benefits in various applications, it also has multiple possible shortcomings. For example, manual drawing of ROIs onto the tumor for quantitative or qualitative assessment may result in interobserver variation. Furthermore, image distortion due to artifacts is common on DWI, particularly around air-tissue interfaces. During the restaging of tumor, radiologists tend to overestimate the presence of a tumor on T2-weighted image alone. According to previous studies, such overestimation can be reduced when DWI was added on T2-weighted image (646566). In real clinical practice, however, such corrective effect of DWI may not be encountered because most conservative radiologists would not change their decision to cCR even in patients with no diffusion restriction on DWI if when residual tumor signal is present on T2-weighted imaging.
According to a previous study, DWI volumetry without T2-weighted imaging showed highest AUC (> 0.90) for the assessment of pCR. This observation might be due to the fact that the bias related to T2-weighted imaging can be eliminated in this study (66). Another subsequent biinstitutional independent validation study proved that the previously established cutoff value for DWI volumetry could be used to assess pCR after CRT accurately (15). Therefore, DWI volumetry may have some potential to overcome intrinsic limitations of qualitative DWI-related artifact or radiologists' conservative tendency.
Combined Use of MRI and Colonoscopy
In the past, endoscopy and digital rectal exams served as the main tools for the assessment of treatment response (1567). Continuous decrease in tumor size and the disappearance of tumor tissues along with mucosal healing, were regarded as clinical signs of CR on endoscopy (57). However, a major limitation of these techniques is that transmural or extraluminal tumor extent as well as mesorectum cannot be examined (57). Because residual tumors can present in any layer of the rectal wall regardless of tumor stage (576869), MRI can reveal such residual tumors beneath the mucosa, which can be inaccessible via colonoscopy.
Endoscopy and MRI may play a complementary role in rectal cancer restaging. Maas et al. (57) reported that the combined use of MRI and endoscopy resulted in a high PPV (98%). Although an improved PPV maximizes oncologic safety, it also decreases the opportunity of organ-preserving treatment in pCR patients with equivocal findings (57). However, we believe that such a conservative approach may be reasonable considering the limitation of imaging tools for predicting pCR after CRT and oncologic safety.
Selection of Candidates for Local Excision after Chemoradiotherapy
Considering the limitations of MRI or endoscopy in predicting pCR, local excision may be a more go-ahead approach. Indeed, there have been conflicting arguments for the indications for local excision. Some reports have demonstrated acceptable oncologic outcomes after local excision for ypT2 lesions (425470) while lymph node metastasis was reported in up to 20% of ypT2 lesions (387172).
The most important issue in selecting patients for local excision is the guarantee of pN0 before an organ-preserving treatment because lymph node removal is not performed and any residual viable tumor deposit may be left behind after local excision (42). Indeed, the risk for tumor recurrence after local excision has been described to parallel the risk of lymph node metastasis (2.0–9.1% for ypT0, 15.0–17.1% for ypT1, and 17.0–20.8% for ypT2) (387172). Therefore, an acceptable NPV for the presence of metastatic nodes is crucial for planning organ-preserving treatment. Even though the use of size criteria on post-CRT MRI shows a relatively high NPV (78–96%) (3870), such imperfect NPV does not entirely guarantee the oncologic safety after local excision. Therefore, the risk of local tumor recurrence due to residual metastatic lymph nodes should be compensated by strict MRI follow-up so as to facilitate early detection during the time window in which curative radical resection can still be performed (42).
SUMMARY
Along with significant improvement in terms of treatment options and imaging tools, there is an increasing demand for reliable risk stratification after CRT for personalized tailored treatments in patients with LARC. Radiologists should be familiar with new surgical approaches. With the knowledge of oncologic concepts specific to rectal cancer management, radiologists should provide critical information during post-CRT MRI interpretation such as mrTRG, ycTN staging, relationship with anal sphincter complex, CRM status, and ymrEMVI. Post-CRT MRI may play a prominent role in the decision-making process for rectal cancer management. However, because current MRI techniques have several limitations for assessing treatment response after CRT, tumor response evaluation on post-CRT MRI should be reliably or safely determined with an aid of DWI, MRI volumetry, and complementary endoscopy, balancing between oncologic safety and quality of life for patients.

 XML Download
XML Download