

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The accidental ingestion of a corrosive substance is a common cause of esophageal strictures in children (1). Corrosive substances, whether acid or alkali, can both cause significant esophageal strictures, though reactions differ (i.e., acids cause coagulation necrosis of the mucosa, whereas alkalis, like lye, produce liquefaction necrosis that may penetrate deeper layers including muscular layers) (2). Because glacial acetic acid is still used domestically by some as a food seasoning in East Asia, the occurrence of accidental acid ingestion and of subsequent corrosive esophageal stricture development is more frequent in East Asia than in other parts of the world (3, 4).
Treatment for esophageal strictures in children has evolved from surgical revision, to esophageal bougienage, and to the currently used esophageal balloon dilatation (EBD) (5). Since London et al. (6) reported the successful treatment of esophageal strictures with a Gruentzig-type balloon catheter in 1981, EBD has been accepted as a safe and effective treatment for benign esophageal strictures (2, 7-9). In infants and children, this technique has been primarily used to treat anastomotic strictures resulting from surgery for esophageal atresia (7-10). However, although EBD is considered as a safe and effective treatment for esophageal stricture, to the best of our knowledge, its safety and effectiveness for the treatment of corrosive esophageal stricture in children has rarely been reported (11-14). The purpose of our study was to retrospectively evaluate the effectiveness of EBD for the treatment of a corrosive esophageal stricture in children.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the medical records and radiologic findings of 14 children who underwent EBD for corrosive esophageal stricture in our institution from August 1991 to January 2007. The authors' Institutional Review Board approved this retrospective review of clinical data and radiologic findings and waived the requirement for informed consent.
The patients included eight boys and six girls with a median age 24 months (range: 17-85 months) at the time of the initial EBD. The caustic agents that caused an esophageal stricture were acid (glacial acetic acid) in nine patients, and alkali (lye) in five patients. Children were considered for EBD when one or more of the following symptoms were present: excessive drooling unrelated to oral intake, regurgitation of food particles immediately after oral intake, and discomfort associated with oral intake (15). EBD was begun at least one month after a corrosive injury because complications may occur during the acute or early phase (16). Periods between caustic agent ingestion and initial EBD ranged from 1 to 57 months (median; 2 months).
Balloon Dilatation Procedures
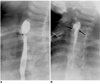
All patients underwent a barium esophagography at one day before performing an EBD to evaluate the stricture location and extent. Based on narrowed segment lengths, lesions were classified into three types: lesions < 1 cm in length were defined as focal strictures (Fig. 1), those between 1 cm and 3 cm were defined as segmental strictures (Fig. 2), and those > 3 cm were defined as long strictures (Fig. 3).
The EBD procedures were performed by an experienced pediatric radiologist. In all cases, in order to perform an EBD, written informed consent was obtained from the parents. Before dilation, patients fasted for at least six hours to reduce stomach contents and were placed on a fluoroscopic table in the supine position. Patients were strongly sedated by a nurse with intravenous midazolam (Midazolam injection; Bukwang, Ansan, Korea). Under fluoroscopic guidance, a guidewire with a soft tip (Radiofocus, Terumo, Tokyo, Japan) was introduced through the nostril and was positioned in the stomach. A Gruentzig-type balloon catheter (Schneider, Zurich, Switzerland; Medi-tech/Boston Scientific, Watertown, MA) was then passed over the guidewire, placed across the stricture, and slowly inflated with diluted water-soluble contrast material (Telebrix; Guerbet, France). The correct positioning of the balloon at the level of esophageal stricture was confirmed when the 'waist' was in the center of the balloon. Manual inflation which was held for 30 seconds was performed until the waist of the balloon contour disappeared (Fig. 2) or showed no further change in its shape and diameter despite a positive inflation pressure (Fig. 3). Inflations were repeated three times per session. The sizes of the initial balloon catheter were chosen based on the estimated esophageal caliber of the stricture segment and the esophagus distal to the stricture, as determined by an esophagography before an EBD. Balloon catheter sizes were increased by 2 mm for subsequent EBD sessions, if a dilatation had been easily achieved and the balloon catheter upon removal showed little evidence of blood or blood clot. Once it was determined that no further dilatations were necessary, a pull-back esophagography was performed through the retracted balloon catheter to evaluate the possibility of procedural complications such as an esophageal perforation. In the absence of evidence of free leakage, a water-soluble contrast esophagogram was obtained at least two hours after patients had recovered from sedation to evaluate stricture improvement, delayed leakage, or the further extension of a small leakage. Patients were allowed a soft food diet and were encouraged to resume a regular diet the day following the procedure. Repeat dilatations were scheduled if there was a recurrence of the symptoms described above.
Follow-Up and Outcomes
The patients' medical records were reviewed and the following clinical and radiological data were obtained: improvement in the patient's age-appropriate food intake and dysphagia after each session of EBD, number of EBDs for each patient, total time from the first EBD to the last EBD, and complications of EBD. We defined temporary success for an EBD as dysphagia relief (i.e. the acceptable swallowing of liquid or solid foods) for at least one month after the EBD session and long-term success for an EBD as dysphagia relief for at least 12 months after the last EBD (10, 13).
Statistical Analysis
The overall association between the ingested materials (i.e., acid versus alkali) and type or location of esophageal stricture was assessed by Fisher's exact test. We evaluated the association between temporal success of an EBD and the size of the balloon, number of EBD, age at the first EBD, as well as the interval between the time of caustic agent ingestion and the first EBD by Mann-Whitney test. We also evaluated the overall association between the temporary success of an EBD and the caustic agent with the type or location of the stricture by Fisher's exact test. For all tests, p < 0.05 was considered to indicate a statistically significant difference. Statistical analyses were performed with SPSS 7.5 for Windows software (SPSS, Chicago, IL).
RESULTS
The clinical and radiological data of the 14 patients are summarized in the Table 1.
Type of Esophageal Stricture
Four patients had a focal stricture (Fig. 1); all of which had ingested glacial acetic acid. Their strictures were located in the upper third portion of the esophagus. In the case of segmental (n = 2) or long (n = 8) strictures involved in the mid-portion of the esophagus. These type of strictures were caused by lye (n = 5) or glacial acetic acid (n = 5) (Figs. 2, 3). All patients having ingested lye had long strictures. None of the 14 study subjects showed gastric outlet obstruction. There was a statistically significant association between caustic agents (acid versus alkali) and the type of esophageal stricture (focal or segmental versus long strictures) (p = 0.031), or the location of the strictures (upper versus mid-esophagus) (p = 0.031).
EBD for Corrosive Esophageal Strictures
A total of 52 EBD sessions were performed in 14 patients, with 1 to 8 sessions per patient (median: 4 sessions per patient). The balloon was fully dilated in 51 out of 52 sessions (98%). An initial EBD was performed using a balloon of at least 8-mm in diameter in 10 patients, whereas in four patients with severe focal (n = 2) or long (n = 2) strictures, we used a balloon less than 8-mm in diameter. The maximum balloon diameter of the last session ranged from 10 to 15 mm in 10 patients and was 8 mm in four patients.
Contrast leakage, suggesting a submucosal tear, was observed by esophagography after two (4%) out of the total 52 sessions. Associated strictures were of the focal type caused by acid ingestion (n = 1) or of the diffuse type caused by lye ingestion (n = 1). In these two patients, a follow-up esophagography obtained after two weeks of conservative management showed no contrast media leakage.
Outcomes
Long-term success in resolving strictures by performing EBDs was achieved in two patients (14%). Strictures in both the patients, involved mid-esophageal segments, were long strictures, and intervals between the caustic agent ingestion and the first EBD in these patients were performed at two and five months, respectively. One of these patients received two EBD sessions (initial/maximum balloon diameter 10 mm/10 mm) over one month and the other eight sessions (10 mm/12 mm) over four months, respectively.
Temporary success of EBDs in resolving strictures was achieved in 17 out of 52 sessions (33%) and in eight out of 14 patients (57%). Two patients underwent no further sessions of EBD after their initial EBD because of persistent dysphagia or food intolerance after an EBD (n = 2) and incomplete balloon distension (n = 1). The remaining 12 patients underwent additional EBD sessions (range; 2-8 sessions) due to recurrent dysphagia. In these patients, dysphagia improved after an EBD and oral feeding was possible for variable periods of time between each EBD session.
There was no significant association between temporary success of EBD and type of caustic agent, location or type of esophageal stricture (Fisher exact test; p > 0.05). There was no significant difference between temporal success of EBD in resolving strictures and the size of the esophageal balloon, number of EBD sessions, interval between the time of ingestion of the caustic agent and the first EBD, age at first EBD, and the duration of EBD (p > 0.05); whereas, two patients achieved long-term stricture resolution after undergoing EBDs, as mentioned above. The 10 remaining patients that underwent additional EBD sessions experienced repeated stricture recurrence and as a result, had to undergo a surgical intervention.
Surgical intervention (segmental resection and anastomosis [n = 7], gastric tube interposition [n = 4], and esophagocologastrostomy [n = 1]) was performed due to persistent or recurrent dysphagia in 12 patients (86%). In these 12 patients, the time interval from caustic agent ingestion to surgical intervention ranged from four to 83 months (median: 7 months), whereas the time interval from the initial EBD to surgery ranged from one to 79 months (median: 4 months). Lastly, the time interval from the last EBD to surgery ranged from one to 16 months (median: 2 months). The histologic reports of nine patients (acid [n = 6], lye [n = 3] ingestion) were available. In all nine patients, dense fibrosis involving the submucosal and muscular layer of esophagus was seen.
DISCUSSION
Esophageal stricture is the most important late complication of corrosive esophagitis (16-19). At three to four weeks after injury, a stricture may form (19, 20). Because perforation, necrosis, and subsequent complications such as mediastinitis may occur during the acute or early states, EBD is usually started at least 1 month after corrosive injury (16).
Fluoroscopically guided EBD is generally considered a safe, easy, and effective means of treating a variety of esophageal strictures in children (7-13). Overall success rates of EBD have been reported to range from 67 to 98%, whereas the rupture rates have been reported to range between 0 to 9% (21-24). Perforation rates associated with EBDs are lower than those of bougienage due to the substantially lower shear forces generated during balloon dilatation (24, 25). However, the success rate of EBD in patients with corrosive esophageal stricture is low (29-70%) (2, 13, 15, 18, 26, 27), since corrosive esophagitis usually involves both esophageal and paraesophageal tissues (26). Furthermore, the rupture rate of EBD for corrosive esophagitis is higher (16-33%) (2, 26, 27) than for postoperative strictures (2, 26), because corrosive esophagitis increases tissue resistance and reduces tissue elasticity due to progressive fibrosis and dense scarring.
Because the natural course of severe, deep, and circumferential caustic esophageal burns is progressive and the remodeling period is protracted (6 to 24 months), feeding problems may occur during this period, and the established treatment modalities comprise a long-term dilation program and/or surgical treatment (11, 13, 15). Moreover, considering the progressive and long natural course of corrosive esophagitis, we defined long-term success of EBDs as dysphagia relief for at least 12 months after the last EBD. Serial EBDs may prevent esophageal tears or perforations by progressively stretching the organizing scar tissue and by reducing the risk of overstretching the strictures (11).
In the present study, all patients with focal strictures had ingested glacial acetic acid, and all patients who had ingested lye had long strictures.
Gundogdu et al. (27) reported that the success rate of EBDs in child cases of caustic esophageal stricture is higher in patients younger than eight years (80-96% versus 43%), and that EBD success rates are higher for strictures that involve the upper third of the esophagus (92%), strictures less than 5 cm in length (91%), and strictures caused by caustics materials (96-100%) other than lye (70%).
In the present study, EBDs were successful in two patients (14%) with a long stricture in the mid-esophagus caused by lye or acid ingestion. Although we cannot explain why this occurred, we presumed that the severity of esophageal wall involvement might be more related to the success of EBD than the length or location of involved segment. We did not find any relation between temporary success of EBD and location, type of stricture, number of sessions or interval between first and last EBD, although admittedly, our series was small. The long-term success rate of the EBD in the present study (14%) was lower than those previously reported in children (success was 48% in the study by Kukkady and Pease [14] and 70% in the study of Gundogdu et al. [27]), which may attribute to the severity of corrosive esophagitis. It is also possible that because EBDs were performed under conscious sedation and not under general anesthesia, our EBD procedure might not have been as aggressive. During conscious sedation, some patients bite the catheter or wire, so we inserted catheter transnasally. Recently, new approaches for corrosive esophageal strictures such have been reported. There is a report which cites the successful use of a cutting balloon to treat a caustic esophageal stricture in a 14-year-old boy (28). In a recent article (13), two patients underwent self-expandable metallic stent placement, however both experienced unsatisfactory outcomes. These techniques need further investigation using a larger number of patients and long-term follow-up period.
Because the use of the EBD in corrosive esophagitis has a high failure rate, surgical intervention is inevitably required in patients with progressive fibrosis and dense scarring (3, 11, 13, 15). Although limited long-term success was achieved by using EBD in this study, the EBD can have a role in allowing the children to eat per os until inflammation has subsided and the lesions have cicatrized prior to surgical management.
The present study has several limitations that require consideration. First, the study had a small population and statistical error should be considered. Second, we could not know the exact balloon pressure in each EBD session, because we inflated a balloon catheter manually instead of using an automatic balloon inflator with a pressure gauge. Third, because total number of EBD sessions and follow-up period was variable in each patient, there was a limitation in the evaluation of long-term effectiveness of the EBD.
In conclusion, only a limited number of children with corrosive esophageal strictures were considered cured by EBD. However, the outcome of repeated EBD was sufficient to allow the children to eat per os prior to surgical management.



 XML Download
XML Download