

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Popliteus is a flat muscle that forms the floor of the lower part of the popliteal fossa. The muscle arises within the capsule of the knee joint by a strong tendon, which is attached to a depression at the anterior end of the groove on the lateral aspect of the lateral condyle of the femur. It courses in an inferomedial direction within the popliteal fossa and finally inserts into the medial two-thirds of the triangular area above soleal line on the posterior surface of the tibia (1). Popliteus plays a role as major stabilizer of posterolateral knee. The biomechanics of the muscle is to resist the lateral rotation of the tibia on femur and to unlock the knee joint with lateral rotation of the femur on tibia.
In the region of the popliteal fossa, rare accessory muscles such as accessory slips of the medial and lateral head of the gastrocnemius muscle, the tensor fasciae suralis muscle (2), and the accessory semimembranosus muscle (3) have been well-studied. However, to our best knowledge, the accessory popliteus muscle was first reported by Duc et al. (4) in the radiology literature and any case has not been reported yet after that.
We encountered an extremely rare case of the accessory popliteus muscle, which was incidentally detected on MRI.
CASE REPORT
A 52-year-old man visited the hospital for right knee pain over the past one-month without any specific event. Physical examination revealed limited of motion of right knee joint and further examination is impossible due to knee pain. Plain radiography showed spur formation at right lateral tibial condyle.
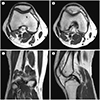
The right knee MRI was performed using a 1.5-Tesla MR (Achieva 1.5T SE; Philips, Amsterdam, the Netherlands). Intermediate-weighted turbo spin echo (TSE) sequences in the axial, sagittal, and coronal planes [repetition time (TR)/echo time (TE), 4000/36; slice thickness, 3.5 mm], intermediate-weighted fat-suppressed TSE sequence in the coronal plane (TR/TE, 4000/36; slice thickness, 3.0 mm), and T2-weighted fat-suppressed TSE sequences in the sagittal plane (TR/TE, 2270/60; slice thickness, 3.5 mm) were obtained. MRI findings of right knee showed the accessory muscle originating from the medial side of the lateral head of the gastrocnemius muscle (Fig. 1A). The muscle traversed from this origin, in an inferomedial direction, deep to the popliteal fossa, and anterior to popliteal vessels (Fig. 1B, C). Distally, the muscle inserted into the posteromedial articular capsule of the knee joint, slightly above the level of the insertion of the semimembranosus muscle (Fig. 1D). The signal intensity of the accessory muscle were similar to those of the adjacent muscles and the dimensions of the muscle belly measured 4.0 cm in length and 1.5 × 0.7 cm in thickness.
Additional MRI findings of right knee showed tears of both menisci and several cartilage defect lesions. The patient underwent arthroscopic total meniscectomy of the lateral meniscus. After operation, the knee pain improved and the patient was followed up at periodic intervals as an outpatient.
DISCUSSION
Accessory muscles are uncommon developing anomalies that represents additional distinct muscles analogous to the rest of the muscles of the body. A great variety of accessory muscles in the muscular system have been described in the anatomic, surgical, and radiologic literature. Most of them are generally asymptomatic and incidentally found, but in some cases, they may be the cause of clinical symptoms. Of the reported variations, especially in the lower extremities, the peroneus quartus muscle (5), the accessory soleus muscle (6), and the flexor digitorum accessorius longus muscle (7) are known as the most common anatomic variations.
There are rare accessory muscles in the region of the popliteal fossa, including accessory slips of the medial and lateral heads of the gastrocnemius muscle, the tensor fasciae suralis muscle, and the accessory semimembranosus muscle. Accessory slips of the medial and lateral heads of the gastrocnemius muscle may have different origin, respectively. An accessory slip of the medial head of the gastrocnemius originates from the intercondylar notch. This slip passes between popliteal artery and vein, and lastly joins with the medial head. An accessory slip of the lateral head of gastrocnemius originates from the distal femoral metaphysis, slightly medial to lateral head. This slip passes anterior and lateral to the popliteal vessels and inserts into the lateral head (8). From a clinical point of view, a close anatomic relationship between the accessory slip and the popliteal artery may result in popliteal artery entrapment syndrome (9). The tensor fasciae suralis muscle arises from the lateral side of the distal semimembranosus muscle within the popliteal fossa. This anomalous muscle body passes superficially from the popliteal fossa and terminates as an elongated tendon attached to the most superficial aspect of the Achilles tendon (2). The accessory semimembranosus muscle arises from the distal portion of the semimembranosus muscle and courses through the popliteal fossa. This accessory muscle does not have osseous insertion, but instead attaching to the proximal medial head of the gastrocnemius muscle (3).
Supernumerary muscle bundles of the popliteus muscle have demonstrated by anatomists (10). These bundles have been called various terms such as small popliteus or proximal popliteus, popliteus geminus, popliteus biceps, and double-headed popliteus. The bundle originates via an aponeurotic band or a short tendon either from a sesamoid bone of the lateral head of the gastrocnemius or from the proximal posterior aspect of the lateral femoral condyle. The distal part of the bundle merges with the popliteus muscle and some of its fibers may also insert at the posterior ligament of the knee joint. In our case, on the other hand, the accessory muscle is completely separated from the normal popliteus and no merger with its distal part. The accessory muscle is very similar to the normal popliteus muscle in that it is situated in the deep plane of the popliteal fossa as well as its course paralleling to the normal popliteus muscle. These imaging findings are identical to the case first reported by Duc et al. (4). However, there is limitation in naming of this accessory muscle. First no anatomical or surgical correlation was performed. So far, only one case has been reported in the radiologic literature. Second, the muscle has no share of origin or insertion with the normal popliteus muscle. This finding is inconsistent with the definition of the accessory muscle. Further studies are necessary in order to assess the entity of the muscle.
Although in the case reported by Duc et al. (4) the patient had no any symptoms, the authors hypothesized that because of the proximity of the accessory popliteus muscle to the adjacent structures such as popliteal vessels and tibial nerve, the muscle might result in clinical symptoms. In our case, the patient had the knee pain but the MRI showed meniscal tear and degenerative change of knee joint and the knee pain was improved after surgery, suggesting that the accessory popliteus muscle did not cause the pain.
In conclusion, the accessory popliteus muscle is an extremely rare anatomic variation that has so far reported only two cases, including our case. Due to its rarity, it is likely to be overlooked on knee MRI. Accordingly, when evaluating the muscles at the level of the popliteal fossa on MRI, careful evaluation of accessory muscles and precise determination of their anatomic relationship with surrounding structures may help the surgeon to make accurate surgical planning and prevent unexpected injury during operation.
 XML Download
XML Download