

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The gastrocnemius muscle is located along with the soleus muscle in the posterior compartment of the leg. The lateral head originates from the lateral condyle of the femur, whereas the medial head originates from the medial condyle of the femur. The muscle extends to about midway along the calf; the muscle fibers of the medial head extending lower than those of the lateral head and inserting into a broad aponeurosis. The distal end of the aponeurosis extends for a variable distance as a thin, tendinous sheet and receives the tendon of the soleus muscle to form the tendocalcaneus or the tendon of Achilles.
Anatomic variations in the attachment of the gastrocnemius muscle to the soleus muscle and variations of the medial head of gastrocnemius muscle have been well-studied, but it is difficult to find any reported case about an anatomic variation of the origin of the lateral head of the gastrocnemius muscle.
We encountered a rare case of an anatomic variation of the origin of the lateral head of the gastrocnemius muscle, which was detected as an incidental finding on magnetic resonance imaging (MRI).
CASE REPORT
A 29-year-old man visited the hospital with pain in both knees over the past 1 month. Six years previously he had undergone subtotal meniscectomy of his left lateral meniscus due to a meniscal tear. The pain in both knees occurred gradually without any specific cause and he had no history of trauma.
On physical examination, he had no tenderness, swelling, or range-of-motion limitation in either knee joint. X-ray showed no abnormality.
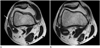
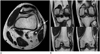
MRI of both knees was performed using a 1.5-T MR scanner (Achieva 1.5T SE, Philips, the Netherlands). An examination of the MRI scans revealed a variation in the lateral head of the gastrocnemius muscles of both knees. The lateral head of both gastrocnemius muscles originated from the posterior aspect of the lateral femoral condyle, but the lateral segment of the muscles originated from the iliotibial band (Figs. 1, 2). The other abnormalities were: complete lateral discoid meniscus in the right knee, and osteoarthrosis with lateral femoral condylar grade 2 cartilage lesions by the modified Outerbridge classification.
The patient underwent a left lateral meniscus transplantation and right lateral meniscoplasty for complete discoid meniscus. His pain disappeared after operation and he was followed up periodically as an outpatient.
DISCUSSION
Various anatomic variations of the gastrocnemius muscle have been reported previously, but mainly by cadaveric studies. The gastrocnemius muscle may have a sesamoid bone in its medial or lateral head, the two heads may be separable further down than usual, the tendon may be perfectly separated from that of the soleus muscle for a few inches, the lateral head may have a few lower fibers attached to the external lateral ligament or the posterior ligament of Winslow, a third head may arise from the popliteal surface of the femur, the entire muscle may be bilaminar, and the lateral head may be entirely tendinous (1). Cases of the bottom third of the gastrocnemius lateral head joining the lower two-thirds of the soleus muscle or the gastrocnemius muscle tendon joining the lower third of the soleus tendon have been reported as well (2).
Of the reported variations, a third head (caput tertium) is the most common variation of the gastrocnemius muscle. It arises from some part of the popliteal surface of the femur. It may also arise from: the linea aspera, the long head of the biceps femoris, the lateral epicondyle, the knee joint capsule, the midfibula, and the crural fascia. The third head may manifest clinically as popliteal artery entrapment syndrome (PAES) (3). A third head joining the medial head of the gastrocnemius muscle is most commonly cited as causing problems and occurs in 21% of patients with PAES (3, 4). As the third head originates from the popliteal surface of the femur, then passes lateral to the popliteal vessels and finally becomes inserted into the medial head of the gastrocnemius muscle, it compresses the popliteal nerve and vessels and causes intermittent claudication, arterial stasis and aneurysm, venous stasis, and impaired nerve function. However, an anomaly of the lateral head of the gastrocnemius muscle has been reported to be the cause in 34% of cases of PAES, including both abnormal insertion type and an aberrant accessory head (5).
In our case, the lateral segment of the lateral head of the gastrocnemius had an anomalous origin bilaterally from the iliotibial band. MRI findings of anatomic variations of the lower extremities, including the soleus, peroneus, flexor digitorum longus muscles and the medial head of the gastrocnemius muscle are well-known; but not for anatomic variations of the lateral head of the gastrocnemius muscle (5, 6, 7, 8, 9).
Kim et al. (10) reported anatomic variations of the lateral head of the gastrocnemius in pediatric patients. Anatomic variations of the lateral head of the gastrocnemius muscle were noted on MRI in 3.4% of patients, and lateral segmental anomalous origins of the lateral head were identified in 1.9% of patients. Of these, 56% patients had patellofemoral symptoms but there was no abnormality on MRI except a lateral segmental anomalous origin of the lateral head. Kim et al. (10) raised the possibility of the relationship between a lateral segmental anomalous origin of the lateral head of gastrocnemius muscle and lateral stability of the patella. Although this variation was not related to knee pain in our patient, further study will be needed to evaluate whether this variation is associated with knee symptoms.
In conclusion, the gastrocnemius muscle has a number of variable anatomic variations. MRI is an excellent means of detecting cases of anomalous muscles and determining their anatomic relationship with surrounding structures such as blood vessels and nerves. In addition, this information also helps the surgeon to prevent unexpected injury during surgery.
 XML Download
XML Download