

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Carcinosarcomas of the urinary system are very uncommon. To the best of our knowledge, there have been approximately 70 cases of carcinosarcoma of the urinary bladder and only 14 cases of carcinosarcomas of the ureter reported in the medical literature (123). Further, only 2 reports on carcinosarcoma of the urinary bladder and 1 report on carcinosarcoma of the renal pelvis and urinary bladder have been reported in the radiology literature (245). Therefore, we present the case of a histologically proven carcinosarcoma of the right ureter and the tumor extended to the urinary bladder, which was shown on computed tomography (CT).
Case Report
An 83-year-old man was admitted to our institution because of gross hematuria. A CT examination was performed and it showed an intraluminal mass in the right distal ureter and the mass was protruding into the lumen of the urinary bladder. The mass was slightly hyperattenuating relative to the urine on the unenhanced scan. On the contrast-enhanced CT scans, the tumor showed heterogeneous enhancement on the corticomedullary phase and it showed gradual enhancement on the nephrographic and pyelographic phases (Fig. 1). Ipsilateral hydroureteronephrosis and parenchymal thinning of the kidney were seen because of the right ureteral mass. There was no evidence of periureteral invasion, hepatic metastasis, or regional lymphadenopathy.
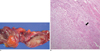
Based on the clinical and radiologic findings, our initial diagnosis was transitional cell carcinoma involving the right distal ureter and urinary bladder. The patient underwent right nephroureterectomy and transurethral resection for the ureteral and urinary bladder mass. The pathologic specimen of the right nephroureterectomy showed a relatively well circumscribed grayish yellow mass protruding into the lumen of the ureter with a relatively homogeneous cut surface. The tumor was 7 cm in length and there were areas of spotty necrosis (Fig. 2A). There was evidence of angioinvasion and invasion to the periureteric fat tissues. The pathologic specimen of the urinary bladder consisted with several pieces of hemorrhagic soft tissues.
Microscopically, these surgical specimens showed both malignant epithelial and stromal components. The predominant component consisted of undifferentiated sarcoma with small areas of squamous cell carcinoma (Fig. 2B). The immunohistologic features showed positive staining for cytokeratin and vimentin and these pathologic findings were all consistent with carcinosarcoma of the ureter and urinary bladder.
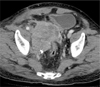
Repeat CT examination was performed 2 months after the surgery and it showed local tumor recurrence, and this presented as large heterogeneous mass in the right side of the pelvic cavity (Fig. 3). The patient underwent radiotherapy and he ultimately passed away 6 months after the surgery due to his poor general condition and pulmonary embolism.
Discussion
Carcinosarcomas are rare malignant and aggressive tumors that have both epithelial and stromal components (6). The malignant epithelial components are transitional cell carcinoma, carcinoma in situ, small cell carcinoma, adenocarcinoma and squamous cell carcinoma. The sarcomatous components are chondrosarcoma, osteosarcoma and leiomyosarcoma (3).
In the genitourinary system, these tumors usually occur in the postmenopausal uterus and they rarely occur in the urinary system (7). Carcinosarcoma usually presents in elderly patients in the sixth to seventh decades of life and they occur more often in men than in women. Clinically, patients with this tumor present with gross hematuria or with the signs and symptoms of ureteral obstruction (3). Since carcinosarcomas are high-grade malignancies and they have poor prognosis, aggressive treatment with nephroureterectomy is the only choice that has a chance for a cure. Adjuvant chemotherapy or radiotherapy does not offer any survival advantages (3).
Pathologically, carcinosarcoma of the ureter has features that are similar to those of transitional cell carcinoma, which is an intraluminal mass of a mucosal origin. The feature to differentiate well-differentiated transitional cell carcinoma from carcinosarcoma is that carcinosarcoma has no papillary projections of solid tumor. Radiologically, carcinosarcoma of the ureter can have similar features as transitional cell carcinoma as an intraluminal protruding mass.
There are only a few reports showing the radiological features of carcinosarcomas of the urinary system. One case of carcinosarcoma of the urinary bladder by Sumi et al. (4) contained the CT and MR findings. In that case, CT showed a homogeneously enhancing soft tissue mass with multiple calcific foci in the urinary bladder. MRI showed a mass with low signal intensity foci on both the T1 and T2 weighted images, and these foci corresponded to calcifications. Histologically, the calcifications were bone formations by the osteosarcomatous components. Those authors suggests that when calcifications or ossifications are seen within a bladder tumor on CT scan, the differential diagnosis should include bladder tumors with dystrophic calcification, hemangioma, osteosarcoma, carcinosarcoma with bone formation, and carcinoma with stromal osseous metaplasia (4).
Tekes et al. (2) reported on 3 cases of carcinosarcoma of the urinary bladder with the MRI findings. The masses were polypoid or sessile with single to multiple tumors. MRI showed isointense signal intensities compared to muscle on the T1 weighted images and the T2 weighted images showed heterogeneous signal intensities. These heterogeneous signal intensities on the T2 weighted images are not commonly observed in transitional cell carcinomas. After the administration of gadolinium, the enhancement was variable and the tumors did not showed early strong arterial enhancement, which is unlike transitional cell carcinoma. Those authors believed the gadolinium-enhanced images may be helpful to differentiate carcinosarcoma from transitional cell carcinomas of the urinary bladder (2).
One case of Yilmaz et al. (5) had carcinosarcoma of the renal pelvis and urinary bladder. The sonographic findings showed a large heterogeneous mass in the left renal pelvis and a small echogenic polypoid mass on the urinary bladder. CT showed a tumor with dimensions of 35 cm by 24 cm by 22 cm in the left renal pelvis. The tumor was heterogeneous and solid with large central low density areas. There was also a 1 cm sized small soft tissue sessile mass on the urinary bladder. Sonography and CT could not identify the normal renal parenchyma or the collecting system of the left kidney. Those authors suggested that this tumor was different from typical transitional cell carcinoma as carcinosarcoma of the renal pelvis and urinary bladder was centrally located with centrifugal expansion that presented with a uniform contour of the kidney and extrarenal spread at and through the renal hilum (7).
In our case, the urinary tract was examined using multiphasic CT and performing unenhanced and contrast-enhanced scans during the corticomedullary, nephrographic, and pyelographic phases. The attenuation values of the tumor were higher on the nephrographic and pyelographic phases than that on the corticomedullary phase and the values showed the gradual or persistent enhancement of the tumor. A study by Fritz et al. (8) investigated the attenuation differences of transitional cell carcinoma on MDCT scans during different phases. The result showed no significant differences between the mean attenuation values of transitional cell carcinomas on the corticomedullary, nephrographic and pyelographic scans. Since our case had a higher attenuation value during the nephrographic and pyelographic phases than during the corticomedullary phase, this might be helpful to differentiate carcinosarcomas from transitional cell carcinomas.
We report here on a case of carcinosarcoma of the ureter and urinary bladder and we present the CT findings of this tumor. If a heterogeneous intraluminal mass is seen on the ureter with extension to the urinary bladder with gradual enhancement, although it is rare, carcinosarcoma should be included in the differential diagnosis along with other common tumors such as transitional cell carcinoma.

 XML Download
XML Download