

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
T-cell non-Hodgkin lymphomas (NHLs) are biologically diverse, uncommon malignancies that represent approximately 12% of all NHLs (1). T-cell NHL includes a spectrum of disease most recently defined in 2016, according to the World Health Organization (WHO)/European Organization for Research and Treatment of Cancer classification (2). In the United States, cutaneous T-cell lymphoma (CTCL) and peripheral T-cell lymphoma (PTCL), not otherwise specified (NOS) are the most common mature T-cell NHL subtypes, accounting for 26.5% and 15% of cases, respectively (345). Mature T-cell NHLs may be indolent or aggressive; CTCLs are generally indolent, while PTCL-NOS is a “wastebasket” category of aggressive nodal lymphoma. Precursor T-cell lymphoblastic lymphoma (T-LBL) is a highly aggressive disease, representing 14% of lymphoblastic lymphoma typically characterized separately from mature T-cell NHL subtypes (5). Numerous other T-cell NHL subtypes have been described, each with characteristic histopathologic features and clinical behavior.
Imaging plays an important role in staging and management of many T-cell NHLs. CT is the most commonly used tool for staging and follow-up as it is readily available, easy to perform, reliable and reproducible (6). However, nodal involvement by CT is limited to assessment of node size and shape, and it may poorly depict involvement of bone marrow and some extranodal sites (78). 18F-flourodeoxyglucose (FDG) positron emission tomography CT (PET-CT) is increasingly used for staging and response assessment, particularly for aggressive lymphomas due to its superior sensitivity. PET-CT improves detection of extranodal involvement and accuracy of baseline staging compared with CT alone (910). Evidence also supports the utility of PET-CT in treatment response assessment, facilitating timely optimization of appropriate treatment regimens (1112). Magnetic resonance imaging (MRI) is employed in the diagnosis and follow-up of extranodal NK/T-cell lymphoma and subcutaneous panniculitis like T-cell lymphoma, due to superior soft tissue contrast in the nasal cavity and subcutaneous tissues, respectively (1314). The purpose of this review is to familiarize radiologists with clinical features and imaging manifestations of T-cell NHL as well as the role of CT, PET-CT and MRI in the management of common subtypes.
Subtypes of T-cell NHLs
Cutaneous T-cell Lymphoma
Mycosis Fungoides/Sézary Syndrome
Mycosis fungoides (MF) and Sézary syndrome (SS) are the most common subtypes of CTCL, which account for approximately 6% of NHLs (515). These entities present with skin involvement and are to be distinguished from other T-cell lymphomas which may involve the skin, to be discussed later (16). MF is generally indolent, and diagnosis is based upon clinical findings of erythematous patches/plaques often originating on the trunk as well as histopathologic findings of neoplastic CD3+ and CD4+ T-cells in the skin (17). Affected patients may have had several years of skin lesions confused with benign entities, even on biopsy due to accompanying non-malignant inflammatory infiltrates. Multiple skin biospies may be necessary for diagnosis. Skin lesions progress from patches to plaques to cutaneous tumors. SS may evolve from MF or can present de novo, characterized by skin rash and malignant lymphocytes within the peripheral blood (Sezary cells) (16). Extensive skin involvement, peripheral lymphadenopathy and visceral disease may be present. In contrast to MF, SS is more symptomatic and is associated with lower remission and survival rates.
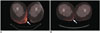
In MF, patients with only cutaneous lesions including erythema, patches, and/or plaques may demonstrate no imaging/CT abnormalities. If the disease progresses to form a discrete mass, then skin thickening or a mass is seen on CT if one is performed (18). In the context of clinical trials, CT is advised when it is important to fully stage participants and have the ability to assess response (19). Repeat examinations may not be needed in patients with clinically early disease, while follow-up imaging is useful in advanced disease to detect response to treatment and progression, especially in terms of nodal or visceral involvement. PET-CT is not routinely performed in MF/SS, though it has been shown more sensitive than CT in detecting nodal involvement and defining reactive versus malignant nodes (91820). In one report, PET-CT was shown useful for more accurate measurement of skin lesion thickness and nodal staging, both of which have been correlated to outcomes (Fig. 1) (18). Imaging contributes to accurate staging in advanced CTCL, whereby tumor lesions indicate stage IIB, erythroderma in the absence of nodal or visceral disease indicates stage III, histologic lymph node involvement, irrespective of T stage represents stage IVA, and visceral disease represents stage IVB, irrespective of T and N stage. It is important to detect lymphadenopathy and/or other visceral organ involvement since survival rates decrease dramatically with visceral involvement. Pulmonary involvement is the most common extra-nodal involvement of CTCL, associated with poor outcomes (2122).
Several long-term prognostic studies have revealed that patients with early CTCL have a favorable prognosis. In fact, patients with stage IA disease may have complete resolution of skin lesions with treatment, which may include psoralen and ultraviolet A radiation, electron-beam radiation, topical and other treatments (16). However, patients with advanced CTCL have a poor prognosis despite intensified therapy including systemic chemotherapy. The extent of cutaneous involvement (ranging from T1–T4) is significantly associated with prognosis and disease progression. One large study found that the risk for disease progression at 5 years was 10% in T1, 22% in T2, and 48% to 56% in T3 to T4 levels of cutaneous involvement (23). For treatment response assessment, PET-CT can be used to monitor lymph nodes that are 18FDG-avid but do not meet the size criteria for staging (182425). In addition, changes in 18FDG uptake in the form of maximum standardized uptake values (SUVmax) can potentially impact patient management (18).
At present, CTCL treatment is not based on specific genetic or molecular targets. However, altered molecular pathways and genetic drivers are being discovered and studied, to better understand the pathogenesis of this disease and to identify potential targets for treatment, including mutations in the T-cell receptor complex, nuclear factor-κB, and the Janus kinase/signal transducer and activator of transcription signaling pathways (26). Biomarkers are sought to guide management in targeted and non-targeted treatment settings.
Large-Cell Transformation in Cutaneous T-Cell Lymphoma
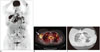
Mycosis fungoides may undergo a process of large cell transformation (LCT), which is characterized by more aggressive disease, in up to 39% of MF patients (Fig. 2) (2728). LCT is defined histopathologically by the presence of large cells that are at least 4 times the size of lymphocytes exceeding 25% of the cell populations (29). LCT can occur in any stage of CTCL, however, it more frequently occurs in advanced stages. LCT is commonly found in skin tumors but may occur at any involved site, such as nodes (29). PET-CT may be useful in patients with suspected LCT. According to Feeney et al. (9), average SUVmax of cutaneous lesions in LCT is significantly higher compared to those in MF or SS without LCT. The prognosis of LCT is significantly worse than MF. In one report, median survival of LCT patients from initial diagnosis of MF/SS was 37 months, compared with 163 months in patients with no transformation (30). It is recommended that any patient with MF who develops new papules receive a biopsy to evaluate for LCT and subsequent PET-CT. If LCT is confirmed, patients are treated more aggressively, with systemic chemotherapy and possibly autologous or allogeneic hematopoietic cell transplantation (HCT) and/or radiation (29).
Peripheral T-Cell Lymphoma, Not Otherwise Specified
Peripheral T-cell lymphoma, NOS is a heterogeneous group of predominantly nodal T-cell lymphomas. It is the most common subtype of PTCL, accounting for approximately 30% of PTCL and approximately 4% of NHLs overall (5). PTCL NOS is usually aggressive and relapse is common. Most patients present with generalized lymphadenopathy with or without extra-nodal disease, including involvement of skin, gastrointestinal tract, liver, spleen or marrow (3132333435). Approximately 60% of patients with PTCL NOS have stage IV disease at the time of diagnosis (35). Diagnosis of PTCL NOS is made based upon the results of a tissue biopsy, usually of a lymph node. However, because PTCL NOS is essentially a diagnosis of exclusion, the diagnostic agreement rate among expert hematopathologists in one report was only about 75% (33). Gene expression profiling studies have identified subtypes of PTCL NOS with differing clinical behavior and response to therapy (236).
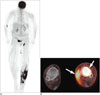
On CT, generalized lymphadenopathy is the most common finding in PTCL NOS. The imaging appearance is generally not distinguishable from other types of lymphoma. On PET-CT, PTCL NOS is often 18FDG-avid, as seen in 33 of 34 patients in one report with SUVmax ranging from 2.8 to 42.3 (mean 12.3) (Fig. 3) (9). According to the Lugano classification guidelines, which are the most recent recommendations for initial evaluation, staging, and response assessment of Hodgkin and NHL, PET-CT is recommended for routine staging of 18FDG-avid, nodal lymphomas (37). It may become more commonly used in PTCL NOS.
The standard treatment for PTCL NOS is a conventional-dose systemic anthracycline-containing chemotherapy (3). The role of HCT is still investigational and the potential benefit of HCT is difficult to ascertain due to reports combining PTCL subtypes and disease rarity (38). Poor prognostic factors in PTCL NOS include age > 60, performance status ≥ 2, elevated lactate dehydrogenase (LDH) and bone marrow involvement (39). According to one multicenter study, the cumulative 5-year overall survival of PTCL NOS was 43% (39). Attempts have been made to identify biologically and prognostically distinct subgroups within the heterogeneous PTCL NOS category. For example, Epstein-Barr virus (EBV) is found in approximately 30% of all cases of PTCL NOS and may be associated with a more aggressive course (40).
Angioimmunoblastic T-Cell Lymphoma
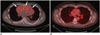
Angioimmunoblastic T-cell lymphoma (AITL) is a rare subtype of PTCL, which accounts for 1–2% of NHLs and 15–20% of PTCLs (3). It is more common in elderly, and patients often present with an acute onset systemic illness including B symptoms, generalized lymphadenopathy, and hepatosplenomegaly at the time of diagnosis. The CT features are nonspecific and similar to those of any disseminated lymphoma. The lesions usually exhibit high 18FDG avidity (Fig. 4) (41). AITL is generally an aggressive disease, although occasional spontaneous remissions are seen. Relapse is frequent and overall survival is low, reportedly 32% in one report (42).
Anaplastic Large Cell Lymphoma, Primary Systemic Type
In the WHO classification, systemic anaplastic large cell lymphoma (ALCL) can be divided into two subgroups on the basis of the expression of anaplastic lymphoma kinase (ALK) protein. ALK-positive ALCL is characterized by a chromosomal translocation linking the ALK kinase gene on chromosome 2 to the nucleophosmin gene on chromosome 5, resulting in a constitutively active tyrosine kinase (43). The distinction of ALK-positive and ALK-negative ALCL is important because of clinical and prognostic differences. Namely, ALK-positive ALCL is more common in younger patients who generally have superior outcomes when treated with standard chemotherapy as compared to patients with ALK-negative ALCL (43). ALK-positive ALCL patients typically have 5-year overall survival rates of more than 70%, whereas patients with ALK-negative ALCL have 5-year overall survival rates less than 50% (4344).
Patients with ALCL often present with painless lymphadenopathy, with or without extra-nodal involvement (Fig. 5). One study has shown differences in extra-nodal sites involved in ALK-positive and ALK-negative ALCLs: bone marrow, bone, subcutaneous tissue, and splenic involvement were seen at more commonly in ALK-positive patients, whereas skin, liver, and gastrointestinal involvement was more frequent in ALK-negative ALCL (43). The degree of 18FDG uptake is higher in ALK-positive ALCL than in ALK-negative ALCL, suggesting that PET may be useful in distinguishing between the two groups (45).
Extranodal NK/T-Cell Lymphoma
Extranodal NK/T-cell lymphoma is most common in Asia and in native populations of Central and South America, and it is rare in the United States and Europe (346). It is strongly associated with EBV infection. 60–80% patients present with localized disease involving aerodigestive tract, resulting in symptoms of nasal obstruction, epistaxis and/or destructive mass involving the nasal cavity, sinuses or oral cavity (47). Lymph nodes may be involved secondarily but are rarely the primary site of involvement. Extranasal involvement is common in soft tissues/skin, the gastrointestinal tract, lungs, adrenal glands, testes or central nervous system (CNS) (47). Extranasal extranodal NK/T-cell lymphoma is associated with more aggressive features in terms of advanced stage at presentation, poorer performance status of affected patients, inferior response to chemotherapy and poorer survival (4748).
On CT, tumors show soft tissue attenuation with mild to moderate heterogeneous enhancement. MRI is better demonstrating the extent of lesion as compared to CT, especially in the nasal type (Fig. 6) (49). Signal intensity of tumors is higher than that of muscle but lower than that of sinonasal mucosa on T2-weighted spin-echo images. On T1-weighted spin-echo images, tumors show similar to higher signal intensity than that of muscle. PET-CT is a useful tool for initial diagnosis and staging, because both nasal and extranasal lesions exhibit high 18FDG avidity (Fig. 7) (415051). Radiotherapy has been validated as primary treatment for localized nasal NK/T-cell lymphoma in several large retrospective studies (5253545556). As expected, patients with early stage disease have a better prognosis as compared to patients with advanced disease.
Subcutaneous Panniculitis Like T-Cell Lymphoma
Subcutaneous panniculitis-like T-cell lymphoma (SPTCL) is a rare subtype of peripheral T-cell lymphoma, accounting for less than 1 percent of all NHLs (3). Patients with SPTCL typically present with one or more usually painless nodules or poorly circumscribed indurated plaques most commonly located on the trunk or lower extremities (5758). Initial diagnosis of SPTCL is often delayed because inflammatory or infectious processes may be suspected both clinically and on imaging. MRI features of SPTCL include nodular or mass-like enhancing areas that infiltrate the subcutaneous tissues (Fig. 8) (14). Central areas of intermediate T2-weighted signal intensity (compared to muscle) may be seen, which can be useful in differentiating SPTCL from other inflammatory or infectious processes (14). Both CT and PET-CT are useful for recognizing other organ involvement and evaluating the extent of disease (4059). Whole body MRI has also been suggested as a useful tool at initial diagnosis and follow-up, to assess the extent of disease and monitor a patient's response to therapy (60). The clinical course of SPTCL can be indolent with relapsing panniculitis, or aggressive with the development of a hemophagocytic syndrome which can be fatal. Favorable (αβ) and poor (γδ) prognostic phenotypes have been described (57).
Precursor T-Cell Lymphoblastic Lymphoma
Precursor T-cell lymphoblastic lymphoma is a rare but highly aggressive neoplasm of lymphoblasts of T-cell origin, with an incidence of approximately 2% of adult NHLs. Patients are commonly young adults who may present with lymphadenopathy in the cervical, supraclavicular, and axillary regions and/or bulky mediastinal masses (Fig. 9) (616263). Superior vena cava syndrome, tracheal obstruction and pleural and/or pericardial effusions may be associated (64). Extranodal disease (e.g., involvement of the skin, testis, liver, spleen and/or bone) is a less common presentation. Central nervous system involvement more commonly occurs in patients with bone marrow involvement.
Imaging studies such as total body CT scan (head and neck, thorax, abdomen, and pelvis) and PET-CT are used for staging and therapeutic response evaluation. For post induction response assessment, CT scan is useful for evaluation of intrathoracic and abdominal disease involvement. Mediastinal mass assessment is important in T-LBL, as residual masses can remain after treatment and mediastinal relapses can occur. Most T-LBL exhibit high 18FDG avidity on PET-CT at baseline, prior to the start of treatment (9406264). Although PET did not predict long-term outcome in previous retrospective studies (6566), PET-negativity is useful because it may eliminate the need for intensification of chemotherapy or mediastinal irradiation.
A variety of therapeutic approaches in T-LBL have been reported, including chemotherapy protocols for high grade NHL and HCT. Complete response rates of greater than 80% and a disease-free survival rate of 56% have been reported in adults treated with intensive/acute lymphoblastic leukemia-type regimens (616768). While prognostic models are not yet defined for adult T-LBL, poor risk features in adults include age > 30 years, advanced stage III or IV disease, high LDH level (more than 1.5 times normal), involvement of central nervous system, bone marrow or mediastinum (676970). Patients with poor risk features are potential candidates for intensified therapy and HCT (1468). Song et al. (71) achieved higher event free survival and overall survival in T-LBL patients who proceeded to HCT compared to patients treated with chemotherapy alone. Disease relapse has been reported as a leading cause of death after HCT, followed by infections, graft-versus-host disease, respiratory, cardiovascular and other treatment-associated complications (Fig. 10) (7273).
CONCLUSION
T-cell NHLs include a wide spectrum of diseases ranging from indolent to highly aggressive, associated with varied clinical features and prognosis. It is important to have familiarity with common subtypes of T-cell NHL, including the expected clinical courses and prognostic factors, to best interpret imaging studies and guide management in affected patients. Specifically, cutaneous disease is often indolent; nodal and/or visceral involvement indicates the need for more aggressive treatment. PTCL NOS is a common subtype, often aggressive. Precursor T-LBL is aggressive, with poor prognosis. Imaging studies including CT, MRI and PET-CT have important and specific roles in the various entities, not only for staging but also in response assessment and detection of disease-related and treatment-related complications.






 XML Download
XML Download