

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Osteoporotic vertebral compression fractures (VCFs) pose an array of clinical problems including pain, spinal deformities, reduced mobility, and an overall increase in mortality in elderly patients. The conservative treatment of VCFs consists of analgesics, bed rest, and bracing. However, this immobilization can lead to a further reduction in bone mass. Alternatively, surgical stabilization with an internal fixture represents a large burden to elderly patients. The principal limitation of vertebroplasty is cement extravasation, the rates of which are as high as 30% (1). Moreover, the vertebroplasty procedure does not easily restore the height of the collapsed vertebral body. The Balloon Kyphoplasty procedure involves the insertion of an inflatable bone tamp to restore the vertebral body height, thus creating a cavity to be filled with bone cement. In order to reduce the risk of extravasation, cement augmentation is performed in a controlled, low pressure environment in the preformed cavity. In this study, we evaluated the efficacy of fracture reduction and the safety of using a Sky Bone Expander (Disc-o-tech Ltd, Herzliya, Israel) for the treatment of painful osteoporotic VCFs. This expansion, which uses a mechanical rather than hydraulic expandable rigid polymer device, as used in the balloon kyphoplasty, enables improved control over the device's position and expansion direction. We also examined the rate of cement extravasation and early patient outcomes.
MATERIALS AND METHODS
Patients
The 26 patients enrolled in this prospective study with pain-causing osteoporotic VCFs (6 men, 20 women), were seen between April 2005 and May 2007. The study protocol was approved by Changzhou No. 2 Hospital's Ethics Committee and informed consent was obtained from all patients before the procedure. The mean patient age was 65.5 years (range: 58 - 90 years). A total of 35 procedures were performed in 26 patients. The fractures occurred between the T8 and L5 vertebrae: T12 - 12 cases; L1 - 11 cases; T11 - 4 cases; L2 - 2 cases; T8-10 and L3-L5 - 1 case, respectively. Of the patients treated with the Sky Bone Expander, 20 were treated for a single VCF, whereas six were treated for multiple VCFs (2-4 vertebrae). Magnetic resonance imaging (MRI) was used to confirm the presence of an acute fracture associated with pain, as well as burst-type injuries with slightly retropulsed bone. The signs of a fracture on the MRI included a higher intensity signal in T2-weighted images and a weaker intensity signal in T1-weighted images. The diagnostic criteria for painful VCFs included obvious back pain and image examination at one or more levels, and low bone mineral density (BMD) with a T-score less than -2.5 (determined by standard dual-energy X-ray absorptiometry) (Explorer QDR, Hologic Inc. MA). Contraindications for the application of this procedure included fractures that did not cause pain, fractures with a big retropulsed bone, and patients afflicted with other diseases which rendered them unable to tolerate the operation. The initial number of VCF patients was 31; however, three patients with vertebral fractures accompanied with spinal cord compression and two patients with severe cardiovascular or pulmonary diseases were excluded due to the inability to tolerate a prone position.
Procedures
The Sky Bone Expander is a device made of a highly rigid polymeric material. In the contracted configuration, it is 4 or 5 mm in diameter and can be inserted via a pedicle cannula into the vertebral body. In turn, its fully expanded shape is a trapezoid or cubic configuration with a maximal diameter of 14 or 16 mm. This shape elevates the endplates restoring the vertebral body height (Fig. 1). The procedures were carried out as described previously (2-4). In brief, all procedures were performed in the operation room with the patient positioned in the prone position with the spine extended. The skin and subcutaneous tissues were locally anesthetized with 1% lidocaine. The proper placement of the Sky Bone Expander involved identifying the transpedicular entry point into the vertebral body using a guide pin and with the aid of fluoroscopy. A hand-mounted drill bit was then used to ream a corridor for insertion of the device. With the guide of a lateral radiograph, the radiopaque polymer tube was ideally situated under the collapsed endplate (Fig. 2A). The creation of the cavity for injection of bone cement was achieved by radial expansion (Fig. 2B), followed by the contraction and removal of the SKY Bone Expander. Furthermore, with the aid of continuous fluoroscopic guidance, bone cement was injected into the created cavity through the implant core (Figs. 2C, D). Cement filling was stopped when the cement mantle reached two thirds of the way back to the posterior vertebral body cortex or when cement extrusion was observed on the lateral fluoroscopic images. The same procedure was repeated on the opposite side of the vertebra if necessary. A single procedure can treat 1-4 vertebral levels, with an average bone cement injection volume of 3.5 mL (range, 2.5-5.0 mL) per vertebrate level.
Assessment of Cement Leakage
Postoperative radiographs were examined for the presence of cement leakage by looking at vertebral position and the possible correlation with any postoperative clinical symptoms.
Radiographic Assessment of the Sagittal Alignment Restoration
All radiographs performed in this study were independently evaluated at one week after surgery by two unbiased researchers who were not involved in the care of these patients. The parameters measured included the Cobb angles across the fractured level, the preoperative and postoperative anterior height (AH), midline height (MH), and posterior height (PH) of the fractured vertebra on a lateral radiograph in the standing position. To determine the Cobb angle, measurements were taken from the superior endplate of the vertebra from one level above the treated vertebra to the inferior endplate of the vertebral body at one level below the treated vertebra (5). The vertebral height of the fractured vertebra was defined as the distance between corresponding points on the superior and inferior endplates at the posterior, middle, or anterior locations (Fig. 3).
Assessment of Early Outcome
The postoperative follow-up time ranged from 3 to 6 months, with an average of 4.5 months. Patients completed the questionnaire of the Visual Analog Scale (VAS) and ambulation status, as well as undergoing a follow-up comprehensive neurologic examination at 1 day, 1 week, 1 month, and 3 months after the procedure. Moreover, patients also rated back pain on a VAS, in which "1" indicated no pain, and "10" indicated severe pain. Lastly, patient ambulation status included full ambulation, assisted ambulation, and no ambulation. The SPSS 11.5 software package (Chicago, IL) was used as a data analysus tool. Paired t-tests were used to compare the pre-operation and post-operation data.
RESULTS
Early Clinical Outcome
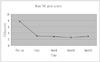
All of the 26 studied patients tolerated the bone expansion procedure well. The average operative time was 42.4 ± 15.5 min per vertebra. As well, all patients also experienced some degree of pain relief and improvements in mobility within the first 24 hours after surgery. The mean patient VAS score significantly improved from 7.7 ± 1.8 before surgery to 3.1 ± 2.0 at 1-day (p < 0.01), 2.9 ± 1.7 at 7-days (p < 0.01), 2.6 ± 1.5 at 1-month (p < 0.01), and 2.9 ± 1.3 at 3-months (p < 0.01) after surgery, respectively (Fig. 4).
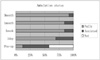
The patients' mobility significantly improved after the operation (p < 0.01). Further, the proportion of fully ambulatory patients increased from 12% before surgery to 69% at 1-day and 92% at 3-months after surgery, respectively (p < 0.01) (Fig. 5).
Restoration of the Sagittal Alignment
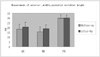
The radiologic height measurement of all the 35 vertebrae treated demonstrated that the Cobb angle improved from an mean angle of 18.5 ± 8.2 degrees before surgery to 9.2 ± 4.0 degrees after surgery (p < 0.01). The anterior vertebral height significantly increased from 18.4 ± 5.1 mm before surgery to 20.5 ± 5.3 mm after surgery (p < 0.01). The midline height significantly increased from 15.5 ± 5.2 mm before surgery to 18.9 ± 4.0 mm after surgery (p < 0.01). The posterior heights remained unchanged (29.9 ± 3.5 mm and 30.2 ± 3.2 mm before and after surgery, respectively) (p > 0.05) (Fig. 6).
Cement Extravasation
In all cases, a cavity was successfully created in the treated vertebral body. Minor cement extravasations were observed in 4 out of 35 procedures, but none of the leakages were associated with any clinical consequences. These leakages included one in the epidural space, one in the disc space, and two in the paraspinal tissues or paravertebral veins (Fig. 7).
DISCUSSION
Osteoporosis is a systemic disease resulting from progressive bone mineral loss and changes in bony architecture, which leaves the spinal column vulnerable to VCFs. Moreover, painful osteoporotic VCFs can be a significant burden for patients, causing impairment of physical function and quality of life. VCFs lead to progressive sagittal spine deformities and changes in spinal biomechanics which are believed to contribute to a fivefold increased risk of further fracture (6).
The conservative treatment for the occurrence of pain-causing VCFs includes analgesic medication, bed rest, and back braces, which do not address spinal deformity. Further, the pain and disability may be prolonged while the fractured vertebral body heals (7). In most cases, vertebral stabilization by open surgery was not indicated because of increased risk for the patients and unsatisfactory results, such as pulled out and lost screws in weak bone. In contrast, the vertebroplasty and kyphoplasty are particularly advantageous because of their short surgical time, rapid pain relief and minimal recovery period (8, 9). Moreover, a vertebroplasty used in osteoporotic VCFs, involving the percutaneous injection of cement directly into the fractured vertebra, has been reported to be effective in improving VCF associated pain (10-13). Limitations in these procedures include the inability to address the kyphotic deformity and a substantial risk of extravertebral cement leakage resulting from the high-pressure cement injection. A balloon kyphoplasty attempts to restore spinal alignment via a lower pressure placement of cement into the cavity created in the vertebral body by a tamp. As previously published results, the kyphoplasty results in considerably less cement extravasation than vertebroplasty (14-18). Hence, the kyphoplasty is an effective procedure in the improvement of kyphotic deformities in some patients, as well as rapidly reducing the pain associated with VCFs in a majority of patients (8, 13, 16, 19). The long-lasting effect of pain relief of balloon kyphoplasty could be attributed to the improved sagittal profile of the spine, which results in a lower compensating activity of the muscles (9, 16).
Vertebral expansion using the Sky Bone Expander is a new therapeutic intervention procedure for painful osteoporotic VCFs. This procedure differs from a conventional vertebroplasty and balloon kyphoplasty in that the device is advanced into the fractured vertebral body, the Expander is unsheathed to reduce the fracture and elevate the endplates, and then is resheathed to produce a cavity to be filled with bone cement (4). This expansion using an expandable rigid polymer device, rather than the hydraulic one used in balloon kyphoplasty, enables improved control over the device's position and expansion direction as well as eliminates risk of device failure. This Bone Expander always expands to the same predefined shape and size, which is highly beneficial in treating vertebral fractures which require reconstruction controllability. As it expands, the expander attains a cobble shaped structure. This structure, coupled with the gradual and controlled expansion of the device, lowers the risk of endplate penetration. It expands mostly in height, therefore steering clear of the lateral and anterior walls. The device is manually and mechanically expanded, and can therefore be expanded to the extent the physician deems necessary. By monitoring the device expansion and the vertebral height restoration by fluoroscopy, the physician can determine whether to expand the device to its full diameter, or to stop the expansion before the full diameter is reached. In addition to it versatility, the Sky Bone Expander is quite easy to use, safe, and has a high degree of controllability compared to the other examined procedures
In the present study, asymptomatic cement extravasation occurred for an average of 11% of the vertebra treated, which is similar to the balloon kyphoplasty (9.8 - 11.3%), and is considerably lower compared with the vertebroplasty (14-18). This supports the fact that the injection of high-viscosity cement at low pressure into a previously formed cavity is a significant improvement over the injection of low-viscosity liquid cement at high pressure into the unreduced vertebral body.
The restoration of normal overall spinal sagittal alignment in elderly patients with a VCF and kyphotic deformity has obvious benefits (4). In this series, an improvement in the spinal sagittal alignment and vertebral body height was achieved in the majority of patients. A mean of 9.3° of correction of local spinal kyphosis was achieved with Sky Expander, is similar to 8.8° of balloon kyphoplasty (19).
The rapid relief of pain after the bone expanding procedure was associated with the effect of bone cement and the stabilization of the vertebral body. Patients in this study exhibited a rapid decrease in pain, with a significant improvement of the VAS score after surgery. The proportion of patients also increased with a high degree of patient satisfaction. The degree of satisfaction was similar to the observed level of procedure satisfaction in the vertebroplasty and balloon kyphoplasty. Additionally, operative time and cost of this technique was less than the balloon kyphoplasty, and the complications were as infrequent as the balloon kyphoplasty (3, 18, 19).
The treatment of VCFs with the Sky Bone Expander device is a safe, effective, and minimally invasive procedure, which provides satisfactory short-term clinical efficacy.
The present study has some limitations, such as the low number of patients and number of fractures treated. A long-term follow-up would be required to further evaluate the efficacy of this device.




 XML Download
XML Download