

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A breast cholesterol granuloma is an uncommon, benign, nodular breast lesion generally found during a pathological evaluation of abnormalities detected from screening. Clinically, these lesions may be indistinguishable from breast carcinomas. Although there have been several English language clinical reports regarding breast cholesterol granulomas (1234567), to our knowledge, no report has described the features evident on dynamic computed tomography (CT). One study has reported the lesion features evident on a non-enhanced CT (7). Here, we present a case of breast cholesterol granuloma detected incidentally on a dynamic abdominal CT. We describe the clinical, radiological, and pathohistological findings of the granuloma as well.
CASE REPORT
Clinical and Radiological Findings
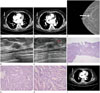
A 78-year-old woman presented for a kidney evaluation and a 1 cm diameter, oval, ill-defined enhancing mass was incidentally found in the mid-outer portion of the right breast on a dynamic abdominal multidetector CT (Sensation 16; Siemens Medical Solutions, Forchheim, Germany). In precontrast imaging, the lesion was not fully scanned, but the density of the partly visualized mass was the same as that of the surrounding breast tissue. We obtained early and delayed phase images 25 and 90 seconds after administering an intravenous contrast solution, respectively. The lesion became progressively heterogeneously enhanced, with no associated skin thickening or infiltration of the surrounding tissue (Fig. 1A, B).
The personal and family breast medical history was unremarkable. On physical examination, no palpable abnormality was evident in the right breast and no axillary lymphadenopathy was noted. Mammography revealed a 1 cm diameter, oval, indistinct hyperdense mass lacking microcalcification, in the mid-outer portion of the right breast, corresponding to the enhancing mass evident on the dynamic abdominal CT (Fig. 1C). Right breast ultrasonography revealed an oval isoechoic mass with a partially angular margin, but without increased tumor-associated vascularity on color Doppler imaging (Fig. 1D, E). The lesion was categorized as Breast Imaging Reporting and Data System category 4B. An ultrasound-guided 16 gage-core needle biopsy was performed and five 1-2-mm-diameter tissue specimens were obtained.
Pathological Findings
The biopsy revealed a relatively well-circumscribed lesion composed of numerous cholesterol clefts, aggregations of foamy histiocytes, a few foreign-body-type multinucleated giant cells, with hemosiderin, and lymphohistiocytic infiltration evident on hematoxylin-and-eosin staining (Fig. 1F-H). These findings were consistent with a cholesterol granuloma. The patient refused surgery.
Follow-up CT
Fifty days after the lesion was detected incidentally on an abdominal CT, a contrast-enhanced chest CT was performed due to the patient's respiratory symptoms; the biopsy-proven cholesterol granuloma was found to have decreased in diameter from 1 cm to 0.6 cm (Fig. 1I).
DISCUSSION
Cholesterol granulomas occur predominantly in the mastoid process of the middle ear cavity and consist of fibrous granulation tissue containing cholesterol crystals surrounded by foreign-body-type giant cells. Such granulomas are rare in the breast. The pathogenesis remains unclear, but is thought to involve duct ectasia and rupture. Lipid-rich material from damaged ductal lumens is released into the periductal parenchyma, causing the formation of cholesterol crystals accompanied by a massive foreign-body inflammatory reaction (12). However, some researchers have suggested that the pathogenesis features fat necrosis (68).
One review of eight breast cholesterol granuloma cases found that five exhibited ectasia of the adjacent mammary ducts (3). We found no pathological evidence of ectasia, possibly because we studied needle-biopsied tissue only. The other three cases of the study lacked histologically confirmed duct ectasia of the surrounding breast tissue as well (3). In a different report, several granulomas were found to occur in the peripheral breast parenchyma, whereas the duct ectasia was centrally located (4). One of the two granulomas that Bezić and Piljić-Burazer (5) studied was located on the periphery of the breast parenchyma; histologically, the surrounding breast tissue showed no evidence of an inflammatory reaction around the breast ducts. They suggested that the spontaneous rupture of a breast macrocyst into the adjacent breast parenchyma had triggered granuloma formation.
To our knowledge, except for a single report that described the non-enhanced CT features of a cholesterol granuloma (7), only the mammographic and sonographic features of this disease entity have been described radiologically (347). Mammographically, such granulomas present as variably-sized, ill-defined masses with or without calcification. Ultrasonographically, the lesions present as lobular or irregular hypoechoic masses or intracystic masses (347). Importantly, a cholesterol granuloma may be indistinguishable from a breast carcinoma clinically and radiologically. Breast cancers have been evaluated using dynamic contrast-enhanced CT (910). In the cited studies, irregular and spiculated margins, an irregular shape, and rim enhancement were the features best predicting malignant breast lesions (9). Early enhancement and washout patterns on post-contrast images were highly predictive of, and sensitive to the detection of, malignant breast lesions (910). However, our case exhibited persistent enhancement. Furthermore, the diameter of the lesion decreased rapidly after the core needle biopsy, in contrast to the behavior of malignant lesions.
In summary, we report the dynamic CT features of a breast cholesterol granuloma exhibiting persistent enhancement on dynamic-enhanced CT, which decreased in diameter 50 days after a core needle biopsy. Such entities are rare, and this report is the first to describe the dynamic-enhanced CT features of a cholesterol granuloma.
 XML Download
XML Download