

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The goal of this study was to investigate imaging results from a coronary CT angiography (CCTA) in chronic coronary total occlusion (CTO) before percutaneous coronary intervention (PCI).
Materials and Methods
In 74 patients with CTO, 34 patients was evaluated by using a 64-row multidetector CT scanner prior to the PCI and 40 control subjects with CTO, who only took PCI, were included. The multiplanar reformation of the heart chambers and three-dimensional CT images were used for determining an optimal view. We analyzed and evaluated the success rates of PCI, length of occluded vessel, calcified plaques, occluded side-branches, tapered occlusion, > 45° angulation of occluded artery, and myocardial density < 50 Hounsfield unit (HU).
Results
Success rates of PCI in the two groups, the control group and the experimental group, were not statistically different (p > 0.05). The mean length of occluded arteries was measured as 25 ± 11 mm and 26 cases (74%) had an occlusion length > 2 cm. Calcified plaques proximal to occlusion were detected in 19 cases (54%). Occluded side branches, tapered occlusion, > 45° angulation of occluded artery, and myocardial density < 50 HU were in 11 cases (32%), 9 cases (27%), 6 cases (18%), and 5 cases (15%), respectively.
Figures and Tables
Fig. 1
A 54-year-old male with chronic total occlusion in right coronary artery (RCA) and procedure by parallel wire technique.
A. A curved multiplanar reconstruction image of CT angiography shows occlusion of the proximal RCA (solid arrows) with concentric plaque (dashed arrows).
B. Volume rendering image shows easily occluded segment of RCA (solid arrow) and calcified plaque (dashed arrow).
C. Right coronary angiography shows two wires well. One wire (solid arrow) is placed in the dissection plane as guide marker and a second wire (dashed arrow) is a passing wire with the same path parallel to the first wire (solid arrow).

Fig. 2
A 43-year-old male with chronic total occlusion in left circumflex coronary artery (LCX) and recanalization by intravascular ultrasonogram (IVUS) guided wiring technique.
A, B. In a curved multiplanar reconstruction image of CT angiography (A) and volume rendering image (B), there are short occluded segment (solid arrows) and nodal branch of LCX, just proximal to occlusion (dashed arrows). In this situation such as blunt stump with side branch, failure of guide wire crossing is common. Therefore, IVUS use can be very helpful for completing the procedure.
C. Left coronary angiography shows main wire (solid arrow) and IVUS probe (dashed arrow), well. Asterisk indicates nodal branch of LCX.
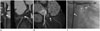
Fig. 3
A 78-year-old male with chronic total occlusion in the proximal left anterior coronary artery (LAD) and procedure by retrograde wire crossing technique. A curved multiplanar reconstruction image (A) and volume rendering image (B) show occlusion of the proximal LAD (solid arrows). LAD os has blunt stump and reverse tapered opacification is seen in the distal segment of occlusion (dashed arrow). Right coronary angiography showed collaterals from the right coronary artery (RCA) to the LAD via septal channels (not shown). The retrograde (solid arrow indicates the RCA os) guidewire through septal branch is located in the LAD, just distal to occluded segment (C). During drilling occluded segment, left coronary angiography shows short occluded LAD segment (solid arrow in D). Finally, the guidewire passed through the occluded segment (not shown).

Table 1
Baseline Clinical Characteristics

Note.-CTO without CT means CTO patient with only coronary angiography. CTO with CT means CTO patient with coronary angiography and CT scan.
CABG = coronary artery bypass graft, CTO = chronic total occlusion, LAD = left anterior coronary artery, LCX = left circumflex coronary artery, PCI = percutaneous coronary intervention, RCA = right coronary artery
Table 2
Lesion Characteristics on CTA and Procedural Characteristics (Recanalization)

References
1. Hoffmann U, Truong QA, Schoenfeld DA, Chou ET, Woodard PK, Nagurney JT, et al. Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med. 2012; 367:299–308.
2. Vliegenthart R, Henzler T, Moscariello A, Ruzsics B, Bastarrika G, Oudkerk M, et al. CT of coronary heart disease: Part 1, CT of myocardial infarction, ischemia, and viability. AJR Am J Roentgenol. 2012; 198:531–547.
3. Ko BS, Cameron JD, Leung M, Meredith IT, Leong DP, Antonis PR, et al. Combined CT coronary angiography and stress myocardial perfusion imaging for hemodynamically significant stenoses in patients with suspected coronary artery disease: a comparison with fractional flow reserve. JACC Cardiovasc Imaging. 2012; 5:1097–1111.
4. Ropers D, Pohle FK, Kuettner A, Pflederer T, Anders K, Daniel WG, et al. Diagnostic accuracy of noninvasive coronary angiography in patients after bypass surgery using 64-slice spiral computed tomography with 330-ms gantry rotation. Circulation. 2006; 114:2334–2341. quiz 2334.
5. Hou Y, Yue Y, Guo W, Feng G, Yu T, Li G, et al. Prospectively versus retrospectively ECG-gated 256-slice coronary CT angiography: image quality and radiation dose over expanded heart rates. Int J Cardiovasc Imaging. 2012; 28:153–162.
6. Xia Y, Junjie Y, Ying Z, Bai H, Qi W, Qinhua J, et al. Accuracy of 128-slice dual-source CT using high-pitch spiral mode for the assessment of coronary stents: first in vivo experience. Eur J Radiol. 2013; 82:617–622.
7. Westwood ME, Raatz HD, Misso K, Burgers L, Redekop K, Lhachimi SK, et al. Systematic review of the accuracy of dual-source cardiac CT for detection of arterial stenosis in difficult to image patient groups. Radiology. 2013; 267:387–395.
8. Mollet NR, Cademartiri F, van Mieghem CA, Runza G, McFadden EP, Baks T, et al. High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation. 2005; 112:2318–2323.
9. Pelliccia F, Pasceri V, Evangelista A, Pergolini A, Barillà F, Viceconte N, et al. Diagnostic accuracy of 320-row computed tomography as compared with invasive coronary angiography in unselected, consecutive patients with suspected coronary artery disease. Int J Cardiovasc Imaging. 2013; 29:443–452.
10. Dey D, Achenbach S, Schuhbaeck A, Pflederer T, Nakazato R, Slomka PJ, et al. Comparison of quantitative atherosclerotic plaque burden from coronary CT angiography in patients with first acute coronary syndrome and stable coronary artery disease. J Cardiovasc Comput Tomogr. 2014; 8:368–374.
11. Lehman SJ, Schlett CL, Bamberg F, Lee H, Donnelly P, Shturman L, et al. Assessment of coronary plaque progression in coronary computed tomography angiography using a semiquantitative score. JACC Cardiovasc Imaging. 2009; 2:1262–1270.
12. Maurovich-Horvat P, Ferencik M, Voros S, Merkely B, Hoffmann U. Comprehensive plaque assessment by coronary CT angiography. Nat Rev Cardiol. 2014; 11:390–402.
13. Hoffmann U, Moselewski F, Nieman K, Jang IK, Ferencik M, Rahman AM, et al. Noninvasive assessment of plaque morphology and composition in culprit and stable lesions in acute coronary syndrome and stable lesions in stable angina by multidetector computed tomography. J Am Coll Cardiol. 2006; 47:1655–1662.
14. Lev EI, Tayyan N, Raizner AE, Solomon SL, Simmons D, Kleiman NS. Initial impact of drug-eluting stent use on the spectrum of patients undergoing percutaneous coronary intervention. Coron Artery Dis. 2006; 17:379–384.
15. Saia F, Piovaccari G, Manari A, Santarelli A, Benassi A, Aurier E, et al. Clinical outcomes for sirolimus-eluting stents and polymer-coated paclitaxel-eluting stents in daily practice: results from a large multicenter registry. J Am Coll Cardiol. 2006; 48:1312–1318.
16. Galassi AR, Tomasello SD, Reifart N, Werner GS, Sianos G, Bonnier H, et al. In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion: insights from the ERCTO (European Registry of Chronic Total Occlusion) registry. EuroIntervention. 2011; 7:472–479.
17. Barlis P, Kaplan S, Dimopoulos K, Tanigawa J, Schultz C, Di Mario C. An indeterminate occlusion duration predicts procedural failure in the recanalization of coronary chronic total occlusions. Catheter Cardiovasc Interv. 2008; 71:621–628.
18. Dong S, Smorgick Y, Nahir M, Lotan C, Mosseri M, Nassar H, et al. Predictors for successful angioplasty of chronic totally occluded coronary arteries. J Interv Cardiol. 2005; 18:1–7.
19. Takimura H, Muramatsu T, Tsukahara R. CT coronary angiography-guided percutaneous coronary intervention for chronic total occlusion combined with retrograde approach. J Invasive Cardiol. 2012; 24:E5–E9.
20. Poulter RS, Nicolaou S, Hoole SP, Seddon MD, Buller CE, Mayo J, et al. Comprehensive assessment of a chronic total occlusion by dual-energy cardiac CT angiography with adenosine stress prior to retrograde percutaneous recanalization. J Cardiovasc Med (Hagerstown). 2011; 12:513–515.
21. Ueno K, Kawamura A, Onizuka T, Kawakami T, Nagatomo Y, Hayashida K, et al. Effect of preoperative evaluation by multidetector computed tomography in percutaneous coronary interventions of chronic total occlusions. Int J Cardiol. 2012; 156:76–79.
22. García-García HM, van Mieghem CA, Gonzalo N, Meijboom WB, Weustink AC, Onuma Y, et al. Computed tomography in total coronary occlusions (CTTO registry): radiation exposure and predictors of successful percutaneous intervention. EuroIntervention. 2009; 4:607–616.
23. Smith SC Jr, Dove JT, Jacobs AK, Kennedy JW, Kereiakes D, Kern MJ, et al. ACC/AHA guidelines for percutaneous coronary intervention (revision of the 1993 PTCA guidelines)-executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee to revise the 1993 guidelines for percutaneous transluminal coronary angioplasty) endorsed by the Society for Cardiac Angiography and Interventions. Circulation. 2001; 103:3019–3041.
24. Christofferson RD, Lehmann KG, Martin GV, Every N, Caldwell JH, Kapadia SR. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol. 2005; 95:1088–1091.
25. Silber S, Albertsson P, Avilés FF, Camici PG, Colombo A, Hamm C, et al. Guidelines for percutaneous coronary interventions. The Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology. Eur Heart J. 2005; 26:804–847.
26. Sirnes PA, Myreng Y, Mølstad P, Bonarjee V, Golf S. Improvement in left ventricular ejection fraction and wall motion after successful recanalization of chronic coronary occlusions. Eur Heart J. 1998; 19:273–281.
27. Moreno R, Conde C, Perez-Vizcayno MJ, Villarreal S, Hernandez-Antolin R, Alfonso F, et al. Prognostic impact of a chronic occlusion in a noninfarct vessel in patients with acute myocardial infarction and multivessel disease undergoing primary percutaneous coronary intervention. J Invasive Cardiol. 2006; 18:16–19.
28. Kinoshita I, Katoh O, Nariyama J, Otsuji S, Tateyama H, Kobayashi T, et al. Coronary angioplasty of chronic total occlusions with bridging collateral vessels: immediate and follow-up outcome from a large single-center experience. J Am Coll Cardiol. 1995; 26:409–415.
29. Schmid M, Achenbach S, Ludwig J, Baum U, Anders K, Pohle K, et al. Visualization of coronary artery anomalies by contrast-enhanced multi-detector row spiral computed tomography. Int J Cardiol. 2006; 111:430–435.
30. Li M, Zhang J, Pan J, Lu Z. Obstructive coronary artery disease: reverse attenuation gradient sign at CT indicates distal retrograde flow--a useful sign for differentiating chronic total occlusion from subtotal occlusion. Radiology. 2013; 266:766–772.
31. Di Mario C, Werner GS, Sianos G, Galassi AR, Büttner J, Dudek D, et al. European perspective in the recanalisation of Chronic Total Occlusions (CTO): consensus document from the EuroCTO Club. EuroIntervention. 2007; 3:30–43.
32. Gomes MN, Davros WJ, Zeman RK. Preoperative assessment of abdominal aortic aneurysm: the value of helical and three-dimensional computed tomography. J Vasc Surg. 1994; 20:367–375. discussion 375-376.
33. Wolf YG, Tillich M, Lee WA, Rubin GD, Fogarty TJ, Zarins CK. Impact of aortoiliac tortuosity on endovascular repair of abdominal aortic aneurysms: evaluation of 3D computer-based assessment. J Vasc Surg. 2001; 34:594–599.
34. Fukuhara R, Ishiguchi T, Ikeda M, Ota T, Takai K, Satake H, et al. Evaluation of abdominal aortic aneurysm for endovascular stent-grafting with volume-rendered CT images of vessel lumen and thrombus. Radiat Med. 2004; 22:332–341.
35. Mollet NR, Hoye A, Lemos PA, Cademartiri F, Sianos G, McFadden EP, et al. Value of preprocedure multislice computed tomographic coronary angiography to predict the outcome of percutaneous recanalization of chronic total occlusions. Am J Cardiol. 2005; 95:240–243.
36. Yokoyama N, Yamamoto Y, Suzuki S, Suzuki M, Konno K, Kozuma K, et al. Impact of 16-slice computed tomography in percutaneous coronary intervention of chronic total occlusions. Catheter Cardiovasc Interv. 2006; 68:1–7.
37. Kaneda H, Saito S, Shiono T, Miyashita Y, Takahashi S, Domae H. Sixty-four-slice computed tomography-facilitated percutaneous coronary intervention for chronic total occlusion. Int J Cardiol. 2007; 115:130–132.
38. Smits PC, Pasterkamp G, de Jaegere PP, de Feyter PJ, Borst C. Angioscopic complex lesions are predominantly compensatory enlarged: an angioscopy and intracoronary ultrasound study. Cardiovasc Res. 1999; 41:458–464.
39. Sianos G, Werner GS, Galassi AR, Papafaklis MI, Escaned J, Hildick-Smith D, et al. Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention. 2012; 8:139–145.
40. Hausleiter J, Meyer T, Hadamitzky M, Huber E, Zankl M, Martinoff S, et al. Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation. 2006; 113:1305–1310.
41. Hendel RC, Patel MR, Kramer CM, Poon M, Hendel RC, Carr JC, et al. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006; 48:1475–1497.
 XML Download
XML Download