

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A meconium pseudocyst consists of a thinning intestinal wall. The pseudocyst wall has a muscle layer continuous with the intestine but because of inflammation it has no epithelium (1).
In contrast, the cystic-type meconium peritonitis results from the meconium peritonitis. Meconium peritonitis is defined as a sterile chemical or foreign-body peritonitis that is caused by the escape of meconium from the intestinal tract into the general peritoneal cavity during the fetal or perinatal period and the small bowel is nearly always involved. In the first day the meconium is surrounded by giant cells and histocytes resulting in foreign body granulomas and subsequently in calcification (2).
Meconium peritonitis creates a cystic cavity with a fibrous wall when the inflamed intestinal loops become fixed and the result is named as cystic-type meconium peritonitis. Because of their different treatment strategies the meconium pseudocyst and the cystic-type meconium peritonitis should be distinguished. An one-stage intestinal resection with a primary anastomosis is recommended for the meconium pseudocyst. However, a cystic-type meconium peritonitis is usually treated using a drainage with subsequent elective surgery (3).
In various studies have been reported the radiologic findings of meconium peritonitis with cystic lesions. However, there are limitations to distinguish a meconium pseudocyst from a cystic-type meconium peritonitis.
For this report the literature was reviewed and the characteristic CT findings of neonates with meconium pseudocysts were discussed.
CASE REPORT
On fetal ultrasonography at week 29 week of gestation was observed a hypoechoic abdominal cyst which predominantly occupied the right abdomen. In the follow-up fetal sonography a progressive abdominal distension, polyhydraminios and an increased cyst size was shown. As a result, a newborn boy, weighing 2490 g, was delivered by cesarean at 33 weeks of gestation.
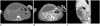
A simple radiograph of the abdomen revealed a large egg-shell calcification in the mid abdomen (Fig. 1). An abdominal ultrasonography demonstrated a huge complicated cystic mass filled with heterogeneous echogenic material and encapsulated by dense calcification and without vascularity along the wall (Fig. 2). A CT scan showed a large hypodense cyst with calcified rim and fluid content and a measurable maximal diameter about 5 cm. On sagittal image of CT scan was found a communication between the cyst and the adjacent dilated bowel (Fig. 3B, C), suggesting a meconium pseudocyst. The scan revealed diffuse calcium deposition on the parietal peritoneum and other adjacent intra-abdominal structure also (Fig. 3A).
A resection of the cyst and the ischemic small intestine was performed followed by primary end-to-end anastomosis. The histopathological findings revealed the cyst wall contained a smooth muscle layer in continuation with the normal intestine. The final diagnosis set as meconium pseudocyst with an ongoing ileal perforation. The baby recovered well post-operative.
DISCUSSION
Shyu et al. (4) reported fetal ultrasonographic findings of meconium peritonitis, including calcification, fetal ascites, hydramnios, pseudocysts and a dilated bowel. Polyhydramnios was associated with 25-50% of cases with meconium peritonitis. In the present case, the cyst in the upper mid-abdomen was detected at 29 weeks gestation before a polyhydroamnios was developed. The prenatal sonography showed a progressive abdominal distension and polyhydroamnios at a 2 weeks follow-up.
The radiographic findings of the meconium pseudocyst included an intra-abdominal mass with rim calcification (5). The abdominal ultrasound showed a meconium pseudocyst as a well-defined hypoechoic mass surrounded by an echogenic calcified wall, indicating a contained perforation (6). On CT an intra-abdominal cyst encapsulated by wall calcification, with and without air and fluid contents are seen. The cyst is connected to the proximal intestine (1). Also diffuse calcium deposits could be seen along the parietal peritoneum and other intra-abdominal structures, including the scrotal and thoracic cavities (7).
A meconium pseudocyst consists of a thinning intestinal wall, a muscle layer continuous with the normal intestine without epithelium. Thus it is referred as a pseudocyst. The cause of a meconium pseudocyst is uncertain. However, there is an presumption about an association with dilated intestine caused by intestinal atresia and impaired intestinal blood flow because of an inflammation after intestinal perforation. If the atresia and the impaired blood flow occur before the meconium reaches the small intestine, the site will develop an intestinal atresia without meconium peritonitis. However, a pseudocyst may be formed if they occur after the meconium reaches the site. Fibroadhesive-type meconium peritonitis may be an outcome if the perforation site is sealed and another outcome may be an intestinal dilatation because of an inflammation or an impaired intestinal blood flow. As a result a meconium pseudocyst can be believed. A meconium pseudocyst may be a complication of a meconium peritonitis and therefore it likely to be misdiagnosed as a cystic-type meconium peritonitis (1).
To prevent a bacterial infection and to decompress the distended intestine a baby with a cystic-type meconium peritonitis will need an immediate operation after birth. However, to initially treat these patients with a cyst drainage and an enterostomy is possible because the cyst wall may be too frail to resect. When the patient stabilizes, a second operation is necessary to anastomose the intestine when the patient stabilizes (8). However, in patients with a meconium pseudocyst, the wall is firm enough to resect because it has a muscle layer. So an one-stage resection and a primary anastomosis can be performed (1).
Meconium pseudocysts and cystic-type meconium peritonitis present with similar clinical and radiologic findings and there may be a confusion tendency. Thus, more efforts by the neonatologist, obstetrician, pediatric surgeon and radiologist are required to distinguish the diagnosis of meconium pseudocyst from the cystic-type meconium peritonitis.
The increased potential risk of radiation induced-cancer is an important concern in the treatment of children who are more sensitive to radiation and are more sensible to radiation and have a longer life span also (9). Therefore a CT is usually not recommended. Thus, CT findings of a meconium pseudocyst are rarely reported. But the CT findings may be helpful if there are confusions due to the sonography and simple radiograph findings. In the presented case, an additional CT showed a finely distributed calcification and the cyst connecting with the proximal intestine on a sagittal image. So, a meconium pseudocyst could be properly diagnosed and another cystic mass such as a distended bladder or mesenteric and ovarian cyst could be easy differentially diagnosed additionally.
Meconium pseudocysts should be distinguished from the cystic-type meconium peritonitis because of differences in the treatment strategy and their pathologic features (1). An early diagnosis and a proper disease management are essential for a better prognosis.
In conclusion, the CT study was useful as a complementary imaging modality in the evaluation, the proper diagnosis of a meconium pseudocyst and for the differential diagnosis to distinct from a cystic-type meconium peritonitis also.


 XML Download
XML Download