

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The incidence of multiple pregnancies has increased over the decades with the increased use of assisted reproductive techniques (ART).12 These women who conceive a multiple pregnancy with ART are usually of more advanced maternal age. With increased age-related chromosomal abnormalities and the risk of aneuploidy per gestation in dizygotic twins, an increasing need is seen for prenatal diagnosis in multiple pregnancies.1345
Under certain circumstances, women with twin pregnancies (TPs) may be advised to undergo invasive prenatal diagnostic testing. Chorionic villus sampling (CVS) and amniocentesis (AC) are the two commonly performed invasive prenatal diagnostic testing.36 Indications for CVS and AC are chromosomal evaluation for advanced maternal age, pregnancies established after intracytoplasmic sperm injection, and chromosomal evaluation or DNA analysis for other indications, including history of monogenetic disease, presence of sonographic markers for fetal aneuploidy or fetal structural defects, chromosomal malformations in parents or previous pregnancies, and the psychological indications.7 However, a possible increased risk of fetal loss after AC or CVS might require a careful evaluation of such a recommendation. In previous studies, the rate of fetal loss related with CVS was believed to be between 1.7% and 11.5% and with AC, between 2.7% and 9.4%.68910111213 While studies have investigated the fetal loss rates associated with each procedure individually, studies comparing both CVS and AC in TP are limited.4514
The primary and secondary aims of the present study were to compare the obstetrical outcomes that followed CVS or AC in TP and to compare the groups with respect to the procedure-related fetal loss, respectively.
METHODS
Between December 2006 and January 2017, 287 CVS and AC procedures were performed on TPs at the Department of Obstetrics and Gynecology, CHA Bundang Medical Center, CHA University, Seongnam, Korea. The exclusion criteria were a twin with known chromosome anomaly or lethal anatomical defects, demise of one twin at the time of the procedure, monochorionic or monoamniotic twin, repeated invasive procedure, and pregnancies in which selective feticide was carried out. After exclusion, a total of 224 dichorionic–diamniotic twin pregnancies were included in the study. CVS and AC were performed in 54 (group 1) and 170 patients (group 2), respectively. Two experienced operators carried out all procedures. A detailed ultrasound evaluation was done in the initial step prior to each procedure including fetal biometry, the position of the fetuses, and the location of each placenta. Chorionicity was determined during the first-trimester scan when the women presented at the appropriate gestation.
CVS was performed transabdominally using ultrasound guidance, after sonographic mapping of placental implantations and cord insertions. Under ultrasound visualization, a double-needle system (outer needle, 18 gauze; inner needle, 20 gauze) was inserted into the placenta. The guided needle was first introduced into the placenta to be sampled. Thereafter, an aspiration needle was passed through the guide needle and villi obtained by aspiration. The placenta of the second twin was sampled by another needle puncture. Samples of > 10 and 20 mg per fetus were considered appropriate for karyotyping and biochemical or DNA analysis, respectively. For AC, under ultrasound visualization, a 22-gauze spinal needle was inserted into each amniotic cavity under continuous transabdominal ultrasound visualization. The first spinal needle was inserted into one sac, and 20 mL of amniotic fluid was aspirated after 2 mL of amniotic fluid was discarded for maternal contamination prevention. The spinal needle was then removed, and the same procedure was then repeated for the second twin using a second needle, separately entered at a different location. A fluid sample was obtained in the same amount. Fetal heart rate variability was always demonstrated after the procedure. Follow-up ultrasound scans were arranged at 1–4-week intervals. Full karyotype reports were available within 3 weeks.
The baseline characteristics were analyzed, including the conception mode, mean nuchal translucency (NT), incidence of first-trimester vaginal bleeding, and the gestational age at the time of procedure. The conception modes were defined as spontaneous or achieved through ART. Indications for AC and CVS were chromosomal evaluation for advanced maternal age (≥ 35 years abnormal maternal serum screening test results, increased NT or abnormal sonographic findings, chromosomal malformations in parents or previous pregnancies, and miscellaneous such as psychological indications and pregnancies established after intracytoplasmic sperm injection. Multiple indications were allowed. The main indications for CVS were increased NT or abnormal ultrasound scan finding in the first trimester, whereas those for AC were abnormal maternal serum screening test results.
The procedure-related fetal loss, which was defined as the loss of one or two fetuses within 4 weeks of the procedure, was assessed in this study. The obstetrical outcomes assessed included the miscarriage rate, which was defined as a delivery at < 24 weeks' gestation; early and late preterm deliveries, defined as a delivery at ≥ 24 weeks and < 34, ≥ 34, and < 37 weeks; term delivery; maternal complications; and overall fetal loss, which was defined as the loss of one or two fetuses during the gestation. The mean birth weight and the need for neonatal intensive care unit (NICU) admission were also recorded.
The statistical analyses were performed using IBM® SPSS® software, version 24 (IBM Corporation, Armonk, NY, USA). The statistical significance of the differences between the amniocentesis and CVS groups was analyzed using the χ2 test, Fisher's exact test, the Mann–Whitney U-test, and a two-tailed unpaired Student's t-test, as appropriate. Logistic regression analysis was used for the multivariate analysis while controlling for the effects of the potential confounders, which included maternal age, body mass index, parity, mode of conception, mean measure of fetal NT, and indications for the procedure. A value of P < 0.05 was considered significant.
Ethics statement
The data were collected retrospectively at the Department of Obstetrics and Gynecology following Institutional Review Board (IRB) approval (IRB No. 2017-04-038) on March 19, 2018, CHA Bundang Medical Center, CHA University. Informed consent was waived by institutional review board due to the retrospective nature of this study.
RESULTS
This study was comprised of 54 and 170 patients who underwent CVS (group 1) and AC (group 2), respectively. Table 1 presents the study participants' characteristics. The mean gestational ages at which the procedures were undertaken were 12 ± 0.05 and 17.9 ± 1.7 weeks for groups 1 and 2, respectively (P < 0.001). Significant differences were evident between groups 1 and 2 regarding the mean measure of NT of the fetuses (group 1, 2.1 ± 0.9 mm; group 2, 1.3 ± 0.5 mm; P < 0.05). No significant difference was observed in incidence of first-trimester vaginal bleeding between the groups.
Table 1
Baseline characteristics
Group 1 had higher numbers of indications of abnormal ultrasound scan including increased NT, poor obstetrical history, and chromosomal aberration in family, and group 2 had higher numbers of indications of advanced maternal age (35 years) and abnormal maternal serum screening test results (Table 2). After the procedure, 15 cases with heteromorphic variants were detected (2 cases in CVS and 13 cases in AC) such as acrocentric chromosomal satellites (ps+), and non-acrocentric chromosomes with qh+, and inversion chromosome 9. We performed parent chromosome analysis if we needed to confirm whether the variants were inherited or de novo. There were 13 cases of non-lethal anatomical defects (2 cases in CVS and 11 cases in AC) such as small ventricular septal defect, unilateral pyelectasis, polydactyl, abdominal cyst of the fetus, and cleft lip.
Table 2
Indications for invasive procedure
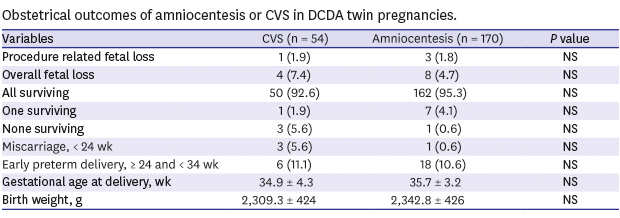
No immediate procedure-related complications occurred. The procedure-related fetal loss tended to be similar between the two groups. After adjusting for the potential confounders described previously, the frequency of procedure-related fetal loss within the 4 weeks was 1.9% in group 1 compared with 1.8% in group 2 (P = NS, not significant) (Table 3). The overall fetal loss rate between group 1 (7.4%) and group 2 (4.7%) had no statistical significance (P = 0.489). There were a total of 12 cases of overall fetal loss. Of these, 4 were procedure-related and 8 occurred from non-procedure-related causes, which included 3 cases which occurred due to preterm labor or preterm premature rupture of the membrane (all delivered before 24 weeks) and 5 cases where one fetus was lost due to discordant twin (intrauterine demise of one fetus at 26 through 33 weeks). The miscarriage rate was higher in group 1 than in group 2. However, this finding was not statistically significant after adjusting for the potential confounders. The groups did not differ with respect to maternal complications, except incompetent internal os of the cervix (IIOC) rate was higher in group 1 (24.1%) than in group 2 (12.9%) (OR, 2.2; 95% CI, 1.0–4.8; P = 0.047). No significant difference was observed with respect to preterm delivery rate, mean gestational age, birth weights, and NICU admission rate between the groups.
Table 3
Procedure-related and obstetrical outcomes between AC and CVS

Data are represented as mean ± standard deviation or number (%).
AC = amniocentesis, CVS = chorionic villus sampling, CI = confidence interval, PPROM = preterm premature rupture of membranes, IIOC = incompetent internal os of the cervix, NICU = neonatal intensive care unit, NS = not significant.
aProcedure-related fetal loss, defined as the loss of one or two fetuses within 4 weeks of the procedure; boverall fetal loss, defined as one or two fetal losses throughout the pregnancy.
DISCUSSION
In this study, the overall fetal loss and procedure-related fetal loss of CVS appear comparable to those of AC. Other obstetrical outcomes tended to be similar between the two groups. The CVS group in our study had a higher rate of IIOC; this might be explained due to the fact that our institution is a university hospital. Compared to amniocentesis, CVS is a more difficult procedure. Moreover, most of the CVS cases were transferred to our institution from local clinics for the procedure, and patients were transferred back to the local clinics after CVS if there was no preterm labor or IIOC. However, patients with preterm labor or IIOC tended to stay and deliver in our institution. In contrast, most of the amniocentesis cases were those that were followed up at our institution from the first trimester; thus, they may have had lower risk pregnancies compared to the CVS group.
Increasing frequencies of multiple pregnancies and advanced maternal age have expanded the need for invasive prenatal diagnosis.123415 Fetal loss after invasive prenatal diagnostic tests is one of the major concerns of pregnant women. Counseling before any of these procedures is mandatory and must include information about the probable risks and benefits of the procedure. The risks of pregnancy loss after CVS and AC in singleton pregnancies are well described.161718192021 A systematic review and meta-analysis by Akolekar in singleton pregnancies revealed miscarriage rates before 24 weeks' gestation of 1.79% and 0.67% for CVS and AC, respectively, and the estimate of a loss attributable to the invasive procedure is 0.1% for AC and 0.2% for CVS in singleton.16 The reported adverse outcomes of invasive testing in twin pregnancies were higher than in singleton pregnancies. In a recent systematic review and meta-analysis, total pregnancy loss rates for CVS and AC were 3.84% and 3.07% in TP, respectively.8
Several studies have been conducted that report on outcomes of each AC and CVS in TPs. The pregnancy loss rate in twin CVS, which ranges from 1.7% to 11.5%, has been reported in various studies.622 De Catte et al.23 reported that the total spontaneous fetal loss rate until birth was 5.5% in 262 TPs. Selective feticide (SF) of one fetus was done in 11 TPs, and it was concluded that CVS is an accurate means of prenatal genetic diagnosis in twins, offering early selective feticide in cases of abnormal genetic results in one of the fetuses. In twin AC, Cahill et al.12 performed a retrospective study comparing 311 dichorionic and monochorionic TPs who elected AC to the rest of the cohort who did not. Those who had an AC performed were more likely to experience a pregnancy loss than those who did not (3.2% vs. 1.4%), indicating an attributable risk of pregnancy loss before 24 weeks of gestation of 1.8%. Similarly, Yukobowich et al.10 performed a large retrospective cohort study to examine pregnancy outcomes after AC in 476 women in TP with singletons and untested twins and concluded that risk of early fetal loss in twin AC cohort appears to be higher than the rest (2.73% vs. 0.60% vs. 0.63%). In contrast, a prospective study by Lenis-Cordoba et al.9 and a retrospective cohort study by Millaire et al.11 revealed no significant increase in the rate of fetal loss in women with TP who underwent AC compared to untested twin.
So far, several literatures are available reporting on clinical outcomes of each AC and CVS in TP. However, to date, there are only four studies that have compared both CVS and AC in TP. The first study by Wapner et al.14 demonstrated that CVS is at least as safe as AC with total fetal loss rates of 4.9% and 9.3% in CVS and AC, respectively. However, the study included cases with repeated invasive procedure and fetus with known chromosome anomaly. Chromosomal anomalies such as trisomy 21 and 18 are associated with increased risks of miscarriage, fetal growth restriction, preterm delivery, and fetal demise in multiple pregnancies.2425 A study by Antsaklis et al.5 revealed total fetal loss rates of 10.2% and 8.8% in CVS and AC, respectively, in dichorionic and monochorionic TP, which included fetuses with structural anomalies. Several studies have reported that the presence of major anatomical malformation of one fetus in TP has been reported to increase the risk of preterm birth.2627 Simonazzi et al.4 reported a miscarriage (< 24 weeks) rate of 3.85% in CVS and 4.0% in AC in dichorionic and monochorionic TP. A large study by Hack et al.28 showed that monochorionic pregnancies have higher adverse pregnancy outcomes than dichorionic pregnancies at all gestations. Three studies above were too heterogeneous for accurate result. After excluding cases that may influence the fetal loss rate, our study revealed the total fetal loss rates of CVS and AC were 7.4% and 4.7%, respectively. Similar exclusion criteria were used in the study of Enzensberger et al.7 The total fetal loss rates in their study were 13.6% and 6.1% for CVS and AC, respectively. The discrepancy among the total fetal loss rates between our study and the study of Enzensberger et al.7 may be due to the fact that the procedures were performed in the same manner by a small, selected group of trained experts.
To the best of our knowledge, only two studies that compared procedure-related fetal loss between twin CVS and AC have been conducted till date. Simonazzi et al.4 reported a fetal loss rate (within 4 weeks) of 3.85% in CVS and 4% in AC. Enzensberger et al.7 reported a fetal loss rate (within 2 weeks) of 6.8% after CVS and 2.3% after AC. Compared to that in these studies, the procedure-related loss rate for both procedures was lower in our series (1.9% and 1.8% for CVS and AC, respectively) (P value = NS). Although the comparison of procedure-related fetal loss rates is difficult because of varying definitions of time intervals, all the literature reviews reported no statistical difference in the procedure-related fetal loss between CVS and AC despite the variation.4720 We defined procedure-related fetal loss as 4 weeks because most published reported articles did the same, and in our study patients were followed up 1 week after the procedure and subsequently 3 weeks later. No significant difference was observed in procedure-related fetal loss in the two groups; thus, extremely old pregnant women with TP may undergo first-trimester CVS, not waiting for AC in the second trimester only for safety.
Prenatal counseling for patients with TP is more complicated than for singleton pregnancies. Some anomalous fetus in TP significantly increased the risk of preterm delivery, frequency of cesarean section, and perinatal mortality rates compared with normal TP.262729 The choice of the invasive procedure (CVS or AC) depends on the level of risk, the likelihood to proceed to SF, the gestation at presentation, and the technical difficulties of the specific patient.5 In this study, the majority of CVS procedures were performed in women with increased NT or abnormal sonographic findings and previous chromosomal malformation or chromosomal aberration in the family. The advantage of CVS in TP is early diagnosis, allowing earlier SF, if indicated.561423 In our study, SF was performed in 15 cases following AC and CVS because of abnormal karyotype (6), major malformation by ultrasound (8), and others (1). Similar to the findings of other studies, CVS appears to be a safe alternative to AC and should be considered as the method of choice particularly when there is a high risk of an affected fetus necessitating SF.5
We acknowledge that the lack of a control group of sampled twins and some fetal losses that occurred after > 4 weeks that could have been procedure-related loss are potential limitations of this study. This study's strengths are associated with it being a single-center study with only two experienced operators performing the procedure. The population enrolled in this study is quite homogeneous compared to that in previous studies, and to date, this is one of the few studies to evaluate procedure-related fetal loss.
In conclusion, the choice of which invasive procedure to perform in TP is based on several factors: indications, gestational age, technical difficulties, the likelihood to proceed to SF, and operators' experience. The procedure-related fetal loss and the overall fetal loss of CVS appear comparable to those of AC. These findings can be used by clinicians when counseling parents of twins regarding their options for antenatal aneuploidy and genetic diagnosis and the associated risks. Furthermore, randomized controlled trials are necessary to compare the safety of CVS and AC in TP.
 XML Download
XML Download