

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Distal renal tubular acidosis (dRTA), also referred to as type 1 RTA, is clinically characterized by persistent hyperchloremic metabolic acidosis with normal serum anion gap, hypokalemia, hypercalciuria, and nephrocalcinosis. This disease is caused by inability of the α-intercalated cells in the collecting duct to secrete H+ and properly acidify urine.12 Primary dRTA is a rare genetic disorder with genetic heterogeneity. To date, at least three genes are known to cause dRTA, including ATP6V1B1, ATP6V0A4, and SLC4A1.23
ATP6V1B1 and ATP6V0A4 encode for B1 and A4 subunits of the apical H+-ATPase pump, respectively, and mutations in these genes cause autosomal recessive (AR) forms of dRTA with or without sensorineural hearing loss.45 Mutations in SLC4A1 (solute carrier family 4 member 1), encoding the basolateral anion (Cl−/HCO3−) exchanger 1 (AE1), can cause both dominant and recessive form of dRTA.1 AE1 is expressed not only in the α-intercalated cells, but also in the erythrocytes (erythrocyte membrane protein band 3). Therefore, SLC4A1 mutations can cause dRTA and/or hemolytic anemia with abnormal red cell morphology.67
SLC4A1 mutations were initially reported to be always associated with autosomal dominant (AD) form of dRTA.6 AR dRTA caused by SLC4A1 mutations have been reported mostly from tropical Southeast Asia and other tropical areas, therefore called as tropical recessive dRTA.789101112131415 Here, we report three Lao patients from two unrelated families with AR dRTA in association with the same homozygous SLC4A1 mutation, p.Gly701Asp.
CASE DESCRIPTION
Case 1
In Sepember 2009, a 4-year-old girl was referred to the Children's Hospital, Vientiane, Laos from Luang Prabang because of short stature and failure to thrive. Her height (80 cm) and weight (7.8 kg) was less than 3 percentiles for her age. Laboratory tests revealed low serum bicarbonate level with hypokalemia (serum HCO3− 13 mmol/L and K+ 2.9 mmol/L). Serum Na+ and Cl− levels were unavailable. Urine pH was measured as 9.0 by dipstick. She did not have anemia and episodes of diarrhea. Under a tentative diagnosis of dRTA, she began to take baking soda, which was the only available oral alkali supplement in Laos at the time.
At the age of 7.8 years, despite steady intake of baking soda, she was still short (96 cm) and underweighted (13.6 kg) for her age. Laboratory tests revealed that serum HCO3− level was 20 mmol/L; K+, 3.0 mmol/L; and Cl−, 113 mmol/L. Renal ultrasonogram showed medullary nephrocalcinosis in both kidneys. Bone X-rays revealed diffuse osteopenia in both forearms. Her hearing ability was normal. At that time, oral potassium citrate became available and was added to baking soda. Her laboratory abnormalities improved (serum HCO3−, 21 mmol/L; K+, 4.0 mmol/L; and Cl−, 106 mmol/L) within 3 months of taking oral potassium citrate supplement, and her appetite and physical activities improved remarkably as well. At the age of 9.7 years, her height and weight was 113 cm and 20 kg, respectively. She was still short for her age, but showed a significant catch-up growth.
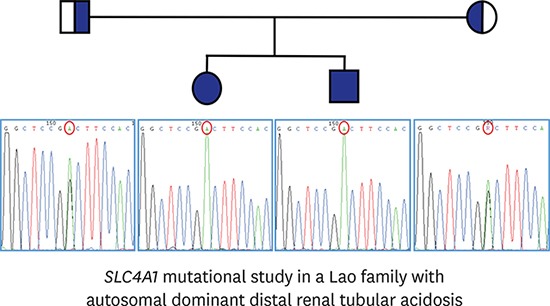
Her younger brother was also short and underweighted. In 2016, mutational analyses revealed a homozygous c.2102G>A (p.Gly701Asp) mutation in exon 17 of SLC4A1 in both siblings. In addition, both siblings harbored a homozygous c.166A>C (p.Lys56Glu) and a heterozygous c.92T>C (p.Met31Thr) variation. Their mother was heterozygous for all three variations, while their father was heterozygous for c.2102G>A and c.166A>C but not c.92T>C (Fig. 1A).
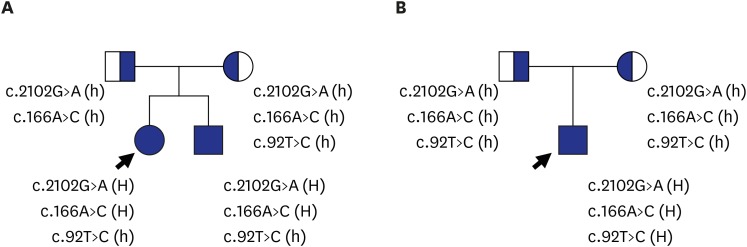
Fig. 1
Pedigrees of two Lao families with autosomal recessive dRTA. (A) Case 1 and her affected sibling have a homozygous SLC4A1 mutation, c.2102G>A (p.Gly701Asp), which is inherited from heterozygous parents. (B) Case 2 has the same homozygous SLC4A1 mutation, and both parents are heterozygous for the mutation.
dRTA = distal renal tubular acidosis, H = homozygous, h = heterozygous.
Case 2
In November 2013, a 3-year-old boy was referred to the Children's Hospital, Vientiane, Laos from Xienquang Province. His height (88 cm) and weight (9.3 kg) was less than 3 percentiles for his age. Such growth retardation had been regarded as malnutrition, one of the common childhood problems in the Province. The laboratory tests revealed that serum Na+ level was 144 mmol/L; HCO3−, 18.1 mmol/L; K+, 2.0 mmol/L; and Cl−, 117 mmol/L. Anion gap was normal (9 mmol/L). The hemoglobin level was 6.2 g/dL, but peripheral blood smear was not performed. Renal ultrasonogram revealed medullary nephrocalcinosis in both kidneys, and skeletal X-ray showed rachitic changes with diffuse osteopenia in both distal radius and ulna. He did not have hearing impairment. He began to be treated with sodium bicarbonate and Urocitra® under clinical diagnosis of dRTA. The laboratory abnormalities were improved (serum K+, 5.0 mmol/L; HCO3−, 24 mmol/L; and Cl−, 108 mmol/L) rapidly within 5 days of treatment. After 6 months, he was able to run and ride a bike. He grew 8 cm in a year, and at the age of 4.8 years, his height was 96 cm and weight was 15 kg (5–10th percentiles and 5th percentiles for his age, respectively).
In 2016, mutational analyses revealed the patient was triply homozygous for the loss-of-function mutation, c.2102G>A (p.Gly701Asp) as well as for two benign variations, c.92T>C (p.Met31Thr) and c.166A>C (p.Lys56Glu), in SLC4A1. Both parents were heterozygous for all these three variations (Fig. 1B).
DISCUSSION
Recently, it has become evident that primary dRTA, in association with SLC4A1 mutations, shows considerable difference in pattern of inheritance and clinical manifestation in different parts of the world.15 In temperate countries, primary dRTA caused by SLC4A1 mutations manifests as an AD disease without any red cell morphological abnormalities. In contrast, in the tropics, it is almost invariably recessive and often accompanies red cell morphological abnormalities or hemolytic anemia.15 AR dRTA caused by SLC4A1 mutations, so called tropical dRTA, has a high prevalence in Southeast Asia, particularly Thailand, Malaysia, the Philippines, and Papua New Guinea.89101112 However, there has been no case report from some neighboring countries, including Laos, Myanmar, Vietnam, Cambodia, and Indonesia. This case report is the first one from Laos.
There are four common SLC4A1 mutations causing AR dRTA: 1) Δ400–408, a 27 base-pair deletion resulting in deletion of the nine AE1 amino acid residues 400–408, which is known to also cause Southeast Asian ovalocytosis (SAO), 2) p.Gly701Asp, 3) p.Ala858Asp, and 4) ΔVal850, a deletion of the 850th valine residue.15
The SAO mutation in dRTA patients was always heterozygous and accompanied by another mutation on the opposite allele, usually one of three other common mutations.15 In other words, the inheritance of SAO is dominant and that of dRTA is recessive in these patients.
The p.Gly701Asp mutation, the same mutation detected in our cases, is the most common SLC4A1 mutation causing AR dRTA.15 This mutation is highly prevalent in Northeast Thailand, with a prevalence of 0.73%.16 Accordingly, the p.Gly701Asp mutation causing AR dRTA in Northeast Thailand has usually been homozygous,78 but in other parts of the tropics, including southern Thailand and Malaysia, it is usually detected as one of the compound heterozygous mutations.101217 Of interest, the p.Gly701Asp mutation is known to be invariably inherited with two nonpathogenic SLC4A1 polymorphisms: p.Met31Thr and p.Lys56Glu.7101112 This complex triad of mutations (p.Gly701Asp/p.Met31Thr/p.Lys56Glu) found in patients with AR dRTA from Northeast Thailand suggests a founder effect.15 However, in a recently reported case of Scandinavian ancestry with AR dRTA caused by compound heterozygosity of p.Cys479Trp/p.Gly701Asp, the p.Gly701Asp mutation was not accompanied by the p.Lys56Glu polymorphism (the report did not mention p.Met31Thr).18 These findings suggested that the mutation in the patient may have evolved independently of the mutation of Northeast Thailand origin. In our study, case 2 had the homozygous complex triad of mutations, as found in Northeast Thailand patients. However, in case 1 and her younger brother, the maternal allele had all the three variations, while the paternal allele had only 2 of the variations p.Gly701Asp and p.Lys56Glu, but not p.Met31Thr. These findings suggest that, although Northeast Thailand and Laos are close to each other geographically, the paternal mutation may evolve irrespective of the founder effect. While p.Gly701Asp heterozygotes do not manifest abnormal red cell morphology,19 homozygotes show oval red cells that are similar to those of SAO.81220 Unfortunately, we could not confirm red cell morphology in our patients.
The p.Ala858Asp mutation is geographically widespread, and cases have been reported not only from Southeast Asia, but also from Oman, India, and Papua New Guinea.1314 In contrast, the ΔVal850 mutation is confined to Papua New Guinea.
According to a comprehensive series of clinical and epidemiological studies in 78 patients with AR dRTA,15 the average age at clinical presentation was 4 years, but included many infants aged less than a year. The major presenting symptom was failure to thrive, with body weights usually less than the third centile. Rickets was noted in 74% of the patients, and medullary nephrocalcinosis in 80% of the patients who underwent renal imaging studies. Our patients presented typical clinical features of failure to thrive, rickets, and medullary nephrocalcinosis. However, adequate supplementation of alkali and potassium resulted in a remarkable improvement of growth retardation and skeletal deformities of the patients.
In conclusion, we have reported three patients with AR dRTA from 2 unrelated Lao families. All patients harbored the same homozygous SLC4A1 mutation, p.Gly701Asp. Although this is the first case report of AR dRTA from Laos, the homozygosity in the patients suggests that there may be more undiagnosed patients in Laos.
 XML Download
XML Download