

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Anterior cervical spine surgery (ACSS) is a common procedure performed for cervical spine disease.1 It is a successful surgical technique with good clinical outcomes and low complication rates.23 Postoperative airway complication rates after isolated ACSS are approximately 1.7%–6.1%.45 Despite these low incidence rate, the risk for airway compromise from prevertebral soft-tissue swelling, hematoma formation or direct injury from instrumentation can be fatal.678910 These life-threatening airway distresses should be managed initially with endotracheal intubation or tracheostomy.11 However, unplanned reintubation or tracheostomy after cervical surgery may result in plate or graft displacement, hypoxia or even death.8 To avoid these issues, overnight intubation is often recommended to protect airway patency.10 Nevertheless, there is no standard guideline for decision of extubation and hence extubation is usually performed on postoperative day 1. Prolonged intubation has some apparent adverse impact as well,12 causing discomfort to conscious patients. Hence, we analyzed the potential risk factors that may have clinical impact on patients with ACSS for time of extubation.
METHODS
Following Institutional Review Board approval, we retrospectively reviewed patients from our medical center diagnosed with cervical spinal disease, those who received operation from January, 2008 to December, 2016. All cervical spine pathologies of C1 to C7 were included. A total of 400 patients with cervical pathologies were treated with ACSS at our institute. All operations were performed by 3 experienced neurosurgeons in our single institute. For more concrete analysis, trauma patients with spinal cord injury (SCI) were excluded as they often have respiratory complications associated with morbidity and mortality.1314 Also, operation technique with solely posterior cervical approach was not included; anterior approach or combined anterior and posterior were included.
Patients with prolonged intubation (defined as intubation maintained for more than 24 hours in our study), or those required an unplanned reintubation within 7 days of operation were identified and compared with group of patients with no airway complication postoperatively. Preoperative patient data (characteristics, medical history, and operative indications), intraoperative data (operative type, combined anterior and posterior surgery, operative time, number of cervical level fused, level of cervical operation, blood transfusion, and estimated blood loss [EBL]), and postoperative outcomes (time to extubation and reintubation) were collected. Patient characteristics include age, sex, body mass index (BMI), current smoking history, anterior neck surgery history, and medical comorbidities (asthma, hypertension [HTN], diabetes mellitus [DM], congestive heart failure [CHF] or ischemic heart disease [IHD], chronic renal failure [CRF], and liver cirrhosis [LC]). The types of operative indications were degenerative, ossification of the posterior longitudinal ligament (OPLL), tumor, deformity, and infection. The types of operative techniques were anterior cervical discectomy and fusion (ACDF), anterior cervical corpectomy and fusion (ACCF), total disc replacement (TDR) and others (anterior cervical osteophytectomy, tumor removal, etc.). Preoperative radiographic studies, like plain radiographs, computed tomography (CT) scans, and magnetic resonance (MR) images were performed to all patients. The operative decisions like technique, number or location of cervical levels were at the discretion of the attending staff.
General endotracheal intubation was routinely performed under conscious sedation for patient undergoing ACSS. The routine anterior cervical approach was used for all ACSS procedures, and patients were transferred to the intensive care unit (ICU) under intubation after ACSS.
After the operation, extubation was performed when patient showed alert consciousness and active breathing in intubated status. If not, they were kept intubated until full recovery. Physicians and nursing staff were available at the time of extubation to prepare for reintubation in case of respiratory distress. The plain lateral cervical spine X-ray was performed within 12 hours of post-surgery to evaluate the prevertebral soft tissue swelling. The anteroposterior length of the prevertebral soft tissue was measured both at C2 and C5 level. If the length of the swollen area was increased above a threshold level (above 250% at C2 or 150% at C5) on X-ray compare to preoperative image, it was defined as meaningful prevertebral soft tissue swelling. When extubation was performed, patients were observed in the ICU for a minimum of 6 hours for safety and transferred to a general ward.
Statistical analysis
All statistical analyses were performed using SPSS (version 21, SPSS Inc., Chicago, IL, USA). The statistical significance was tested using a Fisher's exact test for categorical variables, and an unpaired Student's t-test or Mann-Whitney U-test for continuous variables. Univariate and multivariate logistic regressions using backward elimination method (95% confidence interval) were performed to assess the possible risk factors related to clinical outcome on prolonged intubation or reintubation. All values are reported as a mean ± standard deviation. P value of < 0.05 indicates statistical significance. The primary outcome measure was the rate of prolonged intubation defined in our study or unplanned reintubation within 7 days of operation.
RESULTS
A total of 400 ACSS were analyzed between 2008 and 2016. Among these patients, 389 patients (97.25%) extubated within 24 hours of surgery without airway complication (group 1). There were patients with prevertebral soft tissue swelling in Group 1, but not reaching threshold level on postoperative X-ray and no evidence of respiratory distress. Eleven patients (2.75%) showed postoperative airway compromise that needed further managements (group 2): 7 patients (1.75%, group 2A) needed prolonged intubation, and 4 patients (1.00%, group 2B) required unplanned reintubation. The mean times for extubation in group 1, 2A, and 2B were 2.75 hours (range: 0–23 hours), 76 hours (range: 24–250 hours), and 6 hours (range: 0–20 hours), respectively. In group 2B, the mean elapsed time for reintubation after extubation was 60.75 hours (range: 21–108 hours). For patients with prolonged intubation, there was no airway-related complication after extubation. However, there was a case of postoperative pneumonia in group 2A, which led to respiratory distress and resulted in prolonged intubation until postoperative day 11. In group 2B, whom required unplanned reintubation, emergency tracheostomy was performed in 1 patient (25%, 1/4) due to reintubation failure resulting from severe laryngeal edema. Also there was a single case (25%, 1/4) of expired patient in this group after reintubation due to distal tracheal obstruction followed by cardiac arrest. Other 2 patients showed no further respiratory complications after reintubation (Fig. 1). Among prolonged intubated patients, all were cases of prevertebral soft tissue swelling except for 1 case with postoperative hematoma in our study (Fig. 2). The patient was managed with prolonged intubation as there was a finding of prevertebral soft tissue swelling on postoperative X-ray. The emergency operation was performed on the next day as anterior neck swelling was much increased. The summary of 11 patients (group 2A and 2B) is presented in Table 1.
Fig. 1
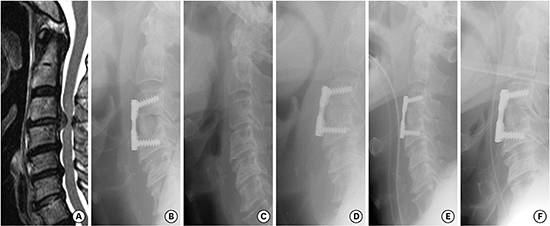
Radiological features of the patient with reintubation after ACSS. (A) A 73-year-old male patient (case No. 9) showing herniated intervertebral disc C3–C4 with severe spinal cord compression on sagittal MR imaging. Anterior cervical discectomy C3–C4 and fusion using iliac bone graft was performed. Extubation was conducted on the day of operation as the patient has no respiratory distress and immediate postoperative plain lateral X-ray revealed (B) only mild prevertebral soft tissue swelling compared to (C) preoperative film. (D) On postoperative day 4, the patient began complaining of difficult breathing and plain lateral X-ray showed markedly increased prevertebral soft tissue swelling. (E) We decided to reintubate the patient to protect the airway patency. (F) The patient was intubated for 4 days and extubated on postoperative day 8. The patient was discharged from hospital on postoperative day 14 without any further respiratory distress.
ACSS = anterior cervical spine surgery, MR = magnetic resonance.

Fig. 2
Radiological features of the patient with prolonged intubation due to cervical hematoma after ACSS. (A) A 52-year-old female patient (case No. 4) showing herniated intervertebral disc C5–C6, C6–C7 right on sagittal MR imaging. Anterior cervical discectomy C5–C6, C6–C7 and fusion using Solis cage with polybone were performed. Immediate postoperative plain lateral X-ray showed (B) mild prevertebral soft tissue swelling compared to (C) preoperative film. Prolonged intubation was decided to protect airway patency. (D) On postoperative day 1, the patient showed desaturation with severe anterior neck swelling and increased soft tissue swelling at the operation level on plain lateral X-ray. (E) Contrast enhanced neck CT scan revealed hematoma (marked in yellow circle) compressing trachea to the left side. Emergent hematoma evacuation was followed and injured right thyroid artery was noted. (F) Immediate postoperative plain lateral X-ray showed much decreased prevertebral soft tissue swelling. Extubation was conducted 4 days after hematoma evacuation. The patient was discharged from hospital on postoperative day 10 without any respiratory complication.
ACSS = anterior cervical spine surgery, MR = magnetic resonance, CT = computed tomography.

Table 1
Clinical data of 11 patients whom required prolonged intubation or reintubation
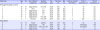
Op. = operation, EBL = estimated blood loss, HTN = hypertension, DM = diabetes mellitus, ACDF = anterior cervical discectomy and fusion, n/a = not applicable, OPLL = ossification of the posterior longitudinal ligament, ACCF = anterior cervical corpectomy and fusion, CRF = chronic renal failure.
aElapsed time to extubate the patient after the initial operation in reintubation cases.
The statistical analysis of preoperative parameters between 2 groups (group 1 vs. group 2) is as follow; the mean age (53.34 vs. 62.00, P = 0.015), female gender (37.53% [146/389] vs. 63.63% [7/11], P = 0.114), the mean BMI (24.72 vs. 24.63, P = 0.954), current smoking history (42.67% [166/389] vs. 27.27% [3/11], P = 0.369), anterior neck surgery history (3.60% [14/389] vs. 0% [0/11], P = 1.000), medical comorbidities; asthma (0.51% [2/389] vs. 9.09% [1/11], P = 0.080), HTN (29.82% [116/389] vs. 45.45% [5/11], P = 0.319), DM (14.40% [56/389] vs. 54.55% [6/11], P = 0.003), CHF or IHD (4.88% [19/389] vs. 0% [0/11], P = 1.000), CRF (1.03% [4/389] vs. 9.09% [1/11], P = 0.131), and LC (0.26% [1/389] vs. 0% [0/11], P = 1.000), and operative indication (P = 0.117). Intraoperative parameters were also analyzed; operative techniques (P = 0.301), combined anterior and posterior approach (2.57% [10/389] vs. 0% [0/11], P = 1.000), operative time longer than 5 hours (19.28% [75/389] vs. 45.45% [5/11], P = 0.048), cervical level fused (≥ 2 levels) (47.81% [186/389] vs. 54.55% [6/11], P = 0.764), cervical level involving above C3-C4 (11.57% [45/389] vs. 27.27% [3/11], P = 0.134), transfusion (1.54% [6/389] vs. 0% [0/11], P = 1.000), EBL greater than 300 mL (6.94% [27/389] vs. 27.27% [3/11], P = 0.042). The baseline characteristics and outcomes of the 2 groups are summarized in Table 2.
Table 2
Analysis of characteristics and outcomes for patients after ACSS
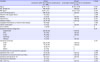
Data shown are number (%) not otherwise specified and plus-minus values are means ± standard deviation.
ACSS = anterior cervical spine surgery, BMI = body mass index, OPLL = ossification of the posterior longitudinal ligament, ACDF = anterior cervical discectomy and fusion, ACCF = anterior cervical corpectomy and fusion, TDR = total disc replacement, EBL = estimated blood loss.
Univariate logistic regression analysis was performed to screen out statistically significant factors that may have associations with prolonged intubation or reintubation, followed by a multivariate analysis to interpret the relationship between the foregoing factors and the incidence rate of airway compromise after ACSS. In univariate analysis, older age (OR [odds ratio], 1.065; 95% CI, 1.011–1.121; P = 0.017), asthma (OR, 19.350; 95% CI, 1.619–231.337; P = 0.019), DM (OR, 7.136; 95% CI, 2.106–24.173; P = 0.002), operative time longer than 5 hours (OR, 3.489; 95% CI, 1.037–11.738; P = 0.044) and EBL greater than 300 mL (OR, 5.028; 95% CI, 1.261–20.051; P = 0.022) were shown to have statistically significant values. In multivariate analysis, asthma (OR, 41.375; 95% CI, 3.088–554.298; P = 0.005) and DM (OR, 8.866; 95% CI, 2.425–32.417; P = 0.001) showed statistical significance (Table 3).
Table 3
Association between prolonged intubation (≥ 24 hours) and reintubation with clinical risk factors using univariate and multivariate linear regression model

DISCUSSION
Literatures report the rate of airway complications after ACSS as approximately 6%,6 and about one third of these complications result in the need for reintubation. Fatal loss of airway is the most devastating potential outcome after cervical spine surgery.10 Although need for prolonged intubation or reintubation has a substantial adverse impact on patients, clinicians must be aware that these patients are at risk for loss of airway.12 Also, failed extubation result in prolonged ICU stay, pneumonia, tracheostomy and even death.151617 Despite that morbidity can possibly arise due to these catastrophic events, literatures directly addressing these issues are still lacking. To our knowledge, little investigation has been devoted to specifically identifying ACSS risk factors related to airway distress postoperatively and there were no reports to date establishing exclusively guidelines for extubation. Hence, patient and operative factors that are potentially associated with airway complications remained to be elucidated.
We have reviewed the postoperative course in patients with ACSS to analyze risk factors associated with prolonged intubation or reintubation. The potential risk factors were previously reported by some authors. Emery et al.10 first reported that asthma and smoking were risk factors for upper airway obstruction after multilevel cervical corpectomy. The idea of overnight intubation and direct fiberoptic visualization of reactive tracheal swelling to determine extubation after multilevel anterior corpectomy with fusion was brought up by Epstein et al.8 They showed asthma, obesity greater than 220 lbs, operation time longer than 10 hours, transfusion, reoperation, and fusion involving C2 level were risk factors. Interestingly, other literatures highlight the importance of intraoperative factors, rather than patient characteristics. Kwon et al.9 studied 24 patients and reported that patient factors (age, weight, and medical comorbidities) were not significantly related to prolonged intubation in single stage, multilevel combined anterior and posterior cervical surgery. They concluded that intraoperative factors like total operative time, blood transfusion, and volume of crystalloid replacement were more significantly correlated. Sagi et al.6 involved 311 patients in their study and showed that characteristics including age, smoking, BMI and medical comorbidities were not significantly related to postoperative airway complication. However, our study with larger sample size showed both patient and intraoperative factors to be significantly related to postoperative airway compromise: older age, DM, operation time longer than 5 hours and EBL greater than 300 mL. Interestingly, female gender approached significant value in univariate analysis (OR, 2.913; P = 0.093). There is 1 published study noted a same result that female patients are in higher risk for prolonged intubation after ACSS.18 Possible causes include mucous membrane in male patients are more tolerable to trauma, whereas smaller tracheal diameter in female patients are more fragile to injury.19
One method to avoid airway compromise after ACSS was overnight intubation.8 Maintaining the patent airway until pharyngeal edema subsides is a key method to reduce the risk of post-extubation airway complication.10 Our study corroborates the above findings. Seven patients were managed with prolonged intubation postoperatively and showed no airway complication after extubation. However, 4 reintubated patients were initially extubated within 24 hours of surgery as there was no definite evidence of airway distress. Three patients from this group had risk factors that were significantly correlated. Hence, we recommend a safe prolonged intubation (more than 24 hours) for patients with risk factors even if there are no sign of respiratory distress.
The minimum time for airway distress to occur after extubation is yet unclear. Respiratory distress after ACSS occurs within the median time between 23–37 hours.610 The maximum prevertebral soft tissue swelling after ACSS is reported to be between postoperative day 2 and 3.5 Four reintubated patients in our study also showed median time of 54.75 hours for respiratory symptom to occur after initial extubation. Hence, postoperative airway protection should be further beyond till this time. However, clinicians often perform overnight intubation and conduct extubation on the next postoperative day within 12–18 hours of the surgery.20 The overnight intubation management should be extended if there is evidence of risk factors identified in our study. On the other hand, we recommend to extubate the patient early as possible if there are no risk factors, as the airway distress are less likely to occur.
Edema of the laryngopharynx and prevertebral soft tissue swelling are the most common causes for postoperative airway compromise.610 Surgeons must be aware of intraoperative managements that may help to low the risk of soft tissue damage. The key factors are operative time and amount of blood loss as shown in our study. The primary goal is definitely pursuing shorter time of operation with a good clinical outcome. The retractors should be frequently released to avoid tissue ischemia during the operation as prevertebral soft tissue edema results from tissue damage.21 We assumed that increased blood loss during operation may be related to soft tissue injury and hence higher chance of bleeding at operation site resulting in airway compression. Other fundamental technique like meticulous bipolar coagulation should always be considered. Most importantly high risk bleeding patients should be well prepared preoperatively with anesthesia staff.
Limitations of our study lies in its retrospective nature performed in a single institution and criteria determining extubation time used in our series had subjective aspects. Thus prospective study with objective extubation criteria should be needed to analyze precise factors regarding airway problems after ACSS. The other possible factors include the degrees of tissue retraction during surgery which may reflect the severity of airway swelling is not being fully considered. The strengths of our study were relatively large sample size with long observation period. However, due to the low prevalence of prolonged intubation and reintubation for ACSS patients (11/400, 2.75% in our study), statistically analyses might have been underpowered and making it difficult to identify all possible significant factors that impacted clinical outcome.
In conclusion, we showed that postoperative airway compromise is related to both patient and operative factors in our study. Patient's characteristics like age, sex and medical comorbidities are not adjustable. However, perioperative factors including operative time and the amount of blood loss are within the control of the operating team. Hence, we advocate prolonged intubation for patients whom are exposed to these risk factors to perform a safe and effective extubation. Even though patients may experience discomfort during prolonged intubation, all resulted in a safe extubation.
 XML Download
XML Download