

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Prostate cancer (PCa) has an extremely heterogeneous clinical course, ranging from indolent and organ-confined to aggressive, metastatic lethal disease.1 Consequently, the tumor characteristics of PCa need to be accurately assessed so that suitable therapeutic options can be considered. Currently, serum prostate-specific antigen (PSA) levels and histopathological analysis, including the tumor grade and tumor stage as measured by the Gleason score, are the primary determinants of therapeutic decisions. However, none of the bio-markers or histological criteria reported to date have appropriate sensitivity and specificity for detecting, monitoring, or determining the prognosis of PCa.23 Thus, there are crucial methods capable of predicting clinical outcomes and responses to appropriate treatment in patients with PCa. The abnormal expression of certain genes in cancer cells is closely related to various aspects of tumor progression, including tumor growth, invasion, and metastasis. Proper cell division requires the precise coordination and execution of several events in the cell cycle, including centrosome duplication, DNA replication, mitotic spindle assembly, chromosome segregation, and cytokinesis.4 The failed execution or mistiming of any of these events can lead to chromosome segregation defects, resulting in aneuploidy or polyploidy.567
Cell division cycle 6 (CDC6), a multi-functional molecular switch, is an important regulator of DNA replication and plays essential roles in the activation and maintenance of the checkpoint mechanisms in the cell cycle.8 CDC6 belongs to the AAA+ (ATPases associated with diverse cellular activities) family of ATPases with chaperone-like activities and was initially identified in a genetic screen aimed at detecting mutations that arrest the budding yeast cell cycle.9 The human CDC6 gene is mapped to chromosome 17q21.3 and its expression is regulated by the E2F family of transcription factors that control S phase-promoting genes.101112 CDC6 is also a component of a pre-replication complex that forms at the origins of DNA replication in early G1 phase and initiates DNA replication during S phase. CDC6 is involved in checkpoint mechanisms that coordinate S phase of the cell cycle and mitotic entry. By coupling DNA replication and the cell cycle S-M phase checkpoint, CDC6 ensures the entire genome is replicated only once per cell division.8 Many previous studies indicate that abnormal expression of CDC6 plays an important role in several human malignancies such as brain tumors,13 hepatocellular carcinoma,14 lung cancer,15 and ovarian cancer.1617 High expression of CDC6 detected by immunohistochemical (IH) staining and Western blotting is associated with a higher tumor grade and a more advanced stage. Although protein expression of CDC6 is elevated around S phase in the LNCaP PCa cell line,18 the clinical significance of CDC6 in PCa remains unclear to the best of our knowledge.
The aim of the current study was to assess the clinical significance of CDC6 in PCa using real-time quantitative polymerase chain reaction (RT-qPCR) and IH staining.
METHODS
Study population
This case-control study included 121 cases of newly diagnosed PCa and 66 age-matched benign prostatic hyperplasia (BPH) controls. The study cases were recruited from among patients with histologically confirmed primary adenocarcinoma of the prostate at our institution. Controls were selected from a database of BPH patients who underwent transurethral resection of the prostate (TURP) and were matched according to age and date of blood sampling. Controls with serum PSA levels > 2.5 ng/mL underwent transrectal prostate biopsy before TURP to rule out the presence of cancer, and those with PSA levels > 10 ng/mL were excluded from the study. Subjects with a suspicious history of previous management for PCa or incomplete medical records were also excluded. The Gleason score and 2002 tumor stage, lymph nodes, metastasis (TNM) stage were used as prognostic factors. The Gleason score was measured from 12-core transrectal biopsy, TURP, or radical prostatectomy specimens. Tumor stage was estimated from radical prostatectomy specimens or from computed tomography, magnetic resonance imaging, or bone scan results.
RNA extraction and construction of cDNA
Total RNA was separated from tissue homogenized in a 5 mL glass tube in 1 mL TRIzol (Invitrogen, Carlsbad, CA, USA). The homogenate was transferred to a 1.5 mL tube and mixed with 200 μL chloroform. After incubation for 5 minutes at 4°C, the homogenate was centrifuged for 13 minutes at 13,000 g and 4°C. The upper aqueous phase was transferred to a clean tube, 500 μL isopropanol was added, and the mixture was incubated for 60 minutes at 4°C. The sample was then centrifuged for 8 minutes at 13,000 g and 4°C. Then, the upper aqueous phase was removed, mixed with 500 μL of 75% ethanol, and centrifuged for 5 minutes at 13,000 g and 4°C. After the upper aqueous layer was discarded, the pellet was dried at room temperature, dissolved in diethylpyrocarbonate-treated water, and stored at −80°C. The quality and integrity of the RNA were confirmed by agarose gel electrophoresis and ethidium bromide staining. cDNA was then prepared from 1 μg total RNA using the First-Strand cDNA Synthesis kit (Clontech, TAKARA, Otsu, Japan) according to the manufacturer's protocol.
RT-qPCR
To quantify the expression of CDC6, real-time PCR was performed using a Rotor Gene 6000 instrument (Corbett Research, Mortlake, Australia). Real-time PCR assays using SYBR Premix Ex Taq (Takara Bio Inc., Otsu, Japan) were carried out in micro-reaction tubes (Corbett Research) using CDC6 sense (5′-CTC CAG TGA TGC CAA ACT AG-3′) and antisense (5′-TGG TGA ACT TTG GCT AGT TC-3′) primers. PCR was performed in a final volume of 10 μL consisting of 5 μL 2 × SYBR Premix Ex Taq buffer, 0.5 μL of each primer (10 pmol/μL), and 2 μL cDNA. The product was purified with a QIAquick Extraction Kit (QIAGEN, Hilden, Germany), quantified with a spectrometer (Perkin Elmer MBA-2000; Perkin Elmer, Fremont, CA, USA), and sequenced with an automated laser fluorescence sequencer (ABI PRISM 3100 Genetic Analyzer; Applied Biosystems, Foster City, CA, USA). The product was serially diluted from 100 pg/μL to 0.1 pg/μL to establish a standard curve. The real-time PCR conditions were as follows: 1 cycle of 20 seconds at 96°C, followed by 45 cycles of 2 seconds at 96°C for denaturation, 20 seconds at 52°C for annealing, and 20 seconds at 72°C for extension. The melting program was performed at 72°C–99°C, with a heating rate of 1°C per 45 seconds. Spectral data were captured and analyzed using Rotor Gene Real-Time Analysis Software 6.0 Build 14 (Corbett Research). All samples were run in triplicate. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used as an endogenous reference gene. CDC6 expression was normalized to the expression of GAPDH.
IH staining of CDC6 in PCa and BPH tissues
Paraffin blocks from ten CaP cases and five BPH controls were available for IH analysis. Tissue sections were cut and placed on SuperfrostPlus microscope slides (Fisher Scientific, Cheongju, Korea). Using the Benchmark XT automated immunohistochemistry stainer (Ventana Medical Systems, Tucson, AZ, USA), tissues were stained as follows. Detection was performed using a Ventana Ultraview DAB Kit (Ventana Medical Systems). Sections were deparaffinized using EZ Prep solution. CC1 standard (Tris/Borate/EDTA buffer, pH 8.4) was used for antigen retrieval. DAB inhibitor (3% H2O2, endogenous peroxidase) was blocked for 4 minutes at 37°C. Sections were incubated with an anti-CDC6 primary antibody (Abcam Inc., San Diego, CA, USA) for 40 minutes at 37°C and then with the Universal HRP Multimer secondary antibody for 8 minutes at 37°C. Slides were stained with DABþH2O2 substrate for 8 minutes followed by hematoxylin and bluing reagent counterstain at 37°C. Reaction buffer (Tris buffer, pH 7.6) was used for washing. The staining intensity and proportion of positively stained epithelial cells were evaluated. CDC6 localized primarily in the cytoplasm. The staining intensity was classified as follows: none (0), weak (1), moderate (2), and strong (3). Each specimen was examined and scored separately by three investigators, and discrepancies were discussed until agreement was reached.
Statistical analysis
Clinical variables such as age and PSA levels were compared using the Mann-Whitney U test. Spearman's rank correlation coefficient was calculated to evaluate the association between CDC6 mRNA and protein expression levels. Receiver operating characteristic (ROC) curves were used to identify the optimal cutoff point for each risk score that yielded the highest combined sensitivity and specificity. To evaluate tumor characteristics, Gleason scores were classified as ≤ 7 and ≥ 8, and the clinical stage was categorized as T2, T3a, T3b, and T4. Multivariate logistic regression analysis was performed to assess the association between CDC6 tissue mRNA expression and clinicopathological parameters in patients with advanced disease or metastasis (odds ratio [OR] and 95% confidence interval [CI]). Statistical analysis was performed using IBM SPSS 23.0 software (IBM Co., Armonk, NY, USA), and a P value < 0.05 was considered statistically significant.
Ethics statement
The Ethics Committee of Chungbuk National University approved the protocol, and written informed consent was obtained from each subject. The collection and analyses of all samples were approved by the Institutional Review Board (IRB) of Chungbuk National University (IRB approval No. 2010-12-010), and informed consent was obtained from each subject.
RESULTS
Baseline characteristics
Table 1 lists the baseline clinical and pathological characteristics of the 66 BPH controls and 121 PCa patients. The median age of the PCa patients was 68.3 years (range, 42–86 years). Among the 121 PCa patients, 103 (85.1%) patients underwent radical prostatectomy and the other 18 (14.9%) patients underwent palliative TURP. At the time of diagnosis, 39 (32.2%) patients had T2 stage, 30 (24.8%) had T3a stage, 30 (24.8%) had T3b stage, and 22 (18.2%) had T4 stage (metastasis). In total, 70 (57.9%), 12 (9.9%), 38 (31.4%), and 1 (0.8%) patients had a Gleason score of 7, 8, 9, and 10, respectively.
Table 1
Comparison of clinicopathologic characteristics between PCa cases and controls
Expression levels of CDC6 mRNA in BPH and PCa tissues

Relationship between CDC6 tissue mRNA expression levels and clinicopathological features
CDC6 mRNA expression was significantly higher in patients with elevated PSA levels (> 20 ng/mL) than in those with low PSA levels (P < 0.001) (Table 2). In addition, CDC6 expression was significantly higher in cancer tissue specimens from patients with a high Gleason score and advanced stage than in samples from those with a low Gleason score and earlier stage, respectively (P < 0.005 in each case) (Table 2 and Fig. 2).
Table 2
CDC6 mRNA expression levels according to the PSA level, Gleason score, and PCa stage

Multivariate logistic regression analysis between CDC6 tissue mRNA expression and advanced disease and metastasis
The area under the ROC curve of CDC6 expression in advanced stage (≥ T3b) was 0.735 (Fig. 3). The highest combined sensitivity of CDC6 expression in advanced stage (T3b and T4) was 73.1%, and specificity was 66.7%. High CDC6 tissue expression was significantly associated with advanced stage (OR, 3.005; CI, 1.212–7.450; P = 0.018) and metastasis (OR, 4.192; CI, 1.079–16.286; P = 0.038) (Table 3).
Fig. 3
ROC curve analysis of CDC6 expression according to the T stage (≤ T3a and ≥ T3b).
ROC = receiver operating characteristic, CDC6 = cell devision cycle 6, AUC = area under the curve.
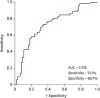
Table 3
Multivariate logistic regression analysis of CDC6 expression as a prognostic marker of advanced disease and metastasis

IH staining of CDC6 in PCa and BPH tissues
The presence of CDC6 protein was assessed in ten PCa and five BPH samples by IH staining (Fig. 4). CDC6 localized primarily in the cytoplasm in cancer tissues. Cytoplasmic staining of CDC6 correlated well with CDC6 mRNA expression (Spearman's correlation, r = 0.576, P = 0.025). The pattern of CDC6 staining was different in BPH tissue; there was intense staining in stromal muscle cells, but the cytoplasm and nuclei of glandular epithelial cells were weakly stained. The staining intensity of CDC6 was significantly higher in PCa tissue than in BPH tissue (P = 0.015). Interestingly, intense staining of CDC6 was significantly associated with a high Gleason score and advanced TNM stage (linear-by-linear association, P = 0.044 and P = 0.003, respectively).
Fig. 4
The IH staining pattern of CDC6 differs between BPH and PCa tissues (200× magnification). (A) Weak cytoplasmic staining intensity of CDC6 in BPH epithelial tissue. Note the intense staining in stromal muscle cells. (B) Moderate staining intensity of CDC6 in localized PCa with a Gleason score of 7 (3 + 4). (C) Strong staining intensity of CDC6 in advanced PCa with a Gleason score of 8 (4 + 4).
CDC6 = cell devision cycle 6, BPH = benign prostatic hyperplasia, PCa = prostate cancer.
DISCUSSION
In this study, we identified the clinical significance of CDC6 in PCa by performing RT-qPCR and IH staining. The level of CDC6 mRNA expression was higher in PCa tissues than in BPH tissues, and the increased expression of this gene was associated with a high Gleason score. Additionally, CDC6 mRNA expression was significantly higher in patients with elevated PSA levels (> 20 ng/mL) and advanced stage than in those with low PSA levels and earlier stage, respectively. IH staining for CDC6 yielded similar results. These results indicate that CDC6 expression is a novel diagnostic and prognostic marker of PCa.
The human CDC6 gene is mapped to chromosome 17q21.319 and CDC6 is an important component of pre-replication complexes. CDC6 is essential for DNA replication, and CDC6 silencing inhibits DNA replication and arrests cells in G1/S phase, resulting in an inability to enter S phase.2021 CDC6 silencing not only inhibits DNA replication but also leads to cell apoptosis.22 Jin and Fondell23 reported that CDC6 is a key regulatory target for the androgen receptor and it is a new mechanisms of PCa cell proliferation as an essential regulatory of G1-S phase progression. Aberrant CDC6 expression may cause malignant proliferation of cells and poses a serious risk of carcinogenesis. A few studies have probed the relationship between CDC6 and many cancers, such as cervical cancer,2425 lung cancer,15 oral squamous cell carcinoma,26 and ovarian cancer,1617 and found that the level of CDC6 expression is correlated with the extent of malignancy. Sun et al.17 revealed that CDC6 is highly expressed in ovarian tissues in contrast with normal ovarian cancer tissues and suggested that CDC6 is related to the stage of ovarian cancer. Deng et al.16 demonstrated that elevated levels of CDC6 are related to cellular proliferation and poor prognosis in epithelial ovarian cancer. Similarly, Zhang et al.15 found that the expression level of CDC6 is significantly higher in lung cancer tissue specimens than in normal lung tissues, and overexpression of CDC6 is associated with poor overall survival of lung cancer patients.
To the best of our knowledge, no study has addressed the prognostic implications of CDC6 in PCa. Our study focused on CDC6 mRNA and protein expression with respect to pathological phenotypes and oncological outcomes. CDC6 expression was significantly higher in PCa patients than in BPH controls. More importantly, the characteristics of PCa were more aggressive as CDC6 expression increased. Our result revealed that increased expression of CDC6 was associated with a high Gleason score, advanced stage, and metastasis. In addition to significant differences of expression of CDC6 expression in high Gleason score prostate tumors, we also found differential expression of CDC6 between Gleason score 7 tumors with primary Gleason grades 3 and 4. Because numerous studies suggest that Gleason 3 + 4 tumors have a better prognosis than Gleason 4 + 3 tumors, thus, it is important to distinguish Gleason 3 + 4 vs. 4 + 3 = 7 tumors.2728 On the other hand, we failed to find a significant expression of CDC6 between those with a total pretreatment serum PSA ≤ 4 vs. 4–10 vs. 10–20 ng/mL (data not shown). The only significant difference in CDC6 expression was observed between those with a total pretreatment serum PSA ≤ 20 vs. < 20 ng/mL. Clinically, the PSA level alone does not facilitate precise staging on an individual basis, although advanced stage tends to correlate with an increased PSA level.29 Therefore, the data presented here suggest that CDC6 expression could be a novel indicator of tumor aggressiveness in patients with PCa.
This study has a possible weakness. IH analysis was performed on a small number of samples. Nevertheless, this analysis is sufficient to demonstrate that cytoplasmic CDC6 staining correlates with CDC6 mRNA expression and that the pattern of CDC6 staining differs between BPH and PCa tissues and varies according to the aggressiveness of PCa.
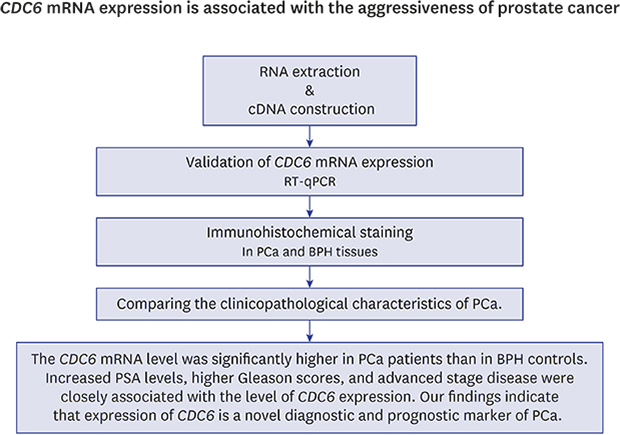
In conclusion, the CDC6 mRNA level was significantly higher in PCa patients than in BPH controls. Increased PSA levels, higher Gleason scores, and advanced stage disease were closely associated with the level of CDC6 expression. Our findings indicate that expression of CDC6 is a novel diagnostic and prognostic marker of PCa.
 XML Download
XML Download