

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Liver transplantation (LT) is the most effective therapy in carefully selected patients with hepatocellular carcinoma (HCC).1 Patients within the Milan criteria (MC) have shown 5-year recurrence-free survival and overall survival (OS) rates of 83% and 75%, respectively.2 However, post-transplant HCC recurrence is reported up to 8%–20% of cases in spite of stringent selection of transplant candidates.1345678 The majority of patients with HCC recurrence after LT have systemic tumor spreading not amenable to resection or locoregional therapies.34910 Moreover, transplanted patients are on multiple drugs including immunosuppressive agents, most of them are known to promote tumor growth.1112 Therefore, patients with systemic tumor recurrence generally show a dismal prognosis with a median survival of less than one year.513 Management of these patients is a challenging issue, however, there is no consensus treatment strategy regarding HCC recurrence not amenable to resection or locoregional therapies.
Sorafenib, a multi-tyrosine kinase inhibitor, is the first drug to demonstrate a significant improvement in the OS of patients with advanced HCC.14 It might be considered in selected cases of HCC recurrence after LT, when systemic treatment is warranted. However, only a few retrospective, small sized studies are available regarding the efficacy of sorafenib in these settings. A recent small case-control study showed that sorafenib seems to be associated with better survival compared to best supportive care (BSC) in this setting.15 In contrast, several studies reported that sorafenib seems to be poorly tolerated because of drug to drug interactions with immunosuppressive agents, and rarely effective.1617 Currently, the efficacy and safety of sorafenib in this setting are controversial.
In this study, we aimed to evaluate whether sorafenib, compared to BSC, could increase survival in patients with HCC recurrence after LT not amenable to surgical resection or locoregional therapies.
METHODS
Patients
This retrospective cohort study included patients who were diagnosed with recurrent HCC following LT between October 2000 and May 2015 at Seoul National University Hospital (Seoul, Korea). Patients were divided into two groups according to treatment regimens after development of HCC not amenable to resection or locoregional treatment (untreatable progression [UP]).15 Patients treated by sorafenib after presenting with UP were classified as the sorafenib group, and those received only BSC including palliative radiotherapy to extrahepatic metastasis were classified as the control group.
Treatment of recurrence and outcomes
After LT, all patients were monitored with dynamic computed tomography (CT) scans or magnetic resonance imaging (MRI) every 2–4 months for the first 2 years and every 3–6 months thereafter. HCC recurrence was either confirmed by histology or diagnosed according to the non-invasive criteria of the American Association for the Study of Liver Disease.18
Treatment of HCC recurrence was discussed and decided at multidisciplinary team meeting. Treatment strategy was carefully aimed, whenever possible, at complete surgical removal of recurrence. Radiofrequency ablation (RFA) was performed in patients with up to three intrahepatic recurrences (≤ 3 cm in size) for which resection was not feasible. Transarterial chemoembolization was considered in patients with 1) multi-nodular HCCs (more than three, > 3 cm in size); or 2) risky or inaccessible lesions for RFA (i.e., hepatic dome or perivascular lesions). When tumor was deemed not anymore eligible to resection or locoregional therapies according to these criteria, patients received systemic chemotherapy or BSC until 2007, and received sorafenib based treatment or BSC thereafter. Sorafenib was initiated at a dosage of 400 mg twice daily. In case of adverse events (AEs), the dose was tapered to 400 mg/day and eventually to 400 mg every other day, according to severity and persistence of symptoms. Sorafenib was withdrawn in case of serious AEs or radiological tumor progression according to Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria.
The primary study objective was evaluation of the efficacy of sorafenib in patients with no otherwise treatable HCC recurrence after LT compared to BSC, according to survival time. Survival time was analyzed in two ways: 1) as the interval between tumor recurrence and death (survival after recurrence); 2) as the interval between UP and death (survival after UP).
A toxicity profile was also evaluated in those patients according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0.
Statistical analyses
The Mann-Whitney U test and Kruskal-Wallis test were used to analyze differences between the groups. The χ2 test or Fisher's exact test was used for categorical data. The cumulative rate of survival was calculated using the Kaplan-Meier method and the log-rank test was performed to compare the differences between the groups. Cox proportional hazards models were used to assess the influence of the clinical variables outcome. Considering that the investigated patients were selected as having UP, we used a left-truncated Cox proportional hazard regression model for the analysis of survival after recurrence to account for the interval between posttransplant HCC recurrence and assessment of UP (median, 11 months). Differences at P < 0.05 were considered statistically significant. The statistical analyses were performed using SPSS for Windows, version 22.0 (SPSS Inc., Chicago, IL, USA) and R language ver. 3.2.0 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
The present study conformed to the ethical guidelines of the World Medical Association Declaration of Helsinki, and was approved by the Institutional Review Board (IRB) of the Seoul National University Hospital (IRB No.: H-1608-019-781). Documentation of informed consent was waived by the IRB because of the anonymous evaluation of data.
RESULTS
Baseline characteristics
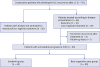
During the study period, 502 patients underwent LT for HCC, 70 of whom developed recurrent HCC. Twenty-five patients presented upfront with a disease not amenable to resection, ablation or locoregional treatments, while 45 received multiple treatments until development of UP. Of the 45 patients, four patients were cured by resection or ablation and did not need any further treatment, and one patient was lost to follow-up. Of the 65 patients presented with UP, 45 patients treated by sorafenib and 20 patients receiving BSC constituted our study population (Fig. 1).
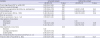
The baseline characteristics of patients are described in Table 1. The median age at HCC recurrence after LT was 55 years (interquartile range [IQR], 49–62 years) and 55 (84.6%) patients were males. Hepatitis B virus infection was the most common etiology of the underlying liver disease. Fifty-two patients (80.0%) underwent living-donor LT (LDLT). Forty-nine patients (75.4%) were beyond MC at pre-transplant staging, and micro-vascular invasion was present in 35 cases (53.8%) at explant pathology. The median time from LT to recurrence was 8.2 months (IQR, 3.2–12.3 months). Recurrence was limited to the liver in 5 patients (7.7%), was limited to extrahepatic lesion in 30 patients (46.2%), and was both intrahepatic and extrahepatic in 30 patients (46.2%) at the time of recurrence. Patients underwent resection or locoregional treatments (range, 0–8) until developing UP. The median time from LT to UP was 11.2 months (IQR, 4.4–20.0 months).
Table 1
Baseline characteristics of patients according to treatment group

Data are presented as median (interquartile range) or number (%), unless otherwise indicated.
BSC = best supportive care, HBV = hepatitis B virus, HCV = hepatitis C virus, LT = liver transplantation, MC = Milan criteria, MVI = microvascular invasion, mTOR = mammalian target-of-rapamycin, AFP = α-fetoprotein, PIVKA–II = prothrombin in vitamin K absence–II, MELD = model for end-stage liver disease, UP = untreatable progression.
Clinical characteristics were similar across the treatment groups except immunosuppressive strategy. All patients in the sorafenib group received tacrolimus as main immunosuppressant, while 3 in the BSC group received cyclosporine. Calcineurin inhibitors were maintained in 60.0% of patients in the BSC group, while 93.3% of the sorafenib group switched to mammalian target-of-rapamycin (mTOR) inhibitors after HCC recurrence (P < 0.001).
Survival analysis
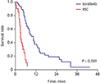
During the median follow-up period of 12.1 months (IQR, 5.7–20.9 months) after HCC recurrence, 57 out of 65 patients died. The median survival after recurrence and median survival after UP were 14.2 months (95% confidence interval [CI], 9.6–18.8) and 9.4 months (95% CI, 6.6–12.2) in the sorafenib group, while 6.8 (95% CI, 1.7–16.7) and 3.2 (95% CI, 2.8–3.6) months in the BSC group, respectively (Fig. 2). Treatment with sorafenib conferred a survival advantage as compared with BSC both for survival after recurrence (hazard ratio [HR], 0.59; 95% CI, 0.28–0.89; P = 0.02) and survival after UP (HR, 0.17; 95% CI, 0.09–0.34; P < 0.001), respectively. In multivariate Cox regression analyses, high serum AFP level, synchronous intrahepatic recurrence and distant metastasis at the time of recurrence, and receiving only BSC after UP were independently associated with poorer survival after recurrence (Table 2). Sorafenib treatment was independently associated with better survival after recurrence as compared with BSC (HR, 0.25; 95% CI, 0.10–0.62; P = 0.002). In addition, sorafenib was also independently associated with better survival after UP (HR, 0.13; 95% CI, 0.06–0.27; P < 0.001).
Fig. 2
Kaplan-Meier estimates of survival after recurrence and after UP. (A) Patients in the sorafenib group showed significantly longer survival after diagnosis of recurrence than those in the BSC group. (B) Patients in the sorafenib group showed significantly longer survival after UP than those in the BSC group.
UP = untreatable progression, BSC = best supportive care.

Table 2
Univariate and multivariate analyses of factors associated with survival after recurrence (corrected by time from recurrence to untreatable progression)
In the subgroup analysis, sorafenib enhanced survival after recurrence compared with BSC both in patients who presented with UP at recurrence and those who received multiple treatments until development of UP (P = 0.005 and 0.006, respectively, Supplementary Tables 1 and 2). In addition, sorafenib treatment was associated with better prognosis in patients with high α-fetoprotein (AFP) levels (≥ 200 ng/mL; P = 0.003), patients developing early recurrence after LT (< 1 year; P < 0.001), and patients who had recurrence limited to extrahepatic lesion at the time of recurrence (P = 0.04). Patients with low AFP levels (< 200 ng/mL), patients developing late recurrence after LT (≥ 1 year), and patients who had intrahepatic recurrence with/without distant metastasis also showed similar trends, although the differences were not significant because of the small number of patients.
AEs
The AEs during sorafenib were as following: hand-foot syndrome was observed in 4 patients (8.9%), diarrhea in 6 (13.3%), alopecia in one (2.2%), vomiting in one (2.2%) and abnormality of liver function test in 2 (4.4%), respectively. The AEs were well controlled by a dose reduction. Drug-related grade 4 or 5 toxicity did not occur. Sorafenib was withdrawn for progression of disease in 39 patients (86.7%), one patient for liver function test abnormality, one patient for vomiting, two patients for diarrhea and one patient for hand-foot syndrome.
DISCUSSION
In this largest single-center report of sorafenib for recurrent HCC following LT, sorafenib treatment was associated with better post-recurrence survival as compared with BSC. The associations were independent of other well-known prognostic factors including serum AFP level and patterns of tumor recurrence. In addition, treatment with sorafenib in the post-transplant setting showed tolerable toxicity.
According to the previous studies regarding post-transplant HCC recurrence, median survival after sorafenib treatment ranges between 17.8 and 38.5 months, suggesting an improvement of prognosis compared to BSC, albeit factors such as small sample size, the heterogeneity of the patients and treatment protocols may limit the conclusions.151619 Similarly, the non-adjusted median survival after recurrence and UP more than doubled in the sorafenib group compared to BSC group in our study. Although sorafenib group were more often on mTOR inhibitors because they were treated in the most recent years, pre- and post-transplant characteristics associated with prognosis, such as MC in or out, microvascular invasion, or time-to recurrence were comparable between sorafenib and BSC group. In addition, treatment with mTOR inhibitors was not significantly associated with prognosis in the multivariate analysis. Furthermore, initial treatment at recurrence, number of treatment until UP, and time to UP did not differ between two groups, suggesting consistent treatment policy regardless of different eras. These findings indicate that the survival difference between two groups may be mainly due to sorafenib treatment.
Meanwhile, the post-recurrence survival of sorafenib group in our study was relatively shorter than that of previous studies performed in Western transplant centers.15161920 It may be resulted from different baseline characteristics of patients. First, more than half of the patients in our study had advanced HCC beyond the MC, and the median time to recurrence after LT was shorter compared with that of previous reports, suggesting more aggressive tumor biology of our cases.21 Second, most patients (83.3%) in our study received LDLT. In the LDLT setting, the acceptable outcome might be lower than that of deceased donor LT (DDLT) as grafts are not public resources.722 In our institute, we use expanded criteria based on AFP, PIVKAII and PET positivity, and consider LDLT even in patients with advanced HCC if there is no other effective therapy and the expected survival/risk of recurrence after LT is acceptable in both donor and recipient.2324 As a result, patients with advanced HCC accounted more than half of the cases in our study. Furthermore, it has been suggested that LDLT is associated with higher post-transplant HCC recurrence rate, compared to DDLT because of release of growth factors that mediate rapid regeneration after implantation, shorter waiting time and fast track selection which might preclude the detection of aggressive tumor before LT.2526272829 Therefore, the poorer outcome of sorafenib group in our study compared to previous studies may be attributed to different baseline characteristics and unique features associated with LDLT. Nevertheless, the beneficial effect of sorafenib on survival was observed consistently even in the predominance of LDLT for HCC beyond the MC, supporting the potential role of sorafenib in post-LT HCC recurrence.
Dose reduction or withdrawn of sorafenib caused by AEs occurred only in 5 patients, and the overall AEs were acceptable with a comparable toxicity profile to the previous reports.151630 Our study shows that the tolerability of sorafenib for recurrent HCC after LT is comparable to the palliative setting of non-transplant HCC.
Combination of sorafenib and mTOR inhibitors has been an interesting issue because of the potential synergistic effects by targeting different major signaling pathways involved in hepatocarcinogenesis; b-Raf and mTOR/AKT.31 Preclinical reports suggest that the combination therapy has additive efficacy compared with sorafenib alone.3233 However, recent randomized phase II trial revealed that combination of sorafenib and everolimus did not improve OS compared with sorafenib alone in the first-line treatment of advanced HCC, although objective response favored the combination group.34 Consistent with this, combination of sorafenib and mTOR inhibitors did not significantly improve prognosis compared to sorafenib alone in our patients with post-LT HCC recurrence, although the interpretation may be limited due to the small sample size. It would be better to test the combination strategy in target-enriched populations such as those with mTOR pathway activation.
Our study has several limitations. First, it is based on retrospective observational data. The different treatment eras related to the time of introducing sorafenib might act as a historical bias in comparing the sorafenib and BSC groups. However, both cohorts received similar treatment strategy over time as shown by similar time-to-recurrence, initial patterns and treatment at recurrence, number of treatments until UP, and time-to-UP. The different immunosuppression strategy between two groups might be a potential bias. However, previous reports suggesting a benefit of mTOR inhibitor are based on uncontrolled pilot studies, and recent multi-center randomized trial showed that sirolimus did not improve long-term progression-free survival and OS compared with mTOR inhibitor-free immunosuppression in patients undergoing LT for HCC.35 Therefore, the benefit of mTOR inhibitor in post-LT HCC is still not clear and more data are awaited. Second, although this study is the largest single-center report of sorafenib for recurrent HCC following LT to our knowledge, it is based on a relatively small sample size. Because of the low incidence of post-LT HCC recurrence, multi-center, prospective cohort studies are needed to investigate this issue more in depth.
Post-transplant HCC recurrence rates may be increased gradually due to the expansion of LT in HCC. Therefore, refinement of treatment strategy regarding HCC recurrence after LT is highly relevant in clinical practice. Our data suggest the intriguing possibility of sorafenib in patients with post-transplant HCC recurrence. Furthermore, sorafenib seems to be well tolerated in post-transplant setting. Further larger, prospective studies performed in real-life cohort are warranted to validate the present results.
 XML Download
XML Download