

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A number of self-reporting questionnaires have been proposed to quantify subjective discomfort arising from the upper extremity, based on objective scales.1 One of the most widely used questionnaires is the Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) consisting of 30 items. The DASH has been translated into several languages and its validity, reliability and responsiveness have been verified in patients with a variety of upper extremity disorders.2
However, there are several limitations which should be overcome when clinicians apply DASH in routine outpatient clinics. First, it takes a long time to fulfill the total DASH questionnaire items to patients. Second, completion of the questionnaire by elderly patients is difficult respectively. With an aging society, with increasing elderly population diagnosed with disorders of upper extremities are increasing, and elderly patients with poor cognitive ability have been also increasing.3 Furthermore a few DASH questionnaire items show a low response rate, especially those pertaining to about sexual activities due to the unique sociocultural circumstances existing in Asia.4 Therefore, development of a concise version of self-reporting questionnaires regarding upper extremity conditions would be required.
A shorter version of DASH, known as Quick Disabilities of the Arm, Shoulder, and Hand questionnaire (QuickDASH), has been developed via a “concept-retention” approach.5 The QuickDASH consists of 11 items from the original DASH. The QuickDASH may be more appealing compared with DASH because shorter questionnaire is associated with a lower burden for the responders as well as the clinicians. Thus, QuickDASH has been translated into various types of languages and process of confirming effectiveness of QuickDASH in particular languages needs to be established before routine clinical applications.6
The validity, reliability, and responsiveness of the questionnaire translated into specific language needs to be confirmed to establish its effectiveness. The adaptation of Korean version of DASH (K-DASH) has been already carried out, however, there have been no studies which tried to reveal the validity, reliability, and responsiveness of Korean version of QuickDASH (K-QuickDASH).47 Furthermore, several studies investigated the responsiveness of QuickDASH in patients with specific conditions including upper limb amputation and shoulder disorders, but no studies reported the validity, reliability, or responsiveness of K-QuickDASH.89
Carpal tunnel syndrome (CTS) is the most common neuropathic disease associated with the upper extremity.10 Patients' subjective symptom, which is represented by pain, is an important factor determining the surgical indication for CTS.11 Therefore, self-reporting questionnaires, which could objectify these subjective discomforts can be helpful to the clinician as well as patients in decision making process. Several previous reports have adopted DASH to evaluate post-operative assessment after carpal tunnel release (CTR). The significant correlations between DASH score and improvements in grip and pinch power and severity of pain have been reported.1213 QuickDASH has advantages compared to DASH that it is quick and easy to perform in clinics.14 However, sparse studies have tried to reveal the responsiveness of QuickDASH targeting diseases such as CTS in Korea. Therefore, in this study, we tried to clarify not only validity and reliability of K-QuickDASH but also the responsiveness of K-QuickDASH in patients with CTS.
METHODS
Subjects
This study was a retrospective cohort study which conducted using clinical records of a total of 83 subjects (8 males [9.6%] and 75 females [90.4%]) with CTS who visited the Department of Orthopedic Surgery, Seoul National University Bundang Hospital. Their mean age was 54.66 ± 9.67 years (age range, 30–79). The subjects underwent open CTR and fulfilled K-DASH and K-QuickDASH at two different time points (before and six months after surgery) between March 2014 and April 2017. All subjects underwent surgical treatment only on one side (46 right side [55.4%] and 37 left side [44.6%]) of their wrist. Subjects with neuromuscular disease, psychiatric disease, such as depression were excluded, and the subjects who did not complete 6-month follow-up were excluded as well. The validity and reliability of K-QuickDASH were analyzed using the preoperative questionnaire data and clinical records of all subjects.
Questionnaires
The K-DASH mainly consisted of a disability/symptom scale with 30 items and 2 optional modules including sports/performing arts module and work module with 4 items each. Disability/symptom scale of K-DASH consists of 21 items related to activities of daily living (ADL), 2 items associated with social activity, 5 items about symptoms, and 2 items related to sleep and self-image, respectively.1516 Based on the full-length K-DASH, the following 11 items that constituted the K-QuickDASH were extracted; 6 items related to ADL, 2 items associated with social activity, 2 items about symptoms, and one item related to sleep (Table 1). The K-QuickDASH also included two optional modules consisting of the same items as K-DASH; sports/performing arts module, and work module. Both modules were calculated in the same way in K-QuickDASH, and their validity and reliability were confirmed according to a previous cross-cultural adaptation study of K-DASH. Therefore, both additional modules were not included in the present study.4 Also, in the previous cross-cultural adaptation study, language adaptation process had already been implemented. Since the K-QuickDASH uses part of the K-DASH questionnaire items, the language adaptation process was not included in this study either.
Table 1
Comparison between the DASH questionnaire items and the QuickDASH questionnaire items

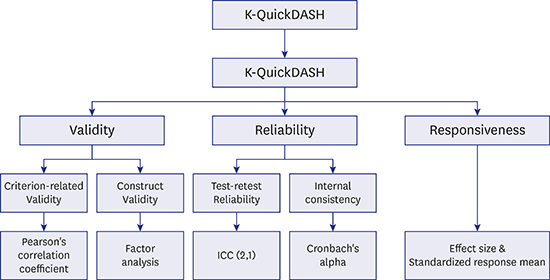
Validity
Both criterion-related validity and construct validity were assessed. The criterion-related validity was defined as the associations between specific questionnaires with other types of questionnaire or clinical outcomes. Concurrent validity, one of the subtypes of criterion-related validity, was estimated by comparing the results from questionnaire and clinical outcomes measured concurrently. The criterion-related validity was evaluated by comparing the results of K-QuickDASH and K-DASH. The relationships between K-QuickDASH and visual analog scale for pain (pain VAS), blend scale of nerve conduction study (NCS), grip power and pinch power were additionally analyzed. Based on K-DASH and K-QuickDASH scoring system, the total scores of K-DASH and K-QuickDASH decreased with improvement in subject status. In addition, as the clinical condition of the subjects improved, the pain would decrease and the degree of nerve abnormalities would be low. On the other hand, grip and pinch power would increase. Therefore, the existence of concurrent validity between two measured values suggests a positive correlation between K-DASH and K-QuickDASH, K-QuickDASH and pain VAS, and K-QuickDASH and blend scale. Conversely, K-QuickDASH exhibits a negative correlation with grip and pinch power. The Pearson's correlation coefficients were obtained between each of the relationships. Generally, the values ranging from ± 0.1 to ± 0.3 indicate small correlation, ± 0.3 to ± 0.5 indicate moderate correlation and ± 0.5 to ± 1.0 imply strong correlation.17
Construct validity was estimated by factor analysis. The generalized least square method was used for factor analysis extraction, and Varimax rotation was used for factor analysis rotation.18 Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Barlett's test of sphericity were conducted to determine our data fit for factor analysis. KMO values greater than 0.70 generally indicate the utility of factor analysis. Values less than 0.05 in Barlett's test, also indicate the utility of factor analysis. The communality indicates the proportion explained by the extracted factors. If the extraction of the items was less than 0.4, it was excluded from the factor analysis. Subsequently, the total variance explained of initial eigenvalues and rotation sums of squared loadings were calculated. Factors with an eigenvalue greater than 1 were extracted. The factor loadings of each of the 11 questionnaire items were calculated for each extracted factor. Questionnaire items with a factor loading in the rotated component matrix of 0.40 or greater were considered acceptable in the extracted factor.
Reliability
Internal consistency and test-retest reliability were assessed to demonstrate reliability of K-QuickDASH. The Cronbach's alpha coefficients were calculated among the items within each category (ADL, social activities, and symptom) and among all the questionnaire items to assess the internal consistency in all patients. Because the sleep category comprised only a single questionnaire item, it was not adequate for evaluation of internal consistency. In general, a score greater than 0.7 is usually acceptable.19
To obtain test-retest reliability, the intraclass correlation coefficient (ICC) using the 2-way random effects and absolute agreement with a single measurement model (ICC [2, 1]) of randomly selected 24 patients from all subjects were assessed.20 The ICC for each of the 11 questionnaire items and the ICC for the entire questionnaire items were verified. The interval between the first and the second interviews was 1 months. ICC values between 0.5 and 0.75 indicated moderate reliability, values between 0.75 and 0.9 indicated good reliability, and values greater than 0.9 suggested excellent reliability.20
Responsiveness
Responsiveness was assessed using the standardized response mean (SRM) and the effect size (ES). The SRM is defined as the mean change in the scores between baseline and follow-up, and this change is divided by the standard deviation (SD) of the individual changes in scores. The ES was defined similar to SRM, altering only the denominator to the SD of the baseline score. The larger value of SRM or ES indicated greater responsiveness. Values exceeding 0.8 would be interpreted as having higher levels of responsiveness. Responsiveness was analyzed using questionnaire data before and six months after operation.721
RESULTS
Validity
The Pearson's correlation coefficient between the K-QuickDASH and the K-DASH was 0.975 (P < 0.001) (Table 1) suggesting a robust correlation between K-QuickDASH and K-DASH. The relationships between the K-QuickDASH and the pain VAS (R = 0.365, P < 0.001), K-QuickDASH and Grip power (R = −0.309, P < 0.01), and K-QuickDASH and pinch power (R = −0.327, P < 0.01) showed moderate correlation with each other. By contrast, the blend scale of NCS was not related to K-QuickDASH (Table 2).
Table 2
Criterion-related validity between K-QuickDASH and K-DASH, Pain VAS, Blend scale of NCS, and grip power

Data obtained from correlation analysis using Pearson's correlation coefficient.
K-QuickDASH = Korean version of Quick Disabilities of the Arm, Shoulder, and Hand questionnaire, K-DASH = Korean version of Disabilities of the Arm, Shoulder, and Hand questionnaire, VAS = visual analog scale, NCS = nerve conduction study.
aP < 0.001, bP < 0.01 by Correlation analysis.
The generalized least square method with Varimax rotation method yielded three factors. The scree plot confirmed the choice of three factors (Fig. 1). The KMO measure of sampling adequacy was 0.837 and Bartlett's test of sphericity showed statistically significance (P < 0.001). The communality of all questionnaire items was greater than 0.4. The KMO measure, Bartlett's test and communality confirmed that all the questionnaire items and data in this study were suitable for factor analysis. The first factor included six questionnaires that correlated with activities of daily living. Two symptom-related questionnaire items and sleep related questionnaire item were included as the second factor. The third factor included two questionnaires items related to social activity (Table 3). Therefore, it was confirmed that questionnaire items of the K-QuickDASH were well organized, and the construct validity was verified.
Fig. 1
Scree plot of K-QuickDASH questionnaire items obtained by factor analysis.
K-QuickDASH = Korean version of Quick Disabilities of the Arm, Shoulder, and Hand questionnaire.
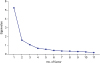
Table 3
Construct validity of K-QuickDASH using the generalized least square method
Reliability
The Cronbach's alpha of 11 K-QuickDASH questionnaire items was 0.89. The Cronbach's alpha values of three category (ADL, social activity, and symptom) were 0.89, 0.70, and 0.72, respectively. Each category showed an acceptable range of internal consistency. The ICC (2, 1) test for each of K-QuickDASH items ranged from 0.64 to 0.98 and was 0.83 for all the K-QuickDASH items (Table 4). All the ICC values revealed a greater than moderate degree of test-retest reliability.
Table 4
The Cronbach's alpha of total eleven items of K-QuickDASH and each subgroup (ADL, social activities, and symptom), ICC (2, 1) for each of K-QuickDASH items and total K-QuickDASH items
Responsiveness
The SRM of the K-DASH score was 1.00 and the ES was 0.91. The SRMs of the K-QuickDASH score were 0.99 and 1.1, respectively (Table 5). The K-DASH and K-QuickDASH exhibited a large degree of responsiveness.

DISCUSSION
QuickDASH is a questionnaire that is widely used for evaluation of severity of upper extremity musculoskeletal disorder.22 It can be used to quantify subjective discomfort, and therapeutic responses, especially in relation to the functional performance of the upper extremity, similar to the original version of DASH.22 QuickDASH has some limitations compared to DASH such as higher scoring tendency and lower specificity, considering the contents of the questionnaire.2223 However, QuickDASH still has values that it is quick and easy to complete the survey than DASH.24 Thus, many cross-cultural adaptation studies have been published for their cultural adaptation of QuickDASH so far, however, the reliability and validity of K-QuickDASH have not been proved.
Based on the aforementioned results, several significant points could be derived. Notably, the present study showed high levels of validity and reliability of K-QuickDASH in CTS patients. In order to evaluate the clinical utility of a specific questionnaire, it is essential to demonstrate its reliability and validity statistically. Evaluation of the validity of a questionnaire requires verification of the three types of validity including content, construct, and criterion-related validity.25 Content validity was already confirmed during the development of the questionnaire items. Therefore, we adopted criterion-related validity using Pearson correlation coefficient and construct validity based on factor analysis. Several cross-cultural adaptation studies investigating QuickDASH only adopted criterion-related validity. Therefore, the value of the present study is that it is the first study to adopt proper way of statistical analysis to reveal the construct validity of the QuickDASH.
The questionnaire items related to symptom and those to the sleep were classified as the same factors. The relationships between chronic pain and sleep disturbances have been reported in several previous studies. However, few studies tried to clarify the relationships between pain and sleep disturbance in CTS patients.2627 Furthermore, sleep disturbance may play a role in pain augmentation process, suggesting that hand surgeons should deliberate on patients' sleep quality.26
Aforementioned results showed the significant correlations between K-QuickDASH and the grip and pinch power, but correlation between K-QuickDASH and blend scale of NCS was not significant. Previous study has shown similar result. NCS was related with function of the nerve fibers with large diameters but the subjective symptoms including pain were associated with function of nerve fibers with small diameters.28 Therefore, K-QuickDASH which is self-reported evaluation tool for subjective discomfort and functional ability could not show significant correlation with bland scale of NCS.
This study demonstrated high levels of responsiveness to K-QuickDASH in CTS patients. The responsiveness of original DASH has reported in various disease entities including CTS and the responsiveness of QuickDASH also has been reported in certain diseases.8929 However, no study has determined the responsiveness of QuickDASH to CTS. The questionnaire format facilitated clinical assessment of patients by clinicians in a relatively short time with minimal effort prior to clinical evaluation and imaging. We confirmed that K-QuickDASH can be used as an evaluation tool for better understand the condition of patients with CTS through the high degree of responsiveness.
Patients with CTS mostly complained of sensory ailments including paresthesia. On the other hand, QuickDASH and DASH mainly consisted of items, which focus on the subjects' functional ability.2224 The present study demonstrated high levels of validity, reliability, and responsiveness in K-QuickDASH to CTS patients. The results suggest that sensory impairment and pain may correlate with functional disability. Previous studies suggested multiple sensory impairments may reduce the functional ability in patients with arthritis.30 Thus, reduced sensory function and pain would be associated with reduced functional ability involving upper extremities.
The present study had several shortcomings. Firstly, characteristics of cross-sectional retrospective study, this study could not provide correlation with additional surveys such as Boston Carpal Tunnel Questionnaire and Michigan Hand Outcome Questionnaire. Thus, there was a limitation to showing concurrent validity with other questionnaires, but we tried to overcome the limitations by providing the correlation with the other parameters which could reflect the patient's objective conditions such as grip power and NCS. Secondly, this study was conducted only in patients with CTS. Although CTS is one of the representative diseases of upper extremity, this study did not include various disease entities of the upper extremities and normal subjects and is considered an obvious limitation of this study. Thus, future prospective studies including K-QuickDASH in various disease entities of upper extremity and with several reference questionnaires would be needed to further elucidate its diagnostic value.
In conclusion, in the present study, the reliability, validity and responsiveness of K-QuickDASH were confirmed based on aforementioned results. Although the study was conducted only in subjects with a single disease entity, adequate meaningful results were derived via appropriate statistical analysis. Thus, the K-QuickDASH can be widely used as an evaluation tool for patients with CTS as a substitute for K-DASH.
 XML Download
XML Download