

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute pyelonephritis (APN) is the most common form of upper urinary tract infection (UTI), and approximately 20%–35% of women experience an episode of APN in their lifetime.1 APN usually occurs secondary to an ascending infection of gram-negative bacteria in women, and the diagnosis is made clinically.2 Incidences of nephrolithiasis related UTI have been on the rise.3
Enhanced computed tomography (ECT) is being widely used for diagnosis of APN.12456 ECT shows both the intrarenal and extrarenal areas as precise images and provides comprehensive anatomical information.7 It also enables the detection of complications such as renal or perinephric abscess.8 However, the administration of iodinated contrast agents used during ECT increases the risk of contrast-induced acute kidney injury (CIAKI).9 specially in patients with poor renal function.10 Patients with APN are more likely to have an acute kidney injury (AKI).11 Nonetheless, ECT is widely used as a primary tool in the ERs, and there is growing concern about the damage it can cause to the kidney.
Unenhanced computed tomography (UCT), on the other hand, avoids both CIAKI and delays in testing due to fasting and can detect nephrolithiasis; parenchymal involvement, such as strings; and other anatomical disorders. However, to our knowledge, no studies yet have investigated the usability of UCT as a diagnostic tool or compared it with ECT for evaluating APN. This study aims to assess the correlations between the clinical and biochemical parameters of APN diagnosed using UCT and ECT as well as compare the clinical outcomes following the use of these techniques. Further, we will the define clinical predictors to help identify patients who can be diagnosed with UCT alone. The principal purpose of this study will be to compare the clinical outcome between UCT and ECT in patients with APN.
METHODS
Study design and measurements
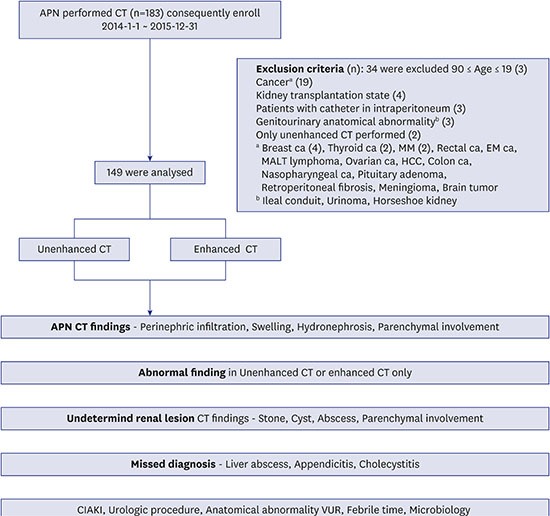
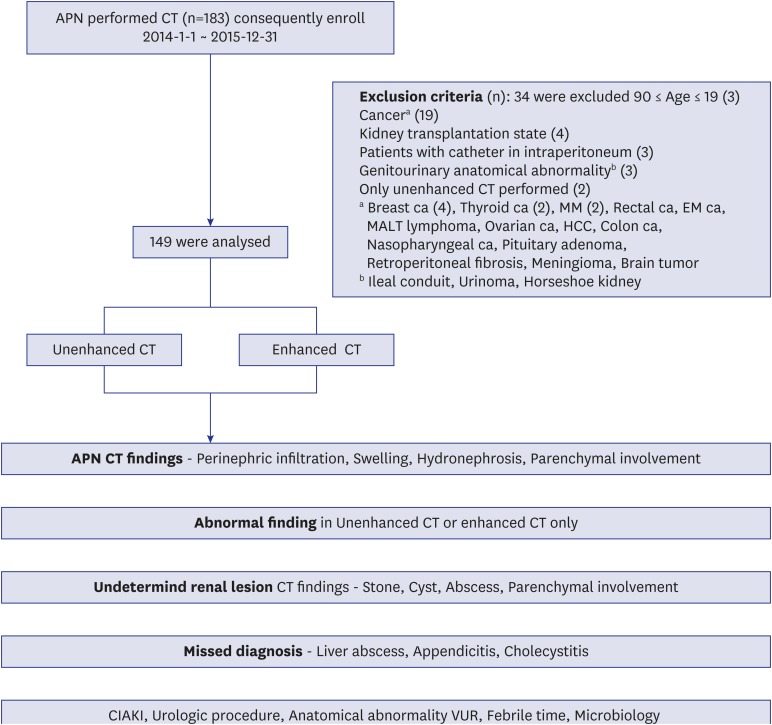
We conducted a retrospective review and analysis of the medical records of adult patients with clinically suggested APN who visited the ER at the Seoul National University Bundang Hospital and underwent both unenhanced- and enhanced-phase abdominal computed tomography (CT) scanning between January 2014 and December 2015. We excluded patients who had a history of cancer, kidney transplantation, intraperitoneal catheter implantation, and known genitourinary anatomical abnormalities (Fig. 1). We finally analyzed 149 patients. We collected demographic data and information on clinical parameters including sex, diabetes mellitus (DM), immunosuppressed state, recurrent urinary tract infection, neurogenic bladder, vesicoureteral reflux (VUR), and neurological diseases.121314
Fig. 1
Study algorithm.
APN = acute pyelonephritis, CT = computed tomography, MM = multiple myeloma, EM = endometrial, MALT = mucosa-associated lymphoid tissue, HCC = hepatocellular carcinoma, UCT = unenhanced computed tomography, ECT = enhanced computed tomography, CIAKI = contrast induced acute kidney injury, VUR = vesicoureteral reflux.
We conducted the following biochemical and laboratory analyses: urine analysis with microscopy, urine culture and antibiotic sensitivity, blood culture, serum creatinine level assessment before and within 2 days after CT, determined the duration of antibiotic therapy and afebrile time, and reviewed the patient data. We also evaluated undetermined lesions in case of UCT and risks for missed diagnosis and incidence of CIAKI.
Clinical diagnosis of APN was made in patients fulfilling more than three of the following four diagnostic criteria: 1) costovertebral angle tenderness with or without lower urinary tract symptoms, including dysuria, urinary frequency, urinary urgency, nocturia, suprapubic discomfort, and, occasionally, gross hematuria, 2) fever of more than 37.5°C, 3) leukocytosis in the complete blood count (> 10,000/μL), and 4) abnormal urine test results (pyuria: white blood cells [WBC] of > 10/high-power field [HPF] or positive urine culture of > 105 colony-forming U/mL).248
CIAKI was defined as a rise in serum creatinine (Cr) of ≥ 0.5 mg/dL (≥ 44 mmol/L) or a 25% increase from the baseline value, assessed at 48 hours after a radiological procedure according to the guidelines of the Kidney Disease Improving Global Outcomes 2012.
CT analysis
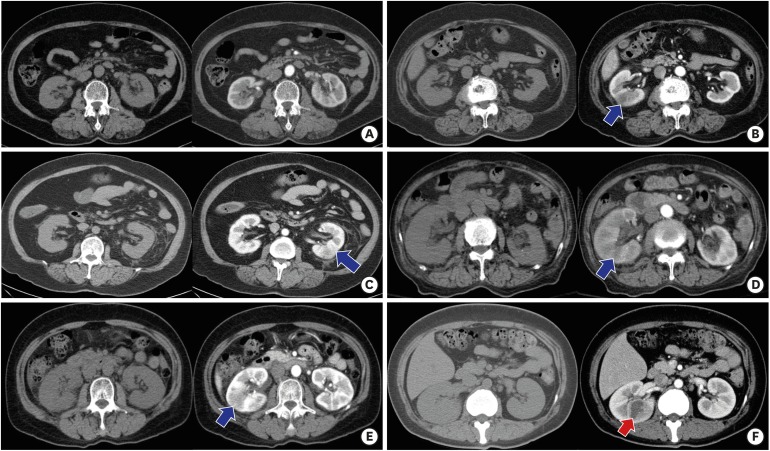
Two radiologists who were unaware of the clinical outcomes recorded and graded the parenchymal involvement, perinephric infiltration, kidney swelling, hydronephrosis, cysts, abscesses,15 and stones on both UCT and ECT.16 Parenchymal abnormalities appeared as hypoenhanced regions that were ill-defined wedge-shaped lesions of decreased attenuation and that radiated from the papilla in the medulla to the cortical surface after contrast injection.16171819 Infiltration of perinephric fat represents APN with infection and obstruction.17 CT findings were divided into 5 grades based on the renal parenchymal involvement in this study, as follows: no renal parenchyma involvement (grade 0), less than 25% involvement (grade 1), 25%–50% involvement (grade 2), 50%–75% involvement (grade 3), and greater than 75% (grade 4).19 Representative types of parenchymal involvement on ECT are shown in Fig. 2.
Fig. 2
Grade of parenchymal involvement. (A) grade 0: no renal parenchyma involvement, (B) grade 1: less than 25% involvement, (C) grade 2: 25%–50% involvement, (D) grade 3: 50%–75% involvement, (E) grade 4: greater than 75% involvement, and (F) Abcess. Left side present are UCT and right side present are ECT.
UCT = unenhanced computed tomography, ECT = enhanced computed tomography.
Statistical analysis
The baseline characteristics and laboratory data are presented as means and standard deviations for continuous variables and as frequencies and percentages for categorical variables. The accuracy of the two diagnostic tests performed simultaneously on an individual subject was compared using the McNemar test. A value of P < 0.05 was considered significant. All analyses were performed using the SPSS Statistics software ver.22 (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
A total of 149 patients were finally enrolled in the study. Comparison of the baseline characteristics between the ECT and UCT groups are shown in Table 1.
Table 1
Baseline characteristics
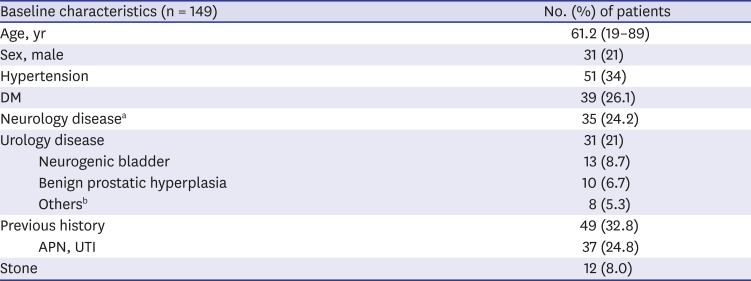
DM = diabetes mellitus, APN = acute pyelonephritis, UTI = urinary tract infection.
aCerebrovascular disease 15 (10), dementia 13 (8.7), Parkinson disease 4 (2.6), Alzheimer's disease 2 (1.3), cerebral palsy 1 (0.6); bOveractive bladder 3 (2.0), foley insertion state 3 (2.0), vesicoureteral reflux 2 (1.3).
Of the 149 patients, 118 (79%) were women. Their mean age was 61.2 (± 10) years. A quarter of the patients had a history of DM and a neurological disease. Previous histories of UTI and nephrolithiasis were found in 37 (25%) and 12 (8%) patients, respectively. The average of Cr is 0.94 mg/dL at the time of ER visit, The mean of Cr at discharge is 0.87 mg/dL. The results of the APN clinical diagnosis criteria presented in this study are as follows: 1) costovertebral angle tenderness, 132 (88%); 2) fever of more than 37.5°C, 129 (86%); 3) leukocytosis in the complete blood count (> 10,000/μL), 98 (65%); 4) pyuria, WBC of > 10/high-power, 131 (87%).
Representative CT-APN CT findings
Table 2 summarizes the number of patients with and without abnormal findings.
Table 2
Representative CT findings
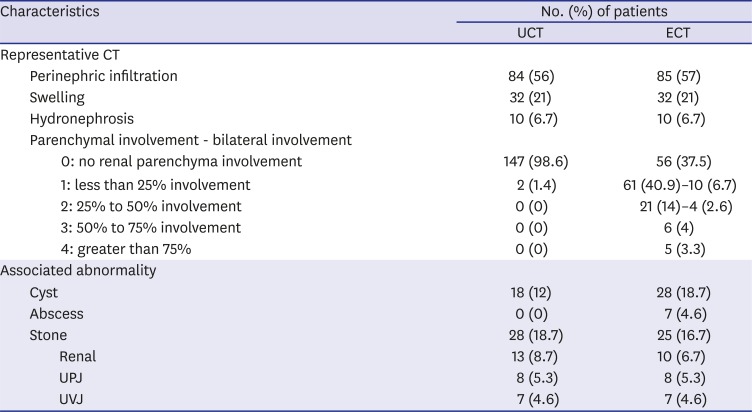
UCT detected abnormal findings in 99(66.4%) patients, which included stone (18.7%), perinephric infiltration (56%), swelling (21%), hydronephrosis (6.7%), and parenchymal involvement (1.4%). The remaining 50 (33.6%) patients had no abnormal findings in UCT. Seventeen patients (11.4%) had an atypical clinical course characterized by abdominal pain without costovertebral angle tenderness, sustained fever regardless of an antibiotics treatment and a sustained shock state, requiring additional tests to confirm the diagnosis by UCT. Of these 17 patients, 7 received a comparable diagnosis by both UCT and ECT, whereas the remaining 10 patients had a different diagnosis including renal abscess by ECT. Evaluation by ECT revealed abnormal findings in 112 (75.2%) of the 149 patients, while the remaining 34 (22.8%) had no abnormal findings. These findings included stone (16.7%), perinephric infiltration (57%), swelling (21%), hydronephrosis (6.7%), and parenchymal involvement (62.5%). Of the 93 patients with parenchymal involvement, 14 presented bilateral parenchymal involvement. There were some differences in the clinical manifestations between the unilateral and bilateral parenchymal involvement groups. Of the 14 patients with bilateral parenchymal involvement, 21.4% were men, 28.5% had DM, 21.4% had shock (systolic blood pressure < 90 mmHg), 71.4% had bacteriuria, and 35.7% had bacteremia. APN CT findings were comparable with regards to stone, perinephric infiltration, swelling and hydronephrosis on both UCT and ECT. In 12 patients (8.0%) ECT detected only a low grade (1 and 2) parenchymal involvement and no perinephric infiltration or other complications such as stone or abscess. These cases were diagnosed as simple APN and had a good prognosis.
Representative CT-stone, cyst, abscess
Table 2 summarizes the number of patients with stones, cysts, and/or abscesses.
While UCT detected various levels of stones in 28 (18.7%) patients, ECT detected the same in 25 (16.7%) patients. The stones were detected in the following anatomical locations: renal (8.7%), ureteropelvic junction (UPJ) (5.3%), and ureterovesical junction (UVJ) (4.6%). Although UCT detected more stones in the renal part, both CTs detected a comparable number of stones in the UPJ and UVJ, thereby suggesting that UCT is overall better than ECT in diagnosing stones.
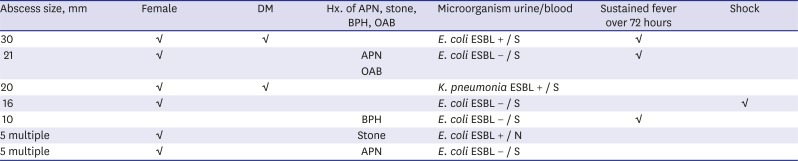
UCT detected renal cysts of multiple sizes in 18 (12%) of the patients, whereas ECT did the same in 28 (18%) patients. A renal abscess was detected in 7 (4.6%) patients with ECT (Table 3). Four of the 149 patients continued having fever 72 hours after starting antibiotics. Three of these 4 patients showed renal abscess by ECT, which was not seen by UCT. The other 3 patients of 7 patients with renal abscess tested positive for extended-spectrum beta-lactamases (ESBL) and had a recurrence of APN respectively.
Table 3
Renal abscess
Missed diagnosis
UCT missed the diagnosis of cholecystitis, liver abscess, and appendicitis, in three men who were then diagnosed with ECT. The patient with cholecystitis had a delayed laparoscopic cholecystectomy following percutaneous transhepatic gallbladder drainage. The patient with appendicitis underwent a percutaneous abscess drainage on the perforated peripheral abscess. The third patient with the liver abscess, who was identified by aspiration and Klebsiella pneumoniae ESBL testing, improved after 6 weeks of antibiotics use. In all of these three cases, there was no imaging evidence for APN and therefore the treatment was completely different from that for APN.
CIAKI
Six patients were diagnosed with CIAKI within 2 days after ECT. CIAKI occurred despite hydration before ECT, but with supportive care, it improved by the time of discharge in all 6 cases. The incidence of CIAKI was related to age and DM in this study. The 6 patients were 89, 82, 80, 48, 42, and 33 years old (mean: 62.3 years). Three of these 6 patients have DM and were women.
Microorganisms
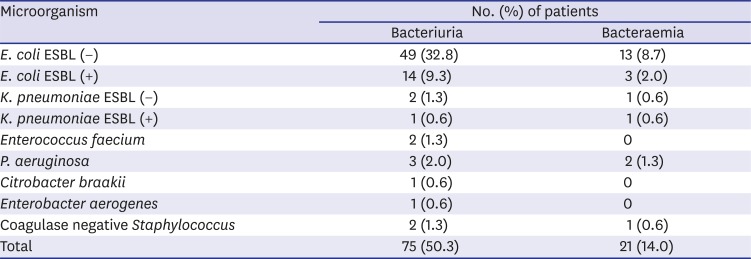
Comparison of identification strains between the urine culture and blood culture groups are shown in Table 4. Blood cultures tested positive in 21 (14%) patients, with Escherichia coli being the most common causative organism (n = 16; 10.7%) followed by K. pneumoniae and Pseudmonas aeruginosa. Only three patients had bacteremia caused by ESBL-producing E coli. Bacteriuria was seen in 75 (50.3%) patients, and E. coli was the most common causative organism, followed by K. pneumoniae and P. aeruginosa. All 7 patients with renal abscess had bacteriuria, and all 11 patients with more than 50% parenchymal involvement had bacteriuria.
Table 4
Results of blood and urine culture
DISCUSSION
APN is a clinical diagnosis, and recent studies have emphasized the importance of early imaging in patients with APN for cost-effective management.16202122 No studies to date have reported the use of UCT as a diagnostic tool for APN or compared it to other imaging techniques especially, ECT. So, we investigated the clinical usefulness of UCT for evaluating upper urinary tract infections and compared it to the ECT.
Recently, perirenal fat infiltration has been considered as important as parenchymal involvement for the diagnosis of APN by UCT.22 Perirenal fat infiltration is observed when the inflammation of the renal parenchyma spreads beyond the renal capsule into the perirenal fat.7 The stranding likely represents fluid that collects within the bridging septa of the perinephric fat as a result of increased lymphatic pressure. Fluid collections may become asymmetric in the presence of unilateral obstruction or pyelonephritis.22
In this study, UCT was able to detect major APN findings. Whereas UCT detected perinephric infiltration for diagnosis of APN in 84 (56%) patients, ECT detected the same in 85 (57%) patients. A longer duration of fever, higher C-reactive protein levels, and grade of pyuria were related with perirenal fat infiltration,7 suggesting that the diagnostic accuracy of perinephric fat infiltration with UCT is almost identical to that with ECT for patients with APN. UCT may, therefore, be a good initial tool for assessing typical cases with low to moderate risk APN, with the advantage of avoiding CIAKI. Based on our findings we consider the following as risk factors for APN: being a woman (79%), DM (26.1%), previous recurrent APN/UTI (24.8%), neurogenic bladder (8.7%), and previous history of stone (8%). These factors are also risk factors for obstructive nephropathy. As a result of this study, perinephric infiltration was the most relevant finding in UCT for the diagnosis of APN. It is thought that perinephric infiltration is not inferior to parenchymal involvement for the diagnosis of APN. Although parenchymal involvement was absent from ECT, non-contrast CT showed 8 cases with perinephric infiltration. Four cases were secondary due to stone, and 4 cases were APN.
Six (4%) patients were diagnosed with CIAKI within 2 days after ECT. Potential benefits and disadvantages of administering contrast and its impact on patient management should be evaluated by physicians based on the complete clinical history. Customized CT examinations can be performed, to improve the diagnostic accuracy. Patients who get only the UCT due to fear of CIAKI, should keep undetermined lesions and missed diagnosis in mind. This study reveals that the high-risk group of patients with renal abscesses and missed diagnosis predominantly included men with DM, recurrence of APN, urologic disorders, and identification of a pathogenic strain in the urine culture.
In patients who did not show any APN findings by UCT, ECT detected parenchymal involvement in. Thirty-four patients with no abnormalities by ECT were treated for simple UTI with oral antibiotics. Sixteen patients who had only parenchymal involvement in ECT continued with the same treatment for APN.
Undetermined lesions visible only with contrast and not visible by UCT included renal abscesses in 7 (4.6%), cysts in 10 (1.4%) and missed diagnosis in 3 cases. These patients underwent additional procedures and different treatments. ECT can detect a renal abscess or other combined intra-abdominal infections. It is not the initial procedure for diagnosis but is used for confirmative imaging. ECT is recommended for patients with high-risk factors mentioned above and for the differential diagnosis of undetermined lesions such as renal abscesses.
Although no abnormalities found in ECT, UCT were detected stones. Stones were well detected in 28 (18.7%) and 25 (16.7%) patients, with UCT and ECT, respectively. In 3 cases, stones were visible only with UCT, all of which were renal stones. This suggests that a renal stone can be missed with ECT alone. Eleven of the 28 patients with stones were treated with urologic procedures. During the analysis, two patients were found to have VUR.
In typical APN patients, the rate of treatment using empirical antibiotics is very high.13 Patients who have unusually severe symptoms and do not respond to antibiotic therapy within 72 hours.2324252627 need ECT despite the side effects of radiation defining the extent of the disease.282930 This study recommends the use of UCT first, and then ECT to detect any missed diagnosis only if the patient belongs to the high-risk group has a persistent fever after 72 hours of antibiotic use and shows no improvement in the symptoms. This two-step CT strategy may prove useful and cost-effective in diagnosing patients with typical low to moderate risk APN.
The limitations of this study are as follows: 1) clinical and laboratory parameters were used as the standard of reference to evaluate APN, 2) we could not identify the sensitivity of the different modalities to diagnosis, and 3) data from patients who were discharged from the ER with no follow-up could not be analyzed. Further studies are needed for prospective and other population settings for suggesting diagnostic guidelines for APN with UCT.
This study is the first one to evaluate the usefulness, efficacy, and validity of UCT as a diagnostic tool for APN. Our findings suggest that UCT is not inferior to ECT as an initial tool for evaluating typical APN patients with low to moderate risk as well as patients with an atypical clinical course, in which additional tests are required for accurate diagnosis.
 XML Download
XML Download