

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Falls are a major cause of injury in all ages,1 and account for 10% to 15% of emergency department (ED) visits. Generally, falls from higher heights cause more severe injuries.23 In the elderly population, however, even falls due to low-energy mechanisms are associated with higher hospitalization rates, longer lengths of hospital stays, and higher rates of mortality compared with younger adults.456 By 2000, the Republic of Korea had become an aging society, with the elderly population increasing at the fastest rate in the world. According to the Korean Statistical Information Service (KOSIS), elderly people aged 65 or older will account for 14% of the Korean population in 2017 and 20% of the population by 2025. As the elderly population increases, the burden of geriatric diseases is also increasing within the community. In particular, fall injuries in the elderly population will be a major social issue,5 and lead to increased health care costs.7
The most effective means of reducing the incidence of any injury is prevention. Identifying characteristics and relating factors to severe fall injuries in the elderly population is necessary to select management targets and establish a prevention strategy.8 There have been many studies on injuries associated with low-velocity falls (LVF) or ground-level falls (GLF) in the elderly population59; however, studies on the characteristics and relating factors to severe injuries caused by low-height falls (LHF) are lacking.
This study was conducted to compare the characteristics of injuries from LHF and to identify relating factors to severe injuries in the elderly population.
METHODS
With support from the Korea Center for Disease Control and Prevention (KCDC), we retrospectively reviewed surveillance data on injured patients who presented to the EDs of six general hospitals from January 2011 to December 2015. LHF were defined as falls from a height of less than one meter.210 Only data from patients who were able to report the height of the fall were included in this study. All patients were 65 years of age or older and were divided into 2 groups based on severity of injury: severe group and non-severe group. The severe group included patients who required emergency surgery, were admitted to the intensive care unit (ICU), were transferred to another medical facility for specialized care, or were either pronounced dead on arrival or death at the ED. The remaining patients were placed in the non-severe group.2
First, the general and clinical characteristics of the severe group were compared with those of the non-severe group. General characteristics of the patients included age, age range (65–74, 75–84, and ≥ 85 years), season of injury occurrence, time of injury occurrence, location of injury occurrence, whether the injury happened indoors or outdoors, specific description of the indoor area, activities during injury occurrence, alcohol consumption, education level, and occupation status. Patients were also sorted into groups based on the season in which the injury occurred: spring (March–May), summer (June–August), autumn (September–November), and winter (December–February). The time of injury occurrence was divided into 6-hour intervals: 0:00 to 6:00, 6:00 to 12:00, 12:00 to 18:00, and 18:00 to 24:00. The location where the injury occurred was classified as a residential facility, medical facility, sports facility, transportation area, work place, public or commercial facility, or other outdoor area. The location of an indoor injury was subdivided into the kitchen, living room, room or bedroom, store (including a mall) or office, hospital room, or other area. Activities during injury occurrence were divided into paid work, unpaid work such as cooking and cleaning, sports or leisure, daily activities such as showering, bathing and shaving, and other activities. Education level was divided into elementary school or less, junior high school, high school, and college or higher. Occupation status was classified as employed and unemployed.
The clinical characteristics of the patients while they were in the ED included blood pressure, consciousness, mode of transportation to the ED, major injury region, excess mortality ratio-adjusted injury severity score (EMR-ISS), result of ED treatment, surgical treatment, and injury severity. Consciousness was classified simply as alert or non-alert. Mode of transportation to the ED was classified as public ambulance, transfer from another medical facility, and individual transportation. Major injury regions were divided into head and neck, thorax, abdomen, hip and thigh, and other extremity. The EMR-ISS is an injury severity scoring systems based on the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Every injury registered in the ICD-10 code was graded on a scale of 1–5 using the calculated excess mortality ratio for all ICD-10 codes from the Korean national injury database. EMS-ISS was calculated as the sum of squares of three maximum severity grades.111213 If several diagnoses were registered, only the main diagnosis was selected. Results of ED treatment were categorized as discharge from ED, transfer to another medical facility, admission to the general ward, admission to the ICU, or dead on arrival or death at the ED.
In addition, the gender specific subgroup analysis was performed to determine the different characteristics between men and women in injuries from LHF.
Statistical analysis
The χ2 test, t-test, and Fisher's exact test were used to compare the severe versus non-severe group. Univariate logistic regression analysis was used using the significant variables (P < 0.2) from the univariate comparison analysis to identify factors related with severe injury in the elderly group. Multivariate logistic regression was performed using statistically significant variables (P < 0.05) from the univariate logistic regression. We excluded clinical variables that directly related to severe injury classification, such as the mode of transportation to the ED, the result of ED treatment and surgical treatment. The gender specific subgroup analysis was compared using the χ2 test. All data were analyzed using the Statistical Package for the Social Sciences version 21.0 (IBM Inc., Somers, NY, USA), and P values < 0.05 were considered significant.
RESULTS
During the study period, 1,190 patients were injured by LHF in the elderly population. The severe group consisted of 82 patients, accounting for approximately 7% of all patients. The mean age was 77 years in the non-severe group and 75 years in the severe group. Patients aged 65–74 years and 75–84 years had similar injury rates in the non-severe group; in the severe group, the most common age ranged was 65–74 years (56.5%). In both groups, the most common location of injury occurrence was a residential facility. However, the proportion of elsewhere except the residential facility was 35% higher in the severe group than 23% in the non-severe group. In the non-severe group, 85% of the patients were injured indoor and 72% in severe group; thus, LHF injuries that occurred outdoors were more likely to be classified as severe. The most common activity during which LHF injuries occurred was daily activities (77%), followed by unpaid work (8%) in the non-severe group, but daily activities (70%), and followed by paid work (15%) in the severe group. Alcohol consumption at the time of the injury was more frequent in the severe group (Table 1).
Table 1
General characteristics of LHF injuries in elderly patients based on the severity of injury

In the severe group, the fewer patients presented with alert consciousness at the ED than in the non-severe group. The most common mode of transportation to the ED was public ambulance (40%) in the non-severe group, and transfer from another medical facility (44%) in the severe group. As region of major injury, 35% of patients in the non-severe group and 71% in the severe group suffered injuries of the head and neck. After analyzing the results of ED treatment, most patients in the non-severe group (58%) were discharged from the ED and most patients in the severe group (70%) were admitted to the ICU. The patients who underwent surgery comprised 39% of the severe group compared with 7% of the non-severe group (Table 2).
Table 2
Clinical characteristics of LHF injuries in elderly patients based on the severity of injury
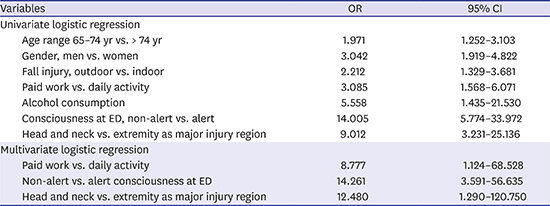
Results of the univariate logistic regression analysis demonstrated that severe injuries caused by LHF in the elderly population were more likely to occur in those aged 65–74 years compared with those aged more than 74 years. Other factors related with severe injuries were men vs. women, outdoor fall vs. indoor fall, paid work activity vs. daily activity, alcohol consumption, non-alert vs. alert consciousness at the ED, and head and neck vs. extremity as the major injury region. Based on the multivariate logistic regression analysis, elderly people injured by LHF were at greater relation of severe injuries if patients were injured during paid work, presented with non-alert consciousness at the ED, or if the major injury involved the head and neck (Table 3).
Table 3
Univariate and multivariate logistic regression analysis for relating factors to severe injury by a LHF in elderly patients

In the gender specific subgroup analysis, men comprised 36% and women 64% in the elderly population. The most common time of injury occurrence was between 12:00 to 18:00 in men and between 06:00 to 12:00 in women. In both groups, the most common locations of injury were residential facilities, respectively 67.0% and 80.8%. The most patients were injured indoors; this was more in women (90%). Especially, LHF injuries occurred most commonly in a room or bedroom. In both groups, the most common activity was daily activity, but the second most common activity was paid work (12%) in men. In men, more patients were educated and employed than in women (Table 4). The most common major injury regions were head and neck followed by extremity in men and head and neck followed by hip and thigh in women. Severe injuries were more common in men compared with those in women (Table 5).
Table 4
General characteristics of LHF injuries in elderly men and women

Table 5
Clinical characteristics of LHF injuries in elderly men and women
DISCUSSION
The mean age of elderly patients injured by LHF in this study was 77 years; this is 7 years older than the age 70 that predicted GLF mortality in previous studies. Age alone is considered to be a risk factor for severe injury and poor prognosis after a fall regardless of the mechanism.314 Careful attentions should therefore be paid to elderly patients presenting to the ED with fall injuries.
In the elderly population, LHF injuries occurred most commonly in residential and medical facilities. The most frequent indoor area where elderly patients fell was a room or bedroom followed by the living room; LHF injuries also occurred mainly during daily activities. A previous study showed a similar result, in that most fall injuries in the elderly population occurred at home during daily activities such as bathing, sleeping, and eating.15 Therefore, in this population, safety precautions should be taken, including the installation of low-height beds and bed railings, not standing on furniture above the ground, and caution in slippery areas such as bathtubs or toilets. Warning labels should also emphasize that elderly people are more at risk of falling from equipment such as scaffolding or ladders. Also, the medical staff and family members of elderly patients in long-term care facilities should strive to prevent fall injuries. Several studies have reported that training in the form of pamphlets, e-books, and electronic applications for elderly patients and their caregivers can reduce the incidence of fall injuries; therefore, more education through these methods is needed.1617
In addition, Helling et al.18 showed that many elderly patients suffered severe injuries after falls from heights less than 6 meter, even when their vital signs were initially stable. Therefore, the elderly patients should be considered at risk for severe injury, even though who presented to the ED with injury by mechanism of a LHF. It is also preferable to transport elderly patients directly from the scene of an accident to the regional trauma center to avoid aggravating the patient's condition. A trauma team should then promptly and carefully evaluate an elderly patient upon arrival to the ED.
Rau et al.10 reported that the most common injury regions caused by falls were extremities at all adult ages, including the hip and pelvis, regardless of the height of the fall. In particular, extremity injuries were significantly more common in elderly patients, and head and neck injuries were the second most common in both groups. In this study, the most common injury regions were head and neck followed by hip and thigh, in the elderly population. These results demonstrate that the injury characteristics of LHF are different from those of falls in general. In the elderly population, head and neck injuries were the most common in both the severe and non-severe groups; however, head and neck injuries were more than twice as common in the severe group compared with the non-severe group. This suggests that the higher rate of non-alert consciousness in the severe group is mostly likely due to serious injuries of the head and neck. Results from the multivariate logistic regression show that head and neck injuries and non-alert consciousness were both relating factors to severe injury in the elderly population; thus, ED medical staff should be especially vigilant in evaluating these patients.
In this study, there are more woman patients (64%) in the elderly population. This is consistent with results from previous studies showing that elderly women are more frequently injured by falls and more likely to present with a fall injury to the ED.101920
Recently, Gelbard et al.9 reported that men account for about half of all elderly patients with fall injuries, and Con et al.8 reported that elderly men are much more likely to fall in special situations (e.g., from a ladder) related to income activities or outdoor activities than their woman counterparts. It has also been reported that severe fall injuries in the elderly population are more common in men than women.1421 Consistent with these findings, we found that the elderly men were more likely to suffer an injury from LHF than the women elderly, especially in the severe group. Furthermore, injuries that occurred outdoors were more likely to fall into the severe group than the non-severe group. In addition, the average age of patients in the severe group was 2 years younger than the average age in the non-severe group, and more than half of the patients in the severe group were in the 65–74 years age range. This suggests that relatively young, healthy, and active elderly men who participated in income activities or outdoor activities,192223 were more likely to present to the ED with severe injuries after a fall.24
This study is limited due to its retrospective design. This is not a population-based study, and the data were limited to EDs from 6 general hospitals. There are also limitations due to coding inconsistency, which is common in large multi-institutional registries. Because 5 out of 6 of the hospitals included in this study were tertiary hospitals, there may have been a higher proportion of severely injured patients. It is also possible that the severe injury group may have been underestimated in this study if the patients or guardians refused further treatment due to the patient's age. The severity of fall injuries in the elderly population may vary depending upon comorbidities,1425 use of anti-coagulants,26 and the level of performance ability; however, these factors were not taken into account in this study. In both the non-severe group and the severe group, the value of variable consciousness at the ED was missing by more than 50% of the data. The missing values were presumed mostly to be alert, however the data were not manipulated for more objective results. In the future, these problems can be complemented by improvement activities of data quality. Finally, it is a meaningful result that paid work was the relating factor to severe injury, because income activities of the elderly population will be increased with an extend life expectancy. Further studies should be conducted focusing on occupation injury or physical activity in the elderly population.
Severe injuries can be occurred in about 7% of the total injuries caused by falls from even low-height in the elderly population. The relating factors to severe injuries were paid work, non-alert consciousness at the ED and major injury to head and neck.
 XML Download
XML Download