

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The global prevalence of osteoporosis is rapidly increasing, and it has become one of the most crucial socioeconomic burdens worldwide.1 In Korea, the population of adults over 65 years old rose from 3.3 million in 2002 to 5.2 million in 2012. The percentage of the elderly population is expected to reach approximately 20% of the total population by 2026.2 Since Korea is rapidly becoming a super-aging society, the socioeconomic burden associated with osteoporosis and its related fractures will increase rapidly and become a major component of the public health burden. Thus, an interest in this issue at the national level is required to adequately deal with this concern.
Presently in Korea, the standard criterion for defining and diagnosing osteoporosis is based on a T-score of ≤ −2.5 from a bone mineral density (BMD) test of the lumbar spine, femur, neck, or total hip.3 This operational definition of osteoporosis by the World Health Organization (WHO) is useful for comparing country-specific prevalence.45 The reported prevalence of osteoporosis in Caucasian women older than 50 years of age varies from 7.9% to 22.6% depending on the study population and design.678 Asian women were reported to have lower bone mass than Caucasians even after the differences between the body sizes of Caucasian and Asian women were considered.9 The prevalence of osteoporosis from a nationwide, cross-sectional health survey conducted in Korea was reported to be 7.5% in men and 35.5% in women in their 50s, higher than in Caucasians.10
However, prevalence based on BMD does not seem to represent the actual burden of osteoporosis in the country. Osteoporosis is a common disease, but due to its few related symptoms, it often goes unnoticed until a fragility fracture occurs. Therefore, it is difficult to assess the actual burden of osteoporosis. However, to know the actual burden of osteoporosis, it is necessary to know the number of patients who seek medical treatment. There are few reliable published reports on the utilization of medical services for osteoporosis in the general population. In Korea, Choi et al.10 estimated the diagnosis and treatment rate at 29.9% and 14.4% respectively, in women aged ≥ 50 years with osteoporosis, using data from a nationwide survey. Since the questionnaire survey in the previous study was conducted to determine the treatment status, we wanted to investigate the actual drug prescription and health service utilization using claim data. The present study was performed to assess the annual trend of utilization of osteoporosis-related health services and treatment status through operational definition, using data from the National Health Insurance Service (NHIS) nationwide database between 2008 and 2012.
METHODS
Database and study subjects
Participants aged over 50 years were identified from the Korean National Health Insurance Service (KNHIS) nationwide database between 2008 and 2012. The KNHIS covers 100% of the population including 97% on health insurance and 3% on medical aid. All clinics and hospitals submit data on inpatients and outpatients, including data on diagnoses (defined by the International Classification of Diseases, 10th revision [ICD-10]), demographic information, and medical costs for claims. Therefore, virtually all information about patients and diseases is available from the KNHIS, and this has been used in several epidemiological studies.111213 The pattern of utilization of osteoporosis-related health services was analyzed. This data included just the performance of the physician under the health insurance. Therefore, patients who received non-insured osteoporosis-related services were not included in this study. The age and sex distributions of the entire Korean population over the study period were obtained from the census data of the Korean National Statistics Bureau.
Operational definition of osteoporosis patients who accessed medical services
Eligible participants of the study were expected to fall within at least one of the following six criteria: 1) prescription of medications exclusively for osteoporosis treatment (bisphosphonate, selective estrogen receptor modifier, calcitonin); 2) ICD diagnostic code for osteoporosis (ICD-10 codes M80–M82) and prescription of medications related to osteoporosis (additionally indicated for other indications; hormones, calcium, and vitamin D); 3) elderly patients (males: ≥ 70 years, females: ≥ 65 years) with an ICD diagnostic code for osteoporosis; 4) past history of prescribed medications causing osteoporosis with an ICD diagnostic code (Supplementary Table 1); 5) past history of a disease that causes osteoporosis with an ICD diagnostic code of osteoporosis (Supplementary Table 2); 6) osteoporosis-related fracture (spine M48.4, M48.5, S22.0, S22.1, S32.0; humerus S42.2, S42.3; distal radius S52.5, S52.6; hip S72.0, S72.1). Each fracture code had to be accompanied by a physician's claim for site-specific fracture reduction or fixation (either open or closed) to enhance the specificity of the coding. In order to identify the osteoporosis patients who accessed medical services, we used a previously developed algorithm employing the above six criteria included in health insurance claim data (Fig. 1).14
Fig. 1
Patient identification algorithm using National Health Insurance claims data.
ICD-10 = International Classification of Diseases, 10th revision.

Newly diagnosed patients with osteoporosis were defined if all of the following criteria were met within 1 year prior to the first visit to the clinics: 1) no drug prescription history with osteoporosis; 2) no prescription history of the therapeutic agent with indications other than osteoporosis; and 3) less than 2 visits to clinics with osteoporosis or osteoporotic fracture-related diagnostic code.
To compute the proportion, the total number of patients with osteoporosis was divided by the total population; this ratio was calculated for each age group. The ratio for the number of patients newly diagnosed with osteoporosis was calculated the same way. Total population data were extracted from the resident registration demographics of the Ministry of Public Administration and Security.
Health service utilization rate and treatment rate
To assume the total number of osteoporosis patients, we used previous reports from the Korean National Health and Nutrition Examination Survey (KNHANES) 2008–2010. The KNHANES is a nationwide cross-sectional survey that has been periodically conducted since 1998 by the Center for Disease Control of the Ministry of Health and Welfare. The contents of the fourth survey consisted of a health, nutrition, and medical examination; the BMD examination has been included in the items of medical examination. Diagnosis of osteoporosis was made using the WHO T-score criteria (T-score ≤ −2.5 at lumbar spine, femur neck, or total femur). The prevalence of osteoporosis based on BMD was reported as 19.3%, 23.1%, and 21.8% of the population of adults, aged 50 or older, in 2008, 2009, and 2010, respectively.15 We estimated the total number of osteoporosis patients over the age of 50, using the prevalence rates of the estimated population from 2008, 2009, and 2010 by the Korean National Statistics Bureau. The health service utilization rate was determined as the number of osteoporosis patients in the present study divided by the total number of people estimated to have BMD based osteoporosis. Drug treatment rate was calculated by dividing the number of subjects who received exclusive medications for osteoporosis treatment (bisphosphonate, selective estrogen receptor modifier, calcitonin) by the estimated total osteoporosis population.
RESULTS
Number of osteoporosis patients using medical services
Between the 2008 and 2012, the number of osteoporosis patients over 50 years who accessed medical services increased by 33.2% (from 1.47 to 1.96 million). The increase in the number of male osteoporosis patients was higher than that of the females (44.4% vs. 31.9%). The number of osteoporosis patients who accessed a medical service increased by 7.4% each year (Table 1). The proportion of osteoporosis patients increased from 1,138/100,000 in 2008 to 1,255/100,000 in 2012, and the gender specific proportion increased by 18.1% in men and 10.5% in women.
Table 1
The number and proportion of osteoporosis patients (age ≥ 50 years) who used medical services in each calendar year

The pattern of utilization of osteoporosis-related health service was different depending on age and sex. For women, the proportion of osteoporosis patients who accessed medical services increased steadily in those 50 years of age and older, being highest in the 70–79 age group with a sharp decrease in those over 80. For men, the proportion was highest in the 80–89 age group and decreased slightly after 90 (Fig. 2).
Proportion of patients according to each definition
In 2012, the greater component of medical services accessed by osteoporosis patients was treatment with medications indicated only for osteoporosis (52.0%), followed by the prescription of medications related to osteoporosis plus a diagnostic code (26.2%). Of our patients, 8.3% had a past history of medication or disease related to secondary osteoporosis, and 6.4% had osteoporosis-related fracture (Fig. 3).
Fig. 3
Distribution of osteoporosis patients by category (2012). (A) Prescription of exclusive osteoporosis medications; (B) ICD-10 codes M80–M82 and prescription of medications related to osteoporosis; (C) elderly patients (males: ≥ 70 years, females: ≥ 65 years) with ICD-10 codes M80–M82; (D) past history of prescriptions causing osteoporosis with ICD-10 codes M80–M82; (E) past history of a disease that causes osteoporosis with ICD-10 codes M80–M82; and (F) osteoporosis-related fracture.
ICD-10 = International Classification of Diseases, 10th revision.
Number of newly diagnosed osteoporosis patients
During the study period, the number of newly diagnosed osteoporosis patients increased by 4.3% in women (from 601,147 to 648,311) and 20.4% in men (from 99,122 to 124,576) (Table 2). The number of newly diagnosed osteoporosis patients increased by 2.5% each year. In men, it increased by 5.9% each year, more than twice of that of women (Table 2). The rate of new diagnoses decreased from 541/10,000 in 2008 to 494/10,000 in 2012. However, in men, the rate of new diagnoses increased by 0.7% each year. The proportion of newly diagnosed osteoporosis patients who accessed medical services was 47.5%, 42.0%, 39.4%, 37.4%, and 39.4% from 2008 to 2012, respectively. The gender-specific proportion of new patients was 68.0%, 58.4%, 55.7%, 54.5%, and 59.2% for men and 45.3%, 40.0%, 37.4%, 35.3%, and 37.0% for women from 2008 to 2012, respectively. According to age distribution, the percentage of newly diagnosed patients was highest in the 50–59 age group (49.8%) and then 70–79 age group (47.7%) in 2012. The new diagnostic rate increased steeply with age in both men and women (Fig. 4).
Table 2
The number and proportion of newly diagnosed osteoporosis patients (age ≥ 50 years)

Health service utilization and drug treatment rate
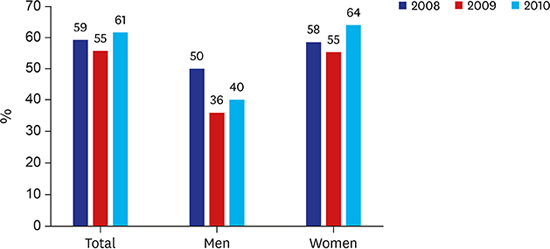
To determine the proportion of osteoporosis patients who accessed medical services, we estimated the total osteoporosis population based on prevalence data of BMD-based osteoporosis from the KNHANES during 2008 to 2010. The prevalence of osteoporosis was 19.3%, 23.1%, and 21.8% of the population aged 50 or older in 2008, 2009, and 2010, respectively. When we extrapolated it to the 2008, 2009, and 2010 population (National Statistical Office data), the estimated osteoporosis population was 2.53, 3.17, and 3.12 million, respectively. According to the present study, the number of osteoporosis patients who accessed medical services in 2008, 2009, and 2010 was 1.5, 1.7, and 1.9 million respectively. Less than 60% of patients with osteoporosis were estimated to access medical services due to osteoporosis (Fig. 5).

In addition, the number of people who received prescription of medications exclusive for osteoporosis treatment in 2008, 2009, and 2010 was 852,415, 976,670, and 1,042,595, respectively. The drug treatment rate in 2008, 2009, and 2010 was 34.1%, 31.1%, and 33.5%, respectively. In relation to gender, drug treatment rate in women was about twice that of men (Table 3).
Table 3
Treatment rate of Korean osteoporosis patients (age ≥ 50 years)

DISCUSSION
We used data from the medical and pharmacy claims of a large, nationwide cohort to assess trends in the utilization of medical services among osteoporosis patents. From the study, it was observed that Korea had recorded a continuous increase in the number of osteoporosis patients over 50 years. The total number of female patients was more than 8 times that of men. However, the rate of increase in men was higher than that of women. In this context, the proportion of newly diagnosed osteoporosis patients tended to decrease every year in women but increased in men. This indicates that, even though women are considered more prone to osteoporosis, its incidence in men is gradually increasing; therefore, it is necessary to develop a management plan for male osteoporosis in the future.
In our study, the number of newly diagnosed patients every year is higher than the increment of osteoporosis patients. This suggests that poor compliance is one of the most important treatment problems. A large US database of 58,109 osteoporotic patients, who initiated drug therapy for osteoporosis, reported a 1-year compliance rate below 25% for all osteoporosis therapies.16 In a longitudinal cohort of 211,319 patients who took bisphosphonate, patients new to bisphosphonates had the worst medication adherence over the year follow-up (25.2% for weekly and 13.2% for daily dosing).17 Similarly, in Korea, recent reports show that only 30% of patients take treatment for more than one year.18 According to our operational definition, newly diagnosed patients may include patients who have stopped taking medication for several years and then restarted. There is a possibility that it is overestimated. Nevertheless, the tendency toward decrease in women is a serious problem, and further research is needed to analyze the cause.
Although the prevalence of osteoporosis increases with age,1920 this study showed that very elderly patients have a lower medical utilization rate for osteoporosis. The utilization of medical services began to increase after age 60 and was highest for men in their 80s and for women in their 70s. After 80 years of age, the utilization decreased dramatically especially in women. The results of previous studies that analyzed the use of osteoporosis-related medical services based on the data of the Health Insurance Review and Assessment during 2005 to 2008 were similar to that of this study.1421 Therefore, our study indicates that very elderly women in Korea have low accessibility to medical services and accessibility has not yet improved. Although further research is needed, the difference may be caused by men generally having increased access to medical services through job screenings. However, this problem is not faced by our country alone. A recent study in the United States also showed that women over 80 years were one-third less likely to utilize recommended services within 6 months after fracture, compared to those aged 50 to 79 years.22 In Korea, lumbar spine BMD measurements have been performed for women aged 66 years as part of the national health screening program.23 The increased utilization by women in their 60s may have been influenced by this screening policy. Therefore, it appears that the new national screening program is likely to overcome a sharp decline in elderly women's health care utilization.
Among the patients with BMD-based osteoporosis in 2008 to 2010, the health service utilization rate was about 60%, while the treatment rate based on drug prescription data was about 32.9%. According to data from a previous nationwide survey, the treatment rate of BMD-based osteoporosis patients was 12.8% (female 14.4%, male 4.0%), which was lower than that of our study.10 However, in this study, treatment was determined by claim data of medications indicated only for osteoporosis, rather than by self-reporting questionnaires as performed in previous studies. Therefore, our results showed the actual treatment pattern of osteoporosis patients in Korea. There are few reliable published reports on the treatment rate for osteoporosis in the general population. In this study, the treatment rates for the entire Korean population over 50 years of age were 6.6%, 7.2%, and 7.3% in 2008, 2009, and 2010, respectively. According to the report by the International Osteoporosis Foundation to the European Union, the proportion of persons aged 50 years or more in 2010 ranged from 0.5% in Bulgaria to 9.3% in Spain, an average of about 5%.24 Therefore, the treatment rate in Korea is not low compared to that in other countries. However, compared with the treatment rate of other chronic diseases such as diabetes (48.8%) or hypertension (66%) in Korea,2526 the treatment rate of osteoporosis is still low; therefore, greater effort is needed to raise awareness of osteoporosis treatment.
This study has several limitations. First, values of the BMDs of the patients were not available because the study was designed based on claims data. Therefore, caution must be used when comparing the prevalence data with that of other studies. However, this study showed the proportion of people who actually accessed osteoporosis-related health services and estimated the real burden of osteoporosis in Korea. Second, there are disadvantages of insurance claim databases such as failure to include prescriptions outside insurance coverage (less than 1% in Korea), incorrect diagnostic coding, and misclassification error by patient-defining algorithms. However, the KNHIS provided a representative data of the total Korean population and minimizes selection bias. This is the major strength of the present study. Finally, it is difficult to determine the cause through the analysis of the claim data. Further research is needed through questionnaires to analyze the cause of these consequences.
In conclusion, this study demonstrated a substantial increase in the trend of utilization of osteoporosis-related health services from 2008 to 2012 in Korea. In men, the increase in medical service utilization was higher than in women, and the proportion of newly diagnosed osteoporosis patients tended to increase. This implies an increase in the need for prevention and treatment of male osteoporosis. Although the treatment rate for osteoporosis was not low compared to that reported by other studies, the rate was lower than that for other chronic diseases in Korea. Osteoporosis may not have obvious symptoms; therefore, it is presumed that patients do not access medical treatment because of ignorance of the disease. Therefore, more efforts are needed to improve awareness of osteoporosis treatment.
 XML Download
XML Download