

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In Korea, between 1980 and 1989, the overall hepatitis B surface antigen (HBsAg) seropositivity rate was 7.95% (9.11% in men and 7.13% in women); it was 5.67% in school children (1). With the success of national vaccination program, however, it was 3.2% in 1988 and 2.6% in 1993 in school children aged between 6 and 17 years old. In addition, it was 0.9% in infants and toddlers living in Seoul in 1995 (2). During a period ranging from 1997 to 1999, the mean HBsAg seropositivity rate was 2.5% (1%–4% in elementary school students and 3.2% in middle-to-high school ones) (3). According to the 4th Korea National Health and Nutrition Examination Survey (KNHANES IV) performed in 2007, the HBsAg seropositivity rate was dropped to 0.44% in middle school students and 0.2% in toddlers aged between 4 and 6 years old (4). Moreover, a recent large-scale, nationwide survey on the prevalence of hepatitis B virus (HBV) in the United States showed that the overall prevalence of HBV was 0.3%; it has remained unchanged since 1999. Furthermore, it was 2 to 3 times higher in non-Hispanic blacks and 10 times higher (3.1%) in non-Hispanic Asians as compared with a general population (5). The overall prevalence of HBV is also approximately 3.1% in Korea (6). People are vulnerable to HBV infections due to the closed society of Asian countries although the national HBV vaccination has dramatically reduced chances of contracting HBV infections (7).
In Korea, the national HBV vaccination was first introduced in 1983. Since 1987, it has been performed in most of the hospitals and clinics, thus being settled as a routine vaccination in 1991. Thus, it was finally listed as one of National Mandatory Vaccines in 1995. Since then, the national vaccination program for newborns has been implemented. According to a survey performed by the Korea Institute for Health and Social Affairs in elementary, middle or high school students, the antibody to hepatitis B surface antigen (anti-HBs) seroconversion rate was estimated at 79.7% in infants who were born and then completed a 3-dose vaccination between 1983 and 1990 and 98.9% in those after 1990 (8).
According to other studies, however, there was a variability in the seropositivity rate of anti-HBs after the national HBV vaccination program. In more detail, according to the KNHANES I performed in 1998, the overall seropositivity rate of anti-HBs was 57.0% in healthy men and 58.9% in healthy women, most of whom had not been fully vaccinated for HBV. In toddlers aged between 4 and 6 years who completed a 3-dose national vaccination program, however, the seropositivity rate of anti-HBs was 94.9% (9). According to a 20-year Taiwanese prospective study, however, the overall seropositivity rate of anti-HBs was 55.9% in 3,332 individuals at 20 years of the HBV vaccination (10). There was also another contradictory report that it was significantly lower (36.4%) in younger individuals (11). This suggests not only that the seropositivity rate of anti-HBs might vary depending on countries but also that it would not exceed 90% at all events.
Use of a booster dose is not recommended for healthy infants and children, which is based on published studies. Leuridan and Van Damme (12) performed a review of literatures, thus reporting that it is not required for immunologically competent persons although it is effective in reducing or abolishing the binding of anti-HBs to HBsAg. These authors noted, however, that it is solely recommended for immuno-compromised patients. Their report may be applicable to developed countries where the HBV seropositivity rate is relatively lower. A booster vaccination would not be mandatory for healthy individuals completing a 3-dose neonatal HBV vaccination. According to a study conducted in native Alaskans, although patients receiving HBV vaccination showed a treatment effect for the following 15 years, 1.27 of 1,000 patients developed a breakthrough infection (13). It can therefore be inferred that it would be mandatory to perform a further follow-up, which is essential for determining whether a booster dose is required for HBV-endemic areas.
In a clinical setting, we have encountered many individuals who are identified as those with negativity for or very low titers of anti-HBs antibodies on a regular medical check-up. Korea is one of the HBV-endemic areas. It is therefore mandatory to maintain a protective level of anti-HBs for life, for which it is necessary to obtain a complete understanding of chronologic changes in anti-HBs seropositivity.
In Korea, neonatal HBV vaccination has been performed for all neonates since 1985. Its rate was reported to reach up to 98% in 1988. Before the year of 2005, neonates were vaccinated with plasma-derived vaccine or recombinant DNA vaccine at birth, the 1st, and 2nd or 6th postnatal month (7). On the other hand, after the year of 2005, neonates were vaccinated with recombinant DNA vaccine only at birth and in the 1st and 6th postnatal month (14). In Korea, plasma-derived vaccine has become unavailable since 2005 (15).
Given the above background, we conducted this study to examine the positivity rate of anti-HBs, negative seroconversion after previous positive anti-HBS status depending on the types of HBV vaccines: plasma-derived vaccine or recombinant DNA vaccine. In addition, we also examined anti-HBs seropositivity rate among those who received booster vaccination.
MATERIALS AND METHODS
Patients and study setting
We conducted the current single-center, retrospective study in a total of 20,738 Korean individuals (10,589 men and 10,149 women) who visited the outpatient clinic of our medical institution and underwent HBV serologic tests as a routine screening test between December of 2000 and July of 2015.
Inclusion criteria for the current study are as follows: 1) The subjects who were not victims of HBV infections, and 2) The subjects who received neonatal HBV vaccination.
Exclusion criteria for the current study are as follows: 1) The subjects who were born of HBV-positive mothers, 2) The subjects who are HBV carriers, 3) The subjects with positive anti-HBc, 4) The subjects who frequently received blood transfusion or hemodialysis, 5) Individuals with immunocompromised status, and 6) The subjects who were deemed to be ineligible for study enrollment according to our judgment.
Excluding 1,666 subjects who did not meet eligibility criteria, we enrolled a total of a total of 19,072 (n = 19,072; 9,721 men and 9,351 women; mean age of 14.1 ± 7.6 years old).
Enzyme-linked immunosorbent assay (ELISA) for determining serologic markers of HBV
All the subjects were evaluated for serum HBsAg and anti-HBs and anti-HBc antibodies. Moreover, the subjects with positive HBsAg were also evaluated for HBeAg and anti-HBe antibodies. A 3 mL blood sample was collected and then centrifuged. This was followed by ELISA using the Roche Cobas e602 (Roche Diagnostics, Indianapolis, IN, USA). The subjects with HBsAg were determined to be seropositive at a cut-off index (COI) of HBsAg, anti-HBsAb, and anti-HBcAb of > 1.0, 10 mIU/mL and 1.0, respectively.
Patient evaluation and criteria
We divided the subjects into 2 groups: the group A (the year of birth < 2005) and the group B (the year of birth > 2005). Then, we compared the effects of neonatal vaccination on seropositivity of anti-HBs, disappearance of anti-HBs and seroconversion after booster vaccination between the 2 groups.
It is known that most neonates are positive for anti-HBs during the first 6 months after birth, when maternal antibodies are positive. We therefore narrowed the age range to babies aged 8–12 months old. In the current study, we analyzed the seropositivity rate of anti-HBs in the age range of 0–9 years old. In addition, we also analyzed the anti-HBs disappearance rate in the age range of 1–7 years old. The reason why the age range was set at 1–7 years old is that the number of children who were 8 and 9 years old was very small in group B.
Statistical analysis
Descriptive variables were expressed as percentages (%). To compare anti-HBs seropositivity rates between the group A and the group B, χ2-test was performed in each group. Considering that there is an age-dependent decrease in the seropositivity rate, we compared it between the 2 groups after the adjustment of the age. That is, we performed an age-adjusted logistic regression analysis. In addition, we also performed a subgroup analysis depending on the age. Statistical analysis was performed using the SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA). A P value of < 0.05 was considered statistically significant.
RESULTS
Baseline and clinical characteristics of the individuals
Our subjects (n = 19,072) comprise 9,721 men and 9,351 women with a mean age of 14.1 ± 7.6 years old.
Seropositivity of anti-HBs
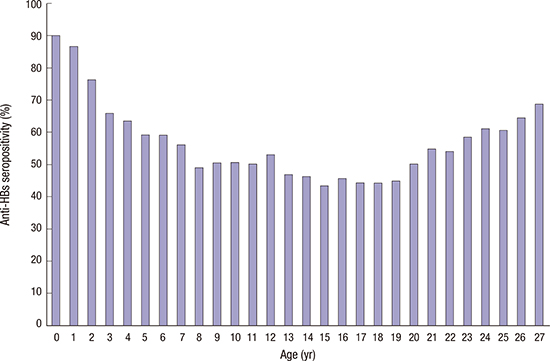
We calculated the overall anti-HBs seropositivity rate and provided its distribution using a range of 0–27. This showed that 10,641 and 8,431 subjects had a seropositivity and a seronegativity for anti-HBs, respectively. Thus, 55.8% of total subjects had a seropositivity for anti-HBs; it was 53.0% (8,957/16,915) in the group A and 78.1% (1,684/2,157) in the group B. This difference reached statistical significance (P < 0.001). The anti-HBs seropositivity rate reached the highest level (90.0%) at the age of < 12 months old. Until the age of 15 years old thereafter, however, it was decreased and then reached the lowest level of 43.5%. Since the age of 16 years old, however, it was gradually increased (Fig. 1).
Fig. 1
The anti-HBs seropositivity rate depending on the age. The anti-HBs seropositivity rate reached the highest level (90.0%) at the age of < 12 months old. Until the age of 15 years old thereafter, however, it was decreased and then reached the lowest level of 43.5%. Since the age of 16 years old, however, it was gradually increased.
Anti-HBs = antibody to hepatitis B surface antigen.
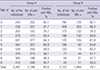
In 2005, the Korean government declared the policy to solely use recombinant DNA vaccine. We therefore compared the seropositivity rate between children aged 9 years or younger in each group. Thus, the overall anti-HBs seropositivity rate in this age subgroup was 68.5%; it was 62.6% (2,188/3,497) in the group A and 78.1% (1,684/2,157) in the group B. This difference reached statistical significance (P < 0.001). After the adjustment of the age, a logistic regression analysis was performed. This showed that there was no significant difference in the mean seropositivity rate between the 2 groups (P = 0.058). In addition, it was evident that the positivity rate was significantly lower in the group A as compared with the group B during infancy (83.1% vs. 92.1%, P < 0.001). After the period of infancy, however, there was no age-dependent significant difference in it between the 2 groups (Table 1).
Table 1
The anti-HBs seropositivity rate depending on the types of vaccine
Seroconversion from seropositive to seronegative status
A total of 1,106 subjects aged between 1 and 25 years old underwent serologic tests more than twice. Of these, 217 subjects (19.6%) achieved seroconversion from seropositive to seronegative status. There was an age-dependent increase in the rate of seroconversion from seropositive to seronegative status; it reached the highest level (45.5%) at the age of 9 years old. Thereafter, however, it was decreased (Fig. 2).
Fig. 2
The rate of seroconversion from seropositive to seronegative status depending on the age.
A total of 1,106 subjects aged between 1 and 25 years old underwent serologic tests more than twice. Of these, 217 subjects (19.6%) achieved seroconversion from seropositive to seronegative status. There was an age-dependent increase in the rate of seroconversion from seropositive to seronegative status; it reached the highest level (45.5%) at the age of 9 years old. Thereafter, however, it was decreased.
Anti-HBs = antibody to hepatitis B surface antigen.

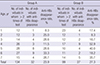
The rate of seroconversion from seropositive to seronegative status in the age subgroup of 1–7 years old was 23.9% in the group A and 27.3% in the group B. But this difference reached no statistical significance (Table 2).
Table 2
The age-specific anti-HBs disappearance rate depending on the types of vaccine
Seroconversion from seronegative to seropositive status after booster vaccination
A total of 95 seronegative subjects aged between 1 and 25 years old underwent booster vaccination after the initial serologic tests. Of these, 83 subjects (87.4%) achieved seroconversion from seronegative to seropositive status. There was a variability in the interval of serologic tests and the exact date of booster vaccination between them. The rate of seroconversion from seronegative to seropositive status of 87.4% would be meaningful for subjects with anti-HBs seronegativity from HBs-endemic areas.
DISCUSSION
We conducted the current study to examine anti-HBs seropositivity after neonatal HBV vaccination and the immunogenicity after booster vaccination. In Korea, HBV vaccines first became commercially available in 1983 (14). With the introduction of technologies from foreign manufacturers, Korean companies have successfully produced their own products; these include plasma-derived and heat-inactivated vaccines. Immunogenicity of these vaccines in adults has been reported to be 92% when administered at 0, 1, and 2 months and 96% when administered at 0, 1, and 6 months (16). Plasma-derived vaccines are manufactured using plasma samples obtained from HBV carriers. But safety from viral transmission and high cost remain problematic (17). Therefore, their production has been prohibited since 2004, being later than 1986 when their clinical use became unavailable in developed countries (18). On the other hand, recombinant DNA vaccines were first introduced in Korea in 1992. They have been solely used since 2005 (14). They are manufactured using Saccharomyces cerevisiae or Hansenula polymorpha. It is widely known that they are effective in maintaining a protective level of anti-HBs (> 10 mIU/mL) in more than 90% of individuals at 0, 1, and 6 months of the completion of vaccination (19). It is also known that even the non-responders achieved anti-HBS after completing a 3-dose vaccination (20). According to a large-scale study conducted in 332,870 children, aged between 6 and 17 years old, undergoing national HBV vaccination program, there was a dramatic increase in the seropositivity rate from 21.7% in 1988 to 54.1% in 1993 (21). Moreover, in Korea, since 1983 when the national HBV vaccination was first performed, there has been a 2-fold increase in the rate of anti-HBs seropositivity (14).
In our series, the overall anti-HBs seropositivity rate was approximately 55.8% (10,641/19,072). This indicates that almost half of the subjects have not been protected from HBV infections. In addition, our results showed that the highest rate of anti-HBs seropositivity was 90.0% in infants aged 1 year or younger. Our results are consistent with a previous report showing that the rate of anti-HBs seropositivity was 50.5% in a general population at 20 years of the national HBV vaccination program (22). This is also accompanied by a report that it was extremely low in individuals born after the implementation of the national HBV vaccination (0.6% at 15 years and 1.2% at 20 years). These reports noted that there were no new HBV carriers, thus suggesting that the national HBV vaccination is sufficiently effective in protecting against HBV infections for the first 20 years of the vaccination despite a relatively lower rate of anti-HBs seropositivity. But chances of contracting HBV infection remain as a concern to adults performing active social and sexual lives. According to a large-scale Korean study conducted in a general population in 2010, adults were vulnerable to HBV transmission based on the findings that the rate of HBsAg seropositivity was 2.29% in subjects aged between 10 and 39 years old and 0.12% in those aged between 10 and 19 years old (23). As shown in Fig. 1, there was an age-dependent decrease in the rate of anti-HBs seropositivity within the age range of 1–15 years old. This was followed by an increase in it thereafter. These results indicate that exposures to HBV during adulthood may provoke anamnestic responses of vaccine-induced anti-HBs and thereby prevent the occurrence of HBV infections. Although a booster dose is not recommended for HBV vaccination, there were some subjects who received booster vaccination. Of these, infants aged 1 and 7 years old achieved the highest rate of seroconversion from seronegative to seropositive status. This suggests that there is an inverse correlation between the degree of anamnestic responses and the age of the subjects receiving booster vaccination.
According to the World Health Organization (WHO) recommendations, individuals with normal immune functions cannot receive booster vaccination who have already completed a vaccination (24). But there are recent contradictory reports that the effects of neonatal HBV vaccination in protecting against HBV infections would last for at least 20 years if performed during childhood and adulthood following an analysis of the rate of anti-HBs seropositivity in individuals receiving the primary hepatitis B vaccination series using the plasma-derived vaccine, which was followed by the conclusion that booster vaccination would not be mandatory (212526). According to another 18-year follow-up study conducted in 318 children who are at increased risks of contracting HBV infections from Hong Kong, the degree of anamnestic responses was so sufficient as not to require a booster vaccination for 18 years (27). In the current study, the overall disappearance rate of anti-HBs was approximately 19.6%, which was followed by a gradual increase in it until the age of 9 years old. Except for those who either had never developed anti-HBs or initially developed but later became seronegative, however, there were no subjects who achieved seropositivity for HBsAg afterwards. There were some subjects who received booster vaccination according to their own decision. But this is unnecessary based on the WHO recommendations and the relevant literatures.
A Taiwanese study showed that the rate of the disappearance of anti-HBs was significantly higher in subjects receiving recombinant DNA vaccine as compared with those doing plasma-derived one (62.7% vs. 42.8%) at 12–15 years of the neonatal vaccination. That study also noted that the final rate of anti-HBs seropositivity was significantly higher in subjects receiving recombinant DNA vaccine as compared with those doing plasma-derived one (94.4% vs. 81.0%). Thus, it recommended the booster vaccination using recombinant DNA vaccine to non-responders in their teens (28). According to another Taiwanese study, there was a decrease in the rate of anti-HBs seropositivity to 50% at 15 years of the vaccination, which was followed by a report that booster vaccination was effective in as high as 100% of total subjects (29). Taken together, we also propose that booster vaccination be considered for individuals with seroconversion from seropositive to seronegative status without anti-HBs or non-responders.
It has been reported that there was a positive correlation between the rate of seroconversion from seronegative to seropositive status and the frequency of booster vaccination (30). According to a long-term, multi-center immunogenicity study conducted in Italy, the rate of seroconversion from seronegative to seropositive status was 97% in children and 96% in total subjects after the completion of a 1-dose booster vaccines and 99.4% in children and 100% in total subjects after a 3-dose booster vaccination (31). This is consistent with our results. Immunological memory for HBsAg could provide a protective effect even at lower titers of anti-HBs of < 10 mIU/mL. Individuals with anti-HBs seronegativity or those who had chronologic disappearance of anti-HBs would not have a seropositivity for HBsAg (32). This deserves further studies because such individuals are children or younger adults. Several earlier studies have already demonstrated that individuals with anti-HBs seronegativity would be at increased risks of contracting HBV infections even at 20 years of the vaccination (3334). This is noteworthy in HBV-endemic areas, including Korea, which has also been supported by several published studies. According to a Taiwanese study conducted in 2010, there was a lack of anamnestic responses in 25% of college freshmen, which was followed by a report that more than 90% of total subjects achieved a seroconversion from seronegative to seropositive status after completing a 2-dose booster vaccination (35). According to another study conducted in medical personnel from Israel, the rate of anti-HBs seropositivity was 33.7% at baseline, 87.7% after the first booster vaccination and 97.9% at one month of the second one (36).
This study has some limitations in that the subjects were selected randomly and studied retrospectively, and serologic data were available for different numbers of cases in different age groups. If a further prospective study over decades could be performed in the future with a larger study population, it might present more accurate, comparable, and helpful data.
In conclusion, our results provide long-term perspectives about persistence of anti-HBs seropositivity. But they did not meet the known expectations. Anti-HBs does not persist as protective titer in some individuals. Thus, our results highlight the importance of reassurance about HBV protection after adolescent period.
 XML Download
XML Download