

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cluster headache (CH) is a neurological disorder characterized by unilateral, severely painful headaches, clustering of headache episodes, and autonomic accompaniment (12). Despite these striking features, it is a rare primary headache disorder and remains underdiagnosed and undertreated (345). The delayed time to diagnosis of CH from onset is approximately 2–8 years; over half of patients with CH do not receive proper treatment before visiting a specialized headache clinic (678).
CH has some interesting and prominent anthropometric and chronobiologic features, including male preponderance and seasonal and diurnal periodicity (910). The higher proportion of men presenting with CH suggests a hormonal influence, but the pathophysiology of CH remains uncertain (1112). Few studies have reported clinical differences in female CH patients in the USA and Italy, so the study of CH sex differences in a different setting is warranted (1314). The typical CH patient is a young male adult, but CH has been reported from childhood to old age, so the age of onset may play a role in the features of CH (15161718).
Compared to CH patients in Western countries, Asian CH patients have been reported to have a lower prevalence of chronic CH, aura, and restlessness (6131920212223). However, the clinical features of Korean CH patients have not yet been reported and the previous studies in the journals published in Korea have been limited to a few case reports (2425). Therefore, we investigated the clinical features of Korean CH patients and the influence of sex and age of onset on the features of CH.
MATERIALS AND METHODS
This study population consisted of 2 databases. The first was from a prospective multicenter headache registry study conducted with Korean patients diagnosed with trigeminal autonomic cephalalgia (TAC) in the headache clinics of 7 university hospitals in Korea between June 2011 and November 2013. The second was the TAC patients database of patients diagnosed between May 2002 and June 2013 in the headache clinics of 11 university hospitals in Korea that were not included the above prospective study. Data from these patients were obtained by retrospectively reviewing their medical records. Pediatric patients younger than 19 years, patients with declined cognitive function or language problems, TAC patients other than CH, and patients with secondary headache presenting as TAC headache were excluded. To avoid overlapping data, only the data from the hospital visited most recently were included for patients that visited multiple hospitals.
Headache assessment and diagnosis
Each patient underwent a detailed clinical interview and neurological examination by a neurologist. Appropriate brain imaging was conducted when secondary headache was suspected. CH improvement, recurrence, and headache patterns at each attack were also evaluated through follow-up. All of the patients that met the CH diagnostic criteria of the second edition of International Classification of Headache Disorders (ICHD-2) were included after compiling the results of the questionnaire analysis, medical records, neurological examinations, appropriate testing, and responses to treatment.
According to the ICHD-2, episodic CH consists of 2 cluster attacks lasting 7–365 days and separated by pain-free periods of ≥ 1 month, and chronic CH consists of attacks recurring over > 1 year without remission periods or with remission periods lasting < 1 month. CH patients with attacks fulfilling all but one of criteria A–D for 3.1 CH were classified as probable CH. CH patients with only a single cluster period were classified as 3.1 CH.
Clinical data collected included age at onset; sex; laterality, location, and characteristics of headaches; cranial autonomic features; presence or absence of migraine features (e.g., nausea, vomiting, photophobia, or phonophobia); time to diagnosis from onset; bout duration and frequency; seasonal and diurnal periodicity; possible trigger factors; history of smoking; and treatment.
Statistical analysis
Statistical analysis was conducted using SPSS for Windows Version 18.0 software (IBM Corp., Armonk, NY, USA). The clinical characteristics of CH are presented as descriptive statistics. For continuous data, statistical differences were evaluated using the Student's t-test and Mann-Whitney test. Categorical variables were analyzed using the χ2 test.
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of Hangang Sacred Heart Hospital (IRB No. 2011-158) and Dongtan Sacred Heart Hospital (IRB No. 2013-046). All patients gave their informed consent to participate in this study or the informed consent process was waived in accordance with the decision of the ethics committee of each hospital.
RESULTS
The subtypes of CH
The retrospective database consisted of 127 CH patients and the prospective database consisted of 73 CH patients. There were no significant differences in age at onset, sex ratio, duration and frequency of attack, or the total duration of CH between the 2 databases.
A total of 200 CH patients suffered 3.0 ± 3.5 (1–25) bouts over 7.3 ± 6.7 years (range 1–30 years). Forty-four patients (22%) experienced a single cluster period and were classified as CH (ICHD-2 code 3.1). Of the remaining 156 patients, a 43-year-old male patient was classified as chronic CH (ICHD-2 code 3.1.2), a 36-year-old male patient was classified as probable CH (ICHD-2 code 3.4.1) due to lack of accompanying symptoms, and 154 patients were classified as episodic CH (ICHD-2 code 3.1.1).
The age at onset and sex ratio
The mean age of onset was 30.7 ± 10.3 years (range 10–57 years) and the mean age at clinic visits was 38.1 ± 8.9 years (range 19–60 years). There were 175 male (87.5%) and 25 female (12.5%) patients, resulting in a male-to-female ratio of 7:1. The male-to-female ratio was 2.9:1 among CH patients with onset in their teens, 11.7:1 among those with onset in their twenties, 8.5:1 among those with onset in their thirties, 8.3:1 among those with onset in their forties, and 3:1 among those with onset in their fifties (Fig. 1, P
= 0.141).

Headache features of CH
Pain was reported as very severe, at 9.3 ± 1.0 on the visual analogue scale. Headache laterality was left-sided in 47.5%, right-sided in 45.0%, alternating in 6.0%, and unspecified in 1.5% of patients. Associated trigeminal autonomic symptoms were conjunctival injection and/or lacrimation in 85.5%, nasal congestion and/or rhinorrhea in 58.5%, eyelid edema in 23.0%, forehead and facial sweating in 8.5%, miosis and/or ptosis in 8.5%, and a sense of restlessness or agitation in 43.5% of patients. At least 1 autonomic symptom was present in 94.0% of patients, and restlessness or agitation without autonomic symptoms was present in 5.5% of patients. Only 1 patient reported aura. There were no significant differences in associated symptoms between female and male patients.
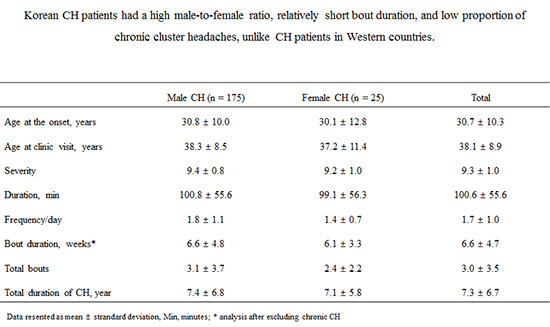
The mean frequency was 1.7 ± 1.0 per day, and the average duration of each attack was 100.6 ± 55.6 minutes. The mean duration of a cluster bout of episodic or probable CH with 2 or more attacks was 6.5 ± 4.5 (range 1–28) weeks, and the duration of chronic CH was 30 months. There were no significant differences in age at onset or clinic visit; frequency and duration of attacks; or duration and frequencies of bouts between female and male patients (Table 1).
Table 1
Clinical characteristics of CH according to sex
Diurnal and seasonal propensity
Diurnal periodicity was present in 68.5%, absent in 6.0%, and unclassified in 25.5% of patients. Among 137 patients with diurnal periodicity, the most frequently cited time was night in 66.4%, morning, afternoon, or evening in 23.4%, and both day and night in 10.2% of patients. There was no significant difference in attack time between female and male patients. Seasonal propensity was present in 44.0%, absent in 33.0%, and unclassified in 23.0% of patients. Among 88 patients with seasonal propensity, the most frequently sited season was spring (37.5% of patients). The distribution of other seasonal propensities was winter in 18.2%, autumn in 14.8%, summer in 13.6%, and multiple seasons in 15.9% of patients.
Previous history of migraine, smoking history, and obesity
Analysis about comorbidity of migraine was done in 72 CH patients among the prospective population. A previous history of migraine was present in 14 patients (19.4%). Regarding migraine-associated symptoms, patients reported nausea (48.6%), vomiting (25.0%), photophobia (8.3%), and phonophobia (9.7%). There were no significant differences in headache features between female and male patients.
Smoking history was available for 150 patients. Among them, 35% were current smokers, 6% had previous smoking history, and 34% never smoked. Body mass index was available for 113 patients. Mean body mass index was 23.8 ± 2.7 kg/m2, and 17% of patients were obese (> 25 kg/m2). Men were more frequently smokers (50.8% in men vs. 22.7% in women, P = 0.004) and had higher body mass indices (24.1 ± 2.4 kg/m2 in men vs. 21.4 ± 3.3 kg/m2 in women, P = 0.002).
Separate analysis according to the age of onset and sex
Clinical features were compared between 3 groups by the age at onset: young onset (10–29 years, n = 35), middle-aged onset (30–49 years, n = 145), and older-aged onset (50 years and older, n = 20). Restlessness or agitation was less common among middle-aged onset than among young or older-age onset (35.9% vs. 65.7% and 60.0%, respectively P = 0.002). The other associated symptoms were not different between the 3 groups. There were no significant differences in the frequency and duration of attacks or bouts between 3 groups. There were no differences in associated symptoms or diurnal and seasonal periodicity according to sex.
DISCUSSION
This was the first multi-center study of clinical features of CH in Korea. The key findings of this study are summarized as follows: 1) the male-to-female ratio was 7.1, with highest ratio at 11.7 among twenties-onset patients; 2) chronic CH was rare; 3) the mean frequency was 1.7 times per day, the average attack duration was 100.6 minutes, and the mean cluster bout duration of episodic CH was 6.7 weeks; 4) restlessness or agitation accompanied attacks in 43.5% of patients; and 5) restlessness or agitation was less common among middle-aged CH patients. Otherwise, clinical features of CH did not differ according to sex or age of onset.
The male-to-female ratio ranges from 3.8–7:1 from studies in Asia and from 1.3–3.5:1 in Western studies (36192026). This study confirms the higher male to female ratio in Asia. The more prominent male preponderance may be related to ethnic, cultural, or lifestyle differences, such as the relatively low smoking history among Asian women (26272829). However, a more significant diagnostic delay has been reported in female CH patients, so we cannot rule out an influence of the diagnostic delay sex gap on the male-to-female ratio in Korea (13). The highest male-to-female ratio among twenties may be related to bimodal or stable incidence of female CH through age (133031).
Chronic CH was rare in this study, which is consistent with previous studies from Asia; the proportion of chronic CH was reported as 0.0%–7.5% in Asia and as 15.2%–25.9% in Western countries (61920323334). The clinical course of CH lasted more than 10 years; approximately 10% of episodic CH transformed into chronic CH, and more than 30% of chronic CH became episodic in Western studies (3234). Therefore, the proportion of chronic CH should be reevaluated in long-term follow-up studies.
The association of smoking and CH is disputable. There is a high prevalence of smokers among CH patients compared to the general population; CH patients with smoking history have longer and more frequent attacks per day, and CH continues after quitting smoking (92835). The proportion of smoking history among female CH patients was 22.7%, which is substantially higher than that in the Korean female general population at 5.3% (28). Interestingly, the smoking prevalence in the general population of Korean men is higher than that of women (2010 statistics, 43.5% vs. 5.3%, respectively) (28) and the trend is similar to that of the male-to-female ratio of CH (Table 2). These trends suggest an influence of smoking on CH prevalence, but the complex relationship between sex, smoking, and CH remains uncertain.
Table 2
Male to female ratio in patients with CH and smoking prevalence of males and females in Korea, China, Japan, and US general population
| Parameters | Korea | China | Japan | US |
|---|---|---|---|---|
| Male-to-female ratio in CH | 7:1* | 7:1 (6) | 3.8:1 (19) | 2.6:1 (13) |
| Smoking prevalence of males/females, % | 43.6/5.3 (26) | 52.9/2.4 (27) | 33.7/10.6 (38) | 24.0/16.2 (27) |
The mean bout duration in this study was 6.6 ± 4.7 weeks. This may be shorter in Asia, including Taiwan (5.8 ± 5.0 weeks) and China (75% of CH patients had bout durations shorter than 2 months), than in Western countries, including Germany (8.5 ± 5.7 weeks) or Italy (10.3 ± 8.0 weeks) (6203536). Whether Asian CH patients have shorter bout durations or better response to treatment is an important topic for future CH studies.
There were no prominent differences in clinical features or diurnal/seasonal propensity according to sex. This result is consistent with a clinic-based study from Italy (14). From a web-based survey study that enrolled 318 female and 816 male CH patients, female CH patients had more frequent language or brainstem aura, jaw or ear pain, nausea, migraine triggers, more daily attacks, and more pain (13). These differences may be related to differences in the study population and method of investigation. In addition, clinical features can be affected by treatment over a long clinical history of CH, so this comparison may be difficult or inconsistent in a cross-sectional study (34).
This study had several limitations. First, this was a multi-center clinic-based study, so selection bias was inevitable. However, CH is a rare headache disorder and some population studies of CH estimated its prevalence at 119–279/100,000 people (337). Therefore, headache clinics may be reasonable settings to evaluate the clinical features of CH. Second, some of our data were based on medical records. There were no significant differences in the comparison between prospective and retrospective headache feature data. Although the impressive features of CH encouraged detailed CH descriptions, some minor features or comorbidities of migraine could have been neglected. Therefore, these analyses about comorbidities of migraine, body mass index, and smoking history were done in the patients with relevant data. Although several studies of CH clinical features have been conducted using retrospective methods, a prospective registry study of CH including follow-up data may be warranted (1522233134). Third, although this is the largest number of Asian female CH patients studied to date, the number of female patients with CH was still relatively small.
In conclusion, Korean CH patients had a high male to female ratio, relatively short bout duration, and low proportion of chronic CH.
 XML Download
XML Download