

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Epithelial ovarian cancer (EOC) is the most common cause of cancer-associated death among women with gynecologic cancers (12). The current standard therapy for patients with advanced stage EOC consists of cytoreductive surgery and adjuvant combination chemotherapy with platinum and a taxane (34). Intraperitoneal (IP) administration of chemotherapy for EOC is effective as first-line treatment. Compared with standard IV treatment, IP chemotherapy was recently demonstrated in three large randomized phase III trials (567) to improve outcomes; a Cochrane meta-analysis confirmed these findings (8).
Given the toxicity associated with cisplatin-based IP chemotherapy and the emerging data on IP carboplatin administration from nonrandomized studies (9101112), we substituted carboplatin for cisplatin in IP chemotherapy and investigated the feasibility of this regimen (13). Few studies supporting the long-term efficacy or oncologic outcomes of carboplatin-based IP chemotherapy have been conducted during the last decade (1014), although randomized data to support the selection of an IP or IV regimen will soon be available from the GOG 252 (ClinicalTrials.gov identifier, NCT00951496) and OV21/PETROC (ClinicalTrials.gov identifier, NCT00993655) trials.
The purpose of this study was to compare the long-term survival of propensity score-matched advanced EOC patients treated with either IP or intravenous (IV) chemotherapy. Also, as a subgroup analysis, we compared the long-term outcomes among IP chemotherapy-treated patients according to chemotherapy regimens; carboplatin-based or cisplatin-based.
MATERIALS AND METHODS
Study design
Patients diagnosed with EOC and treated with IV or IP chemotherapy after cytoreductive surgery between January 2006 and December 2008, were included consecutively. Patients who received neoadjuvant chemotherapy before debulking surgery were excluded. A gynecologic oncology team at a single institute conducted all of the procedures, and a dedicated radiologist and pathologists at the same institute reviewed all data from the imaging studies and pathologic specimens, respectively. A retrospective chart review was performed to collect clinical and pathologic data. All patients were staged according to the International Federation of Gynecology and Obstetrics (FIGO) criteria for ovarian cancer.
The subjects in IP chemotherapy group received either 1) IP carboplatin area under curve (AUC) 5 on day 1, IV paclitaxel 175 mg/m2 on day 2, and IP paclitaxel 60 mg/m2 on day 8 or 2) IV paclitaxel 135 mg/m2 on day 1, IP cisplatin 100 mg/m2 on day 2, and IP paclitaxel 60 mg/m2 on day 8. Standard premedication was administered to prevent hypersensitivity reactions to paclitaxel, and hydration and antiemetic agents were administered before the administration of carboplatin. Before the IP infusion of chemotherapeutic agents, 500 mL of warm normal saline was infused through the peritoneal port. For the IP infusion, carboplatin or paclitaxel was reconstituted in 1 L of warm normal saline and infused as rapidly as possible through the port. After IP administration of the chemotherapeutic agents, 500 mL of warm normal saline was infused through the peritoneal port, followed by rolling the patient into 4 different positions every 15 minutes to disperse the drug throughout the peritoneal cavity. This series of treatments was performed every 3 weeks. For IP access, 31 BardPort catheters and 6 Tenckhoff catheters were used. BardPort implantable port is an access device designed to provide repeated access to IP infusion, and Tenckhoff catheter a cuffed silicone catheter that is permanently inserted into the abdominal cavity for infusion of solution (1516). Patients, who were determined to stop IP chemotherapy due to toxic effects, underwent sequential IV chemotherapy up to 6 to 8 cycles totally.
Routine follow-up was performed every 3 months, comprising a clinical examination and measurement of serum carbohydrate antigen 125 levels, and radiologic investigations when indicated. Recurrence and progression were evaluated using the Response Evaluation Criteria in Solid Tumors Committee (RECIST) (17). All toxicities were graded according to the National Cancer Institute's Common Toxicity Criteria for Adverse Events (NCI CTCAE) version 4.0 (18). Specifically, grade 3 hematologic toxic effects were defined as follows: anemia, hemoglobin < 8 g/dL; granulocytopenia, < 1,000 granulocytes/mm3; leukopenia, < 2,000 white cells/mm3; and thrombocytopenia, < 50,000 platelets/mm3. Grade 2 toxic effects were defined as follows: abdominal pain, pain relieved by oral opioids; fever, temperature > 38°C; tinnitus, moderate symptoms of tinnitus; hearing loss, ability to hear normal levels of voice and sound but not whispered sounds; neuromuscular effects, absence of deep tendon reflexes, weakness, and peripheral nerve pain; and pulmonary effects, transient dyspnea on mild exertion. IP port issues included infection, blockage, leakage, and peritoneal irritation by the catheter.
We used Kaplan-Meier survival analysis to compare long-term survival between 1:2 propensity score-matched patients with advanced EOC treated with either IP or IV chemotherapy. Additionally, clinical features associated with carboplatin-based or cisplatin-based IP chemotherapy were analyzed and compared with those associated with IV chemotherapy, during the whole course of chemotherapy.
Statistical analysis
IBM SPSS version 23 for Windows (IBM Corp., Armonk, NY, USA) was used for the statistical analysis. The Kolmogorov-Smirnov test was used to verify standard normal distribution assumptions. Pearson's chi-square, Fisher's exact, and Mann-Whitney U tests were used in the univariate analysis. To reduce the effect of selection bias and potential confounding in this retrospective cohort study, estimated propensity scores were used to match the IP group to IV group. In our study, this was computed for each of the patients using a logistic regression model including the following variables: age, FIGO stage, tumor histology, tumor grade, and residual disease. The propensity score model was well-calibrated (Hosmer-Lemeshow goodness-of-fit test, P = 0.987). Based on the propensity scores, 34 patients who underwent IP chemotherapy were matched to 68 patients who underwent IV chemotherapy. Progression-free survival (PFS) and overall survival (OS) for patients with stage 3 or 4 cancer were compared between the chemotherapy regimens using Kaplan-Meier survival analyses. A P value < 0.05 was considered statistically significant.
Ethics statement
The protocol received Institutional Review Board approval of the Yonsei University College of Medicine (IRB No. 4-2017-0031) and was performed in accordance with the ethical standards described in the Declaration of Helsinki. The requirement to obtain a written informed consent was waived by the Institutional Review Board of the Yonsei University College of Medicine because our study was retrospective research based on medical records, and this research presented no more than minimal risk of harm to subjects.
RESULTS
Flowchart of patient selection is presented in Fig. 1. The clinicopathologic characteristics of the IP (unmatched, n = 37; matched, n = 34) and IV (unmatched, n = 121; matched, n = 68) chemotherapy groups are listed in Table 1. The median durations of follow-up were 67 (range, 3–131) and 62 (range, 0–126) months for patients receiving IP and IV chemotherapy, respectively. Within the IP group, the median durations of follow-up were 52 (range, 16–131) and 96 (range, 3–126) months for carboplatin- and cisplatin-based IP chemotherapy subgroups, respectively.
Fig. 1
Flowchart of patient selection.
EOC = epithelial ovarian cancer, pts = patients, PDS = primary debulking surgery, NAC = neoadjuvant chemotherapy, CTx = chemotherapy, IP = intraperitoneal, IV = intravenous.

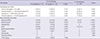
Table 1
Characteristics of patients in the IP and IV chemotherapy groups before and after propensity score matching

A description of the chemotherapy regimens is shown in Table 2. Adjuvant carboplatin- and cisplatin-based IP chemotherapy regimens were initiated 11.0 days and 9.5 days after primary staging surgery, respectively (P = 0.790). Notably, the number of total chemotherapy cycles was greater (P = 0.021) and the proportion of patients who received ≥ 6 cycles was higher in the carboplatin-based than in the cisplatin-based IP chemotherapy subgroup (P = 0.049). Compared with the entire IP chemotherapy group, the IV chemotherapy group had a significantly higher proportion (91.2%) of patients who received ≥ 6 cycles of chemotherapy (P = 0.004). Peritoneal recurrence was less likely to occur in IP chemotherapy group, compared with IV chemotherapy group (P = 0.002), even though the overall recurrent rate was not significantly different (P = 0.816).
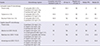
Table 2
Description of chemotherapy-related outcomes in propensity score-matched EOC patients by route of infusion, and by IP chemotherapy regimen

The frequency of toxic events related to IP and IV chemotherapy are summarized in Table 3. Patients undergoing cisplatin-based IP chemotherapy experienced more non-hematogenous toxicities than those treated with carboplatin-based IP chemotherapy: A significantly greater proportion of patients in the cisplatin-based IP chemotherapy group experienced grade 3 granulocytopenia (56.2% vs. 23.8%, P = 0.044) and leukopenia (62.5% vs. 23.8%, P = 0.018). Patients treated with cisplatin-based IP chemotherapy were also more likely than those treated with carboplatin-based IP chemotherapy to experience chemotherapy-related grade 2 or 3 nausea/vomiting (75.0% vs. 19.0%, P = 0.001), abdominal pain (62.5% vs. 23.8%, P = 0.018), hepatotoxicity (43.8% vs. 9.5%, P = 0.016), and neuromuscular effects (56.2% vs. 19.0%, P = 0.019). One patient who received cisplatin-based IP chemotherapy died after completion of 5 cycles of chemotherapy because of chemotherapy-related toxicity. Twelve patients (32.4%) experienced IP port-related complications, primarily port malfunction/obstruction and 1 case of catheter-related bowel irritation. Port-related complications necessitated discontinuation of IP chemotherapy in 4 patients. Compared to the entire IP chemotherapy group, the IV chemotherapy group had a significantly lower proportion of patients who experienced the following toxic events: anemia (P = 0.002), granulocytopenia (P = 0.034), nausea/vomiting (P < 0.001), abdominal pain (P < 0.001), hepatotoxicity (P < 0.001), and neuromuscular effects (P < 0.001).
Table 3
Frequency of hematologic toxic effects (≥ grade 3) and other toxic effects (≥ grade 2) during any course of treatment in patients with FIGO stage IIIC or IV ovarian cancer, by chemotherapy regimen
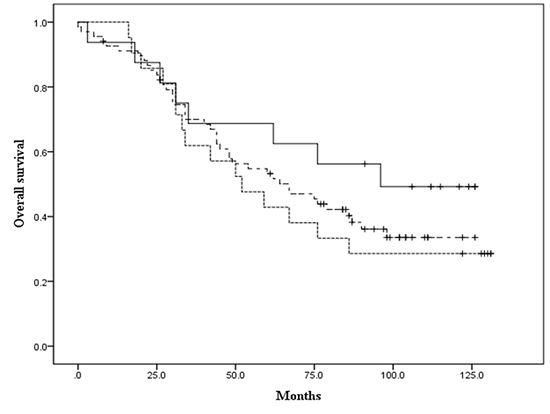
The Kaplan-Meier survival analysis showed no significant difference in PFS (P = 0.735, Fig. 2A) and OS (P = 0.776, Fig. 2B) between the IP and IV chemotherapy groups. The 10-year PFS was 26.4% and 20% in the IP and IV groups, respectively, while the 10-year OS was 38.0% and 33.5% in IP and IV groups, respectively. Moreover, within the IP chemotherapy group, there was no statistically significant difference in PFS (P = 0.533, Fig. 3A) and OS (P = 0.210, Fig. 3B) between the carboplatin-based and cisplatin-based IP chemotherapy subgroups: The 10-year PFS was 24.1% and 40.0% and the 10-year OS was 28.6% and 49.2% in carboplatin-based and cisplatin-based IP chemotherapy groups, respectively.
Fig. 2
Comparison of survival outcomes between IP and IV chemotherapy groups. (A) PFS according to treatment intention in patients with advanced EOC treated with IP or IV chemotherapy. (B) OS according to treatment intention in patients with advanced EOC treated with IP or IV chemotherapy.
IP = intraperitoneal, IV = intravenous, PFS = progression-free survival, EOC = epithelial ovarian cancer, OS = overall survival.

Fig. 3
Comparison of survival outcomes between cisplatin-based and carboplatin-based IP chemotherapy subgroups. (A) PFS according to treatment intention in patients with advanced EOC treated with IP chemotherapy. (B) OS according to treatment intention in patients with advanced EOC treated with IP chemotherapy.
IP = intraperitoneal, IV = intravenous, PFS = progression-free survival, EOC = epithelial ovarian cancer, OS = overall survival.

DISCUSSION
The present study demonstrated that carboplatin-based IP chemotherapy may be an acceptable alternative to cisplatin-based IP chemotherapy or conventional IV chemotherapy for the management of patients with advanced EOC in terms of long-term survival, although the toxicity of IP-based chemotherapy remains a problem. However, the lower frequency of toxic events observed with carboplatin-compared with cisplatin-based IP chemotherapy appears to be a key element allowing for completion of the planned ≥ 6 cycles of chemotherapy; this is a primary factor for a favorable long-term survival outcome (19).
The underlying principle of IP chemotherapy is the ability to deliver high concentrations of the appropriate chemotherapeutic agent to the site where most recurrences are likely to develop, after performing complete cytoreduction. Despite the National Cancer Institute (NCI) Clinical Announcement that was based on multiple trials showing level-1 evidence for a survival benefit (20), IP chemotherapy has not been widely adopted in the management of ovarian cancer. A previous study reported that even after the NCI Clinical Announcement, < 50% of eligible patients received IP chemotherapy (21), potentially because of various concerns including increased toxicity, multiday scheduling, and lack of familiarity with catheter placement and IP drug administration. Although a question remains as to whether a course of 6 IP treatments is optimal, only 42% of patients in the randomized GOG 172 trial, that compared IP and IV chemotherapy, received all 6 cycles of the assigned IP therapy due to intolerable toxic effects such as catheter-related complications; instead, a median of 3 cycles was delivered (7). Ultimately, when making decisions about the type of adjuvant treatment, doctors and patients should be empowered to consider convenience, potential toxicities, and quality of life in addition to the possible survival benefit (22).
To reduce the toxicities associated with cisplatin-based IP chemotherapy, some centers have adopted carboplatin-based IP regimens. Table 4 lists the results of carboplatin- and cisplatin-based IP chemotherapy in other randomized/non-randomized trials. In the present study, 83.3% of patients who underwent carboplatin-based chemotherapy completed the intended 6 cycles. Furthermore, 19 (90.5%) of the 21 patients had a complete response, and 2 had a partial response. Additionally, the median PFS was 20 months and the median OS was 52 months. In a previous study of IP carboplatin with IV paclitaxel in patients with suboptimal residual EOC, the response rate was 83.3% and the median PFS was 25 months; median OS had not been reached (12). A more favorable median OS was reported in another study of carboplatin-based IP chemotherapy, with smaller amounts of chemotherapeutic agent administered (14). However, the reported survival was based on actuarial data, limiting comparisons. The relatively lower median PFS and OS in the present study are partially due to the inclusion of patients whose cytoreduction was suboptimal: Because an IP chemotherapeutic agent penetrates to a depth of 2.0–2.5 mm, it is important that no gross residual disease is present before administration of IP chemotherapy (23).
Table 4
Comparison of the present IP chemotherapy results with those of other randomized/non-randomized trials
| Studies | Chemotherapy regimen | Completion rate of the intended 6 cycles, % | CR rate, % | Negative second look, % | Median PFS | Median OS |
|---|---|---|---|---|---|---|
| Carboplatin-based IP chemotherapy | ||||||
| Present study | IP carboplatin (AUC 5, D1), | 82.4 | 90.5 | NA | 21 | 52 |
| IV paclitaxel (175 mg/m2, D2), | ||||||
| IP paclitaxel (60 mg/m2, D8) | ||||||
| Fujiwara et al. (10) | IP carboplatin (AUC 6, D1), | 84.6 | 83.3 | NA | 25 | NA |
| IV paclitaxel (175 mg/m2, D1) | ||||||
| Bouchard-Fortier et al. (14) | IP carboplatin (AUC 6, D1), | 60.9 | NA | NA | 25.5 | 85.3 |
| IV paclitaxel (135 mg/m2, D1) | ||||||
| Cisplatin-based IP chemotherapy | ||||||
| Present study | IV paclitaxel (135 mg/m2, D1), | 50 | 81.3 | NA | 25 | 96 |
| IP cisplatin (100 mg/m2, D2), | ||||||
| IP paclitaxel (60 mg/m2, D8) | ||||||
| Alberts et al. (GOG 104) (5) | IP cisplatin (100 mg/m2, D1), | 58 | NA | 47 | NA | 49 |
| IV cyclophosphamide (600 mg/m2, D1) | ||||||
| Markman et al. (GOG 114) (6) | 2 courses IV carboplatin (AUC 9) then: | 71 | NA | NA | 27.6 | 63.2 |
| IV paclitaxel (135 mg/m2, D1), | ||||||
| IP cisplatin (100 mg/m2, D2) | ||||||
| Armstrong et al. (GOG 172) (7) | IV paclitaxel (135 mg/m2, D1), | 42 | NA | 57 | 24.3 | 65.6 |
| IP cisplatin (100 mg/m2, D2), | ||||||
| IP paclitaxel (60 mg/m2, D8) |
The oncologic outcomes of 3 studies on IP chemotherapy by the GOG, that compared IP with IV cisplatin administration, are also shown in Table 4. In the phase III GOG 104 trial that compared either 100 mg/m2 IP or IV cisplatin administered with IV cyclophosphamide (5), the median survival was significantly longer in the group treated with IP (49 months) than in the group treated with IV (41 months) cisplatin. The recently published phase III GOG 172 trial showed that IP therapy with cisplatin and paclitaxel was associated with longer survival in stage III patients who underwent optimal cytoreduction, compared with the IV chemotherapy group (median PFS of 18.3 and 28.3 months in the IV and IP chemotherapy groups, respectively, P = 0.050; median OS of 65.6 and 49.7 months, respectively, P = 0.030) (7).
Although our data suggest the feasibility of carboplatin-based IP chemotherapy, without sacrificing patient survival, this interpretation should be approached with caution. The retrospective nature of this study and small sample size might have resulted in selection bias regarding patient recruitment and may have limited the study's statistical power; our study was not powered to detect differences in survival. Moreover, the choice of carboplatin or cisplatin was not randomized or based on clear criteria but on the discretion of each gynecologic oncologist. The therapeutic effects of carboplatin-based IP chemotherapy should be further evaluated through a large randomized comparison study with cisplatin-based IP chemotherapy.
IP chemotherapy could gain widespread acceptance if the associated problems of drug-related toxicity are resolved. In addition, it is reasonable to substitute carboplatin—a less toxic, better-tolerated platinum agent—for cisplatin, particularly in patients with severe cisplatin-associated toxicity. Given the potential advantages of carboplatin-based IP chemotherapy, its use could positively impact the therapeutic strategy for patients with EOC. However, even though there was no statistical significance in our cohort, the Kaplan-Meier curve seemed to indicate relatively better outcome in cisplatin-based IP chemotherapy group, compared with patients receiving carboplatin-based IP chemotherapy or IV chemotherapy. We deemed that if the size of the cohort is large enough, significant difference might be observed.
 XML Download
XML Download