

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes is a serious threat to population health. The global prevalence of diabetes has nearly doubled (from 4.7% to 8.5%) in the adult population since 1980 (1). More than 50% of cases of acquired blindness, chronic renal failure requiring renal replacement therapy, and non-traumatic limb loss are related to microvascular complications of diabetes. Diabetes is closely related to various cardiovascular diseases, including coronary arterial disease, stroke, peripheral arterial disease, and cardiomyopathy, ultimately leading to death. In the US, the estimated prevalence of diabetes was 12% to 14% among adults aged 20 years or older in 2011–2012 depending on the criteria used. The percentage of people with diabetes and HbA1c < 7.0% was slightly declined from 52.2% in 2007 to 50.9% in 2014 (2). About 4.8 million (13.7%) Koreans aged 30 years or older had diabetes in 2014. With respect to overall glycemic control, 43.5% reached the target level of HbA1c < 7.0% (3).
Diabetes is an archetypal complex chronic disease that is managed overwhelmingly in primary care. In the US, community primary care practice is a logical focal point for implementing strategies to improve diabetes care delivery because primary care physicians (PCPs) treat at least 80% of adults with diabetes (4). There is increasing recognition of the important role that PCPs play in reducing hospital admissions for ambulatory care sensitive conditions (ACSCs) (5). Higher PCP supply is associated with better diabetes care (6) as well as lower mortality due to heart disease, cancer, and stroke (7). Large multispecialty physician group practices with a central role of PCPs have achieved high-quality and low-cost care for patients with chronic diseases (8).
Primary care is the delivery of health care services first encountered by people. It is a discipline in which physicians who see patients personally in the context of family and community continue a doctor-patient relationship over time, coordinate health care resources appropriately, and resolve common health care needs of people (9). A health care system is as strong as its primary care sector, which provides entry into the system for all new needs and problems, provides person-focused (not disease-oriented) care over time, and also provides care for all but very uncommon or unusual conditions (10). Certain characteristics of primary care (e.g., lack of a regular physician, poor continuity of care) have been associated with increased likelihood of making an emergency department (ED) visit (11). Rostering with a patient enrolment model in primary care has been found to be associated with a statistically significant reduction in ED visits in Ontario, Canada (12).
An ED visit may be a marker for limited access to primary medical care, particularly among those with ACSCs (13). Better primary care management of these conditions may improve the process of care and clinical outcomes (14), thus reducing ED visits or hospitalization (15). High-quality in continuity of care is associated with decreased ED use for patients with diabetes (1617). A study at a large ED for patients with history of diabetes has shown that patients with PCPs have significantly better diabetes control compared to those without PCPs even after adjusting for confounding factors (18). Greater continuity of care achieved by rostering is associated with lower use of inpatient and ED services and greater patient satisfaction (19). It has been reported that admission to ED can be used as an indicator for poor quality of diabetes care (20). Use of ED for non-urgent conditions may lead to excessive healthcare spending, unnecessary testing and treatment, and weaker patient-PCP relationships. In the US, one study has reported that, among 700 patients waiting for ED care at a public hospital, nearly half (45%) of these patients have cited that access barrier to primary care is their reason for using ED (21). The use of EDs has increased considerably in Korea. A large proportion (35.2%) of all ED visits in Korea are for non-urgent conditions (22).
The Korean health care system has considerable structural problems, e.g., private-sector dominance, weak infrastructure in primary care, and long-standing fee-for-service payments even though the national universal health insurance system has been in operation since 1989. People can visit medical institutions freely. They can see specialists directly on their own and receive medical treatments by different providers for each episode of care. Therefore, the proportion of Korean adults who have a usual source of care (USC) is extremely low. Only 13.9% of Korean adults have a regular doctor (RD). The most influential factor of having a USC is having a chronic disease and the main (66.1%) reason for not having a USC is seldom becoming ill (23).
Whether those having (vs. not having) a RD would use more health care resources because they are likely to become ill is currently unclear. In this study, the target population of interest was narrowed to diabetic adults to minimize confounding effects during study design. The aim of the present study was to find the current status of having a USC in Korean diabetic adults and identify the association of having a RD with the experience of ED visits by analyzing secondary data from 2013 Korea Health Panel (KHP) survey.
MATERIALS AND METHODS
Data source
KHP data were collected from a national database established by a consortium of the Korea Institute for Health and Social Affairs and National Health Insurance Corporation. KHP used stratified multistage probability sampling according to region and residence in order to select nationwide subjects from the 2005 Korea Census (24). The data were initially collected from 7,009 households and 21,283 individuals in 2008, with 5,200 households and 14,839 individuals remaining in 2013.
Sample selection process
Among 14,839 participants in the 2013 KHP survey, 11,999 were 18 years or older. They were eligible to participate in the appendix survey that contained items about USC. There were 11,300 actual participants in the appendix survey (699 non-participants, 5.8%). Among these participants, 1,016 reported that they had diabetes as a chronic disease (E10–E14 by the 10th revision of the International Classification of Disease [ICD]). Three panels were additionally excluded because they responded vaguely about their usual place of care. Finally, 1,013 survey respondents were included for analysis in this cross-sectional study (Fig. 1).

Measurement
Sociodemographic variables
To interpret study results easily, sociodemographic variables were categorized into several groups: age (18–49, 50–64, and ≥ 65 years), marital status (married, divorced/separated/widowed, and unmarried), education (0–6, 7–12, and ≥ 13 years), and types of health insurance (employed, self-employed, and Medical Aid). Household income was divided into five quintile groups.
Self-rated health (SRH) variables
Subjective health status was rated on a 5-point Likert scale (excellent, good, moderate, poor, and very poor) on the survey. It was merged into a 3-point Likert scale (good, moderate, and poor) to be included as a control variable in logistic regression models.
Charlson comorbidity index (CCI)
To adjust for health status of the study population objectively, CCI, a method to categorize comorbidities of patients based on ICD diagnosis (25), was used in this study. It was developed to predict the one-year mortality among 604 patients based on comorbidity data obtained from a hospital chart review in a single US hospital (25). Each comorbidity category had an associated weight (from 1 to 6). The sum of all weights resulted in a single comorbidity score for a patient. A score of zero indicated that no comorbidity was found. The higher the score, the more likely the predicted outcome would result in mortality or higher resource use. Over time, there have been changes to CCI presented in different research studies. The original index was developed with 19 categories. However, it has been modified to 17 categories (26). The list of specific diagnosis codes has been updated to be consistent with ICD-10 coding (27). In this study, three categories were excluded to calculate CCI score because diagnostic codes for end organ damages of diabetes and moderate or severe liver diseases were not provided in the KHP data. Diabetes (E10–E14) is a disease of the study population. Thyroid cancer (C73) was excluded from the malignancy category because most thyroid cancers were over-diagnosed. Five year relative rates of survival for thyroid cancer were 100.1% and 100.4% in regional and localized tumors, respectively, which comprised 97.1% of the increase in the incidence of thyroid cancer during 2006–2010 in Korea (28) (Table 1). CCI scores were transformed into three groups (0, 1, and 2+) for analysis.
Table 1
Diagnostic codes for calculating CCI score based on 2013 KHP data

Three categories are not included in the above CCI score calculation, because diagnostic codes for end organ damages of diabetes and for moderate or severe liver diseases are not provided in the KHP data, and diabetes (E10–E14) is a disease of the study population. Thyroid cancer (C73) is excluded from the malignancy category.
CCI = Charlson comorbidity index, KHP = Korea Health Panel, ICD-10, the 10th revision of the International Classification of Disease.
Variables of interest
Six key variables related to USC were from two items regarding a usual place (“Do you have a medical institution that you usually visit when you are ill or when you are trying to get a medical check-up or consultation?” and “What is the type of medical institution you usually visit?”) and 4 items regarding a RD (“Do you have a medical doctor who you usually see when you are ill or when you are trying to get a medical check-up or consultation? [first-contact]”, “How long has it been since you first saw the medical doctor? [longitudinal relationship]”, “Does the medical doctor solve almost all the common health problems that you have? [comprehensiveness]”, and “Does the medical doctor appropriately introduce you to health care facilities and providers for your health? [coordination]”). Comprehensiveness and coordination were rated on a 5-point Likert scale. Whether having a RD or not was used as one dependent variable to identify sociodemographic factors associated with it. It was also used as a key independent variable to confirm the statistical significance of its association with having ED visits within the last year. There were several questions about ED visits in the KHP survey questionnaire, including date of visits, types and locations of medical institution, methods of transportation, time lengths of transportation to and stay in ED, reasons for ED visits, and etc. But our concern in this study was on ED visits itself, not on any specific reason for ED visits. Primary independent variables of interest related to a RD included types of USC (a RD, only a place, and not having a USC), types of medical institution that RDs worked for (community public/private clinics, community hospital, and university hospital), and primary care attributes (comprehensiveness, coordination, and longitudinal relationship) that patients experienced from their RDs.
Statistical analysis
Types of USC (a RD, only a place, and not having a USC) in adults (18 years or over) with diabetes were analyzed descriptively to show distributions by sociodemographic variables, health status variables, and variables of interest using χ2 tests or Mantel-Haenzel χ2 tests for trend. Distributions of primary care attributes (comprehensiveness, coordination, and longitudinal relation) that patients experienced from their RDs by types of medical institution were analyzed using Mantel-Haenszel χ2 test or one-way analysis of variance (ANOVA). Multiple logistic regression analyses were used to identify sociodemographic factors associated with having a RD as a USC and calculate adjusted odds ratios (ORs) of characteristics of RDs (having vs. not having a RD in model 1, types of USC in model 2, types of usual places in model 3, and three primary care attributes in models 4–6) for an experience of ED visits while controlling for sociodemographic and health status variables. Statistical analyses were performed with SAS version 9.4 software (SAS Institute, Cary, NC, USA). Statistical significance was set at P ≤ 0.05.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul St. Mary's Hospital at The Catholic University of Korea (approval No. KC15QISI0089) with a waiver for informed consent because the data were obtained from a public database (https://www.khp.re.kr:444/).
RESULTS
Based on the 2013 KHP survey, the crude prevalence of diabetes was 9.0% in Korean adults aged 18 years or over.
Sociodemographic characteristics of adults with diabetes by types of USC
Percentages of adults with diabetes having a RD, having a place only, and those not having a USC were 41.3%, 28.1%, and 30.6%, respectively. The older the age group, the higher the rate of those having a RD. The younger the age group, the higher the percentage of those not having a USC (P = 0.044 for trend). The higher the CCI score, the higher the percentage of those having a RD (P = 0.001 for trend). However, there was no significant difference in percentage of those having a RD based on sex, marital status, education, household income, types of health insurance, subjective health, types of medical institution that a RD worked for, or experience of ED visits within the last year. Among diabetic adults who had a RD, the most common type of medical institution their RDs worked for were private community clinics (63.0%) (Table 2).
Table 2
Sociodemographic characteristics of Korean adults aged 18 years or over with diabetes by types of usual source of care based on 2013 KHP data

Data were analyzed using the χ2 test.
KHP = Korea Health Panel, DM = diabetes mellitus, RD = regular doctor, ED = emergency department, CCI = Charlson comorbidity index, USC = usual source of care.
*It means a physician practicing at a place as a USC. †Mantel-Haenszel χ2 test. Cross-sectional weights were applied for percentages and P values. ‡It does not contain scores for diabetes, end organ damage by diabetes, moderate or severe liver disease, and thyroid cancer. §On a five-point Likert scale, two positive (excellent and good) and two negative (poor and very poor) responses were merged into one positive (good) and one negative (poor) response.
Primary care attributes of RDs by types of medical institution
Among adults with diabetes who were age 18 years or over and had a RD, those having positive experience regarding primary care attributes of their RDs accounted for 75.4% for comprehensiveness compared to 27.1% for coordination. Longitudinal relations between doctors and patients were 7.8 ± 5.5 years in average. There was no significant difference in primary care attribute by types of medical institution that RDs worked for (Table 3).
Table 3
Primary care attributes that Korean adults (≥ 18 years) with diabetes experience from their RDs by types of medical institution based on 2013 KHP data

Data were analyzed using Mantel-Haenszel χ2 test for trend.
RD = regular doctor, KHP = Korea Health Panel, SD = standard deviation, ANOVA = analysis of variance.
*Public health center or private local clinic. †On a five-point Likert scale, two positive (excellent and good) and two negative (poor and very poor) responses were merged into one positive (good) and one negative (poor) responses. ‡Data were analyzed using ANOVA. Sample cross-sectional weights were applied for percentages and P values.
Sociodemographic factors associated with having a RD
After controlling for health status variables in multiple logistic regression, those with 13 years or more in education were associated with an increased probability of having a RD (OR, 1.94; 95% confidence interval [CI], 1.13–3.34; P = 0.017) compared to those with 6 years or less in education. Age, sex, marital status, family income, or types of health insurance were not significantly associated with having a RD (Table 4).
Table 4
Adjusted ORs for having a RD by sociodemographic factors in Korean adults aged 18 years or over with diabetes based on 2013 KHP data

Multiple logistic regression analysis. Sample cross-sectional weights were applied.
OR = odds ratio, RD = regular doctor, KHP = Korea Health Panel, CI = confidence interval, CCI = Charlson comorbidity index.
*It does not contain scores for diabetes, end organ damage by diabetes, moderate or severe liver disease, and thyroid cancer. †On a five-point Likert scale, two positive (excellent and good) and two negative (poor and very poor) responses were merged into one positive (good) and one negative (poor) responses.
Adjusted ORs of characteristics of RD for an experience of ED visits within the last year
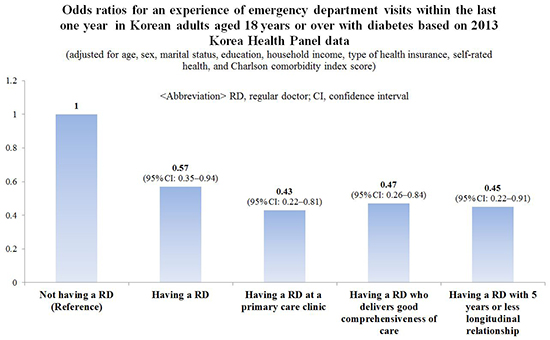
After adjusting for sociodemographic factors and health status variables, those having a RD (OR, 0.57; 95% CI, 0.35–0.94; P = 0.026) (model 1), especially those having a RD of primary care clinic (OR, 0.43; 95% CI, 0.22–0.81; P = 0.010) (model 3) rather than those having a RD of other types of medical institution remained associated with a decrease in an experience of ED visits compared to those not having a RD. Those having a RD (OR, 0.52; 95% CI, 0.29–0.92; P = 0.025) was associated with a decrease in an experience of ED visits compared to those having a place only as a USC (Table 5).
Table 5
Adjusted OR of those having a RD for an experience of ED visits within the last one year in Korean adults aged 18 years or over with diabetes based on 2013 KHP data

Multiple logistic regression analysis. Sample cross-sectional weights were applied.
OR = odds ratio, RD = regular doctor, ED = emergency department, KHP = Korea Health Panel, CI = confidence interval, CCI = Charlson comorbidity index, USC = usual source of care.
*It does not contain scores for diabetes, end organ damage by diabetes, moderate or severe liver disease, and thyroid cancer. †On a five-point Likert scale, two positive (excellent and good) and two negative (poor and very poor) responses were merged into one positive (good) and one negative (poor) responses. ‡Public community clinic or private community clinic.
Adjusted ORs of care attributes of RDs for an experience of ED visits within the last year
After adjusting for sociodemographic factors and health status variables, those having a RD whose care experience was good in comprehensiveness (OR, 0.47; 95% CI, 0.26–0.84; P = 0.010) remained associated with a decrease in an experience of ED visits (model 4) compared to those not having a RD. However, such association was not significant in coordination (model 5). Those having a RD whose longitudinal relationship with patients was 5 years or less (OR, 0.45; 95% CI, 0.22–0.91; P = 0.027) remained association with a decrease in an experience of ED visits. However, such an association was not significant when the longitudinal relationship was 6 years or longer (model 6) (Table 6).
Table 6
Adjusted OR for an experience of ED visits within the last one year by primary care attributes that Korean adults aged 18 years or over with diabetes experience from their RDs based on 2013 KHP data
Multiple logistic regression analysis. Sample cross-sectional weights were applied.
OR = odds ratio, ED = emergency department, RD = regular doctor, KHP = Korea Health Panel, CI = confidence interval, CCI = Charlson comorbidity index.
*It does not contain scores for diabetes, end organ damage by diabetes, moderate or severe liver disease, and thyroid cancer. †On a five-point Likert scale, two positive (excellent and good) and two negative (poor and very poor) responses were merged into one positive (good) and one negative (poor) responses.
DISCUSSION
To the best of our knowledge, this is the first study that analyses the association between having a RD and an experience of ED visits in Korea. This study has several new findings. First, the overall crude prevalence of self-reported diabetes in Korean adults was 9.0%. Among these diabetic adults, only 41.0% had a RD. Second, even in those diabetic adults who had a RD, based on the point of primary care attributes that they experienced from their RDs, coordination was poorer than comprehensiveness in positive response rate (23.7% vs. 75.4%). Third, among diabetic adults, the higher the education level, the higher the percentage of those having a RD. Fourth, among diabetic adults, four features of RD were associated with less likely to have an experience of ED visits within the last year: having a RD (OR, 0.65; 95% CI, 0.35–0.94), having a RD delivering a good comprehensiveness of care (OR, 0.47; 95% CI, 0.26–0.84), having a RD of primary care practice (OR, 0.43; 95% CI, 0.22–0.81), and having a RD who had a longitudinal relationship with the diabetic adults of 5 years or less (OR, 0.45; 95% CI, 0.22–0.91). Fifth, having a RD would be better than having a place only as a USC to less likely have an experience of ED visits in diabetic adults (OR, 0.52; 95% CI, 0.29–0.92) and in the general adult population (OR, 0.71; 95% CI, 0.55–0.93) as reported previously (29).
The 2007 international survey by the Commonwealth Fund has reported that the proportion of adults who have a RD is 100% in the Netherlands, 89% in the United Kingdom, 88% in Australia, 92% in Germany, 89% in New Zealand, 84% in Canada, and 80% in the United States (30). Compared to these countries, the proportion of adults who have a RD is extremely low (13.9%) in Korea (23). This study showed that, even in adults having diabetes as a chronic disease, the percentage of those having a RD was very low.
In addition, Korean patients experience much poorer health care coordination than those in other industrialized countries (31). Regarding the coordination of care that patients experience from their RDs, the percent of those who answered positively is only 34.5% in Korean adults in a previous study (23). In our study, it was only 27.1% in Korean diabetic adults. This implies that patients with chronic condition like diabetes may experience more problems in coordination than the general population. These findings are in sharp contrast with data from other industrialized countries. In the above 2007 international survey (30), proportions of adults who reported receiving coordinated care always or often were 70% in Australia, 69% in the United States, 67% in Canada and Germany, 60% in New Zealand, 58% in the United Kingdom, and 55% in the Netherlands. A 2016 international survey has reported that the percentages of those experienced coordination problem in the past two years were 30% or less in those countries (except 35% in the United States) (32).
Having a usual place of care may not be equivalent to having a RD in terms of benefits. People who report a particular doctor as their USC receive more appropriate preventive care. They have fewer diagnostic tests and prescriptions with fewer hospitalizations and visits to EDs. They are more likely to have more accurate diagnoses than those who either have a particular place or those who have no place at all as their USC (10). In our study, diabetic adults having only a medical institution as a USC without a RD compared to those having a RD rather than those who did not have a USC were significantly more likely to have an experience of ED visits within the last year. This result may imply that the Korean health care system needs to adapt and support patients in coordinating their health needs across multiple specialist services they may rely on to ensure good continuity of care, instead of encouraging further diagnosis and utilization of the large hospital sector (33).
Implementation of policy to encourage patients to use their designated primary care providers can improve the level of adherence to provider among patients. Higher levels of patient adherence are associated with fewer ED visits and hospitalizations (34). An ED visits may be a marker for limited access to primary medical care, particularly among those with ACSCs like diabetes. Patients who have regular PCPs are less likely to report having their last contact with a doctor in an ED than those without a regular PCP (2.5% compared to 14.3%) (15). Certain characteristics of primary care (e.g., lack of a regular physician, unmet needs for healthcare, poor continuity of care, and perceived lack of rapid access to care) are associated with increased likelihood of making an ED visit (35).
It has been reported that physician availability at the primary care clinic during weekends can decrease ED use (35). In addition, patients from clinics offering a larger range of procedures on site have lower ED use (35). Greater comprehensiveness of care by family physicians can predict less use of ED (36). These results are consistent with our results showing that RDs who worked at primary care clinics or whose care was good in comprehensiveness made their adult patients with diabetes less likely to have an experience of ED visits within the last year.
Diabetes outcomes provide a rudimentary but useful lens to analyze the performance of a primary care system. It was estimated that at least 63% of adults with diabetes used primary care settings as a USC in this study. Therefore, quality of these services is paramount in optimal disease management. One of the main strategies to improve quality in primary care is by promoting patient enrolment with a PCP and establishing inter-professional team-based service delivery such as the Family Medicine Group (FMG) model in Quebec, Canada. The FMG model produced reductions in weekly rate of avoidable visits of diabetic patients. After 9 years of reform implementation, there were statistically significant decrease of 2.12 and 2.25 ED visits per 10,000 diabetic patients per week to treat acute diabetes-related complications in urban and rural areas, respectively (37).
In this study, CCI was inferred as a major potential confounder to conceal a statistical significance in the inverse relationship between having a RD and experience of ED visits in bivariate analysis, because having a high CCI score (≥ 2) showed a positive association with having a RD, but revealed to have a high OR (OR, 2.74; 95% CI, 1.41–5.34; P = 0.003) (vs. CCI score = 0) for having an experience of ED visits in multivariate analysis. This study implies that the first 5 years of longitudinal doctor-patient relationship can be more important than the years afterward to decrease avoidable ED visits in adult patients with diabetes, because it is expected that RDs are likely to provide health education and behavior counselling effectively during the initial stage of disease.
Our study has some limitations. First, the causal relationship between having a RD and an experience of ED visits could not be inferred from our study results because this study had a cross-sectional design. In the future, if data regarding a RD are aggregated more than 2 waves repeatedly, a longitudinal analysis can be performed to find the effect of having a RD on various health outcomes including an experience of ED visits. Second, CCI scores calculated and used to control health status in this study might have unavoidable bias because the KHP survey data only had simple 3-digit diagnostic codes (the first digit was alphabet while the second and third digits were numeric), although it was compatible to the ICD-10 coding system. To compensate this weakness, SRH was added as another health status variable. SRH is consistent with objective health status. It can serve as a global measure of health status in the general population (38). Third, there might be reliability problems in the diagnosis of diabetes because it was made by participants' self-reports without differentiating type 2 from type 1 diabetes. However, self-reported diabetes was high in accuracy in adult populations. It is an accurate measure for the prevalence of diabetes. It has specificity of 84%–97% and sensitivity of 55%–80%. It is > 92% reliable over time (39).
In summary, among Korean adults with diabetes, the percentage of those having a RD was very low. After adjusting for health status, having a RD was positively associated with education duration. Even in those having a RD, coordination of care they experienced from their RDs was very poor. Among Korean adults with diabetes, those having a RD, especially those patients whose RD worked at a primary care clinic or delivered good comprehensiveness of care were less likely to have an experience of ED visits within the last year.
In conclusion, health care policies that promote having a RD (rather than having a usual medical institution of care) who delivers high-quality primary care could decrease unnecessary experiences of ED visits by Korean adults with diabetes. This can partly reduce ED overcrowding in Korea.
 XML Download
XML Download