

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pericardiocentesis is an invasive procedure which is usually performed in a patient who has pericardial effusion to resolve the pressure in the pericardial sac. In 1653, Riolanus (1) first described as a trephination of the sternum to relieve fluid surrounding the heart. Due to frequent complications this procedure was out of interest until ultrasound guided technique emerged (2). However, many complications are reported through literature to this day (345). Herein, we report a case of iatrogenic tension pneumopericardium, which exhibit impending cardiac arrest.
CASE DESCRIPTION
A 70-year-old male presented with severe dyspnea and general weakness on March 8, 2013. He was referred from a local hospital for pericardiocentesis and further work-up due to a large pericardial effusion. He had a past medical history of ischemic stroke 15 years prior to his visit to the hospital and of syncope a day before his visit to the hospital.
The vital signs of the patient in the Emergency Room (ER) were as follows: blood pressure of 163/93, heart rate of 135 beats per minute, respiratory rate of 30 breaths per minute, body temperature of 37.0°C, and oxygen saturation of 91%. The patient had distended neck veins and muffled heart sounds but did not have low blood pressure. Echocardiography was performed by an emergency physician, and a right ventricle (RV) free wall collapse in was observed in the diastolic phase. An emergency pericardiocentesis was indicated, and it was performed by a subxiphoid approach. Approximately 700 mL of serous effusion was drained through a catheter; the patient’s heart rate dropped to 110 and his blood pressure was maintained above 130. The follow-up echocardiography showed the absence of RV wall diastolic collapse. A water-sealed chest tube bottle was connected at the end of the catheter for further drainage.
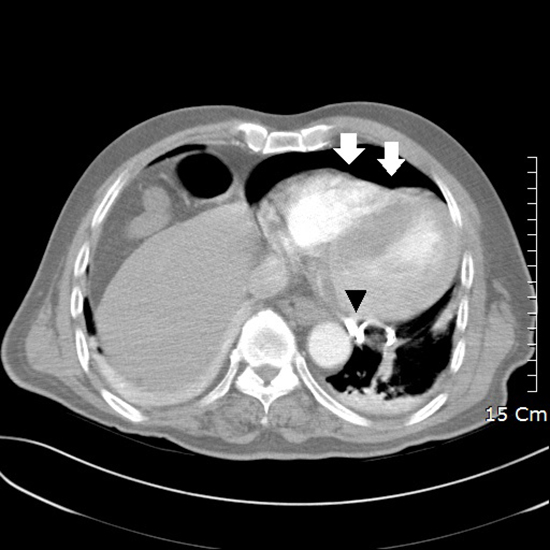
The patient was transferred to a computerized tomography (CT) room for a chest CT to examine the cause of his pericardial effusion. Before he left the ER, his vital signs were stable and he was alert. After the patient returned to the ER from the CT room, his heart rate fell to 30, and he exhibited impending cardiac arrest. An intravenous dose of 0.5 mg atropine was given, and the patient was hydrated with crystalloid solution. The patient’s chest CT confirmed tension pneumopericardium, and imaging showed that pericardial air was compressing the right ventricle and that the catheter tip was placed behind the left ventricle (LV) (Fig. 1). Approximated 500 mL of pericardial air was evacuated rapidly through the previously implanted catheter, and the patient’s vital sign became stable. The patient was admitted to the intensive care unit and subsequently transferred to a long-term care hospital.
DISCUSSION
Pneumopericardium is defined as the presence of air inside the pericardial space. In 1910, Wenkebach first described the X-ray findings of pneumopericardium, and in 1967, Cimmino (6) described the diagnostic features of pneumopericardium. In a review of the literature, Toledo et al. (7) classified the etiology of pneumopericardium into four categories: iatrogenic, pericarditis, fistula formation between the pericardium and an adjacent air-containing organ, and trauma. Additionally, Cummings et al. (8) reported that trauma and positive pressure ventilation are the major causes of pneumopericardium. Iatrogenic cases of pneumopericardium associated with various procedures, such as thoracentesis, paracentesis, poststernal bone marrow aspiration, postcauterization of esophageal webs, pericardiocentesis, radiofrequency ablation, and pacemaker insertion, have been reported (7910).
Usually, pneumopericardium presents as chest pain and dyspnea. If the patient has tension pneumopericardium, physical examination may show tachycardia, distended neck veins, and hypotension. In 1844, Bricheteau was the first to describe the mill wheel murmur in auscultation, which is a characteristic churning or splashing auscultatory sound due to blood mixing with air in the pericardial sac. A chest X-ray showing air surrounding the heart and the “small heart sign” suggests tension pneumopericardium (11). Pericardial air can be mistaken for mediastinal air, but the air in the pericardial sac does not rise above the pericardial reflection of the proximal great vessels. Also a chest X-ray taken from the decubitus position may show a shift of air if the air is in the pericardium, but mediastinal air does not shift (12). A small amount of air in the pericardial sac is indistinguishable by plain chest X-ray but can be detected by CT scan. Bedside echocardiography in the ER is an alternative method for detecting air in the pericardial sac, but a large amount of air may hinder the penetration of the ultrasound beam, so diagnosis by this method may be challenging.
Tension pneumopericardium requires immediate evacuation of the pericardial air. The traditional blind subxiphoid approach can still be used for pericardiocentesis in emergency situations. The needle should be placed 1 cm inferior to the left xiphocostal angle at a 30-degree angle to the skin. It should be aimed toward the left shoulder and advanced while maintaining negative pressure (13). After the insertion of the catheter, a drainage tube is connected to a water sealed device. In our case, a conventional chest tube bottle was used, and during transportation to the CT room, the drainage device was not clamped. There is one possible explanation for this case of iatrogenic pneumopericardium. During the transfer, the water in the bottom of the bottle could have swung back and forth. Originally, the tube connected to the catheter would have been sealed with water, but this swinging motion would have provided the opportunity for air to enter the catheter and, subsequently, the pericardial sac.
Iatrogenic pneumopericardium is rarely reported after pericardiocentesis, but it can lead to tension pneumopericardium, which is a life threatening condition. Physicians should be aware of this serious complication of pericardiocentesis and take extra precautions in handling drainage devices because this iatrogenic complication can lead to cardiac arrest and a medical dispute.
 XML Download
XML Download