

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pulmonary artery sarcoma (PAS) is an extremely rare, malignant neoplasm. The etiology is unknown, and the disease results in significant morbidity and high mortality. Without surgical intervention, the mean survival time after diagnosis is 1.5 months (1). There have been few reports of the long-term results of PAS treatment, especially in Asia. Due to its nonspecific clinical manifestations, including dyspnea on exertion, chest pain and cough, PAS is easily misdiagnosed as a pulmonary vascular disease such as pulmonary thromboembolism (PE) (23). These types of misdiagnoses can delay proper treatment. Therefore, the ability to distinguish PAS from PE is an important issue (45).
Radiation therapy and chemotherapy have been recommended for some patients with PAS (6), although the efficacy of these treatments is largely unproven. Thus, surgical resection remains the mainstay for PAS treatment, as complete resection offers the only chance for a potential cure (7) and prolonged survival (68910111213). Although TNM staging reflects prognosis and is used as the standard for many cancers, there is no standard TNM staging system for PAS. Instead hemodynamic influence may affect to prognosis of PAS. The origination of PAS from the pulmonary trunk and/or main pulmonary artery leads to right heart failure as the main cause of death due to obstruction of the right ventricular outflow track (RVOT). There have been some case reports of PH due to PAS (411), but none of these studies reported the correlation between PH and prognosis.
Interestingly, the largest series of PH due to PAS were reported by pathologists and surgeons (1415). In our study, from a physician’s point of view, we report our experience with 20 PAS patients over a period of 14 years at the Asan Medical Center in Seoul, Korea. We analyse demographics, other baseline characteristics, echocardiographic findings, diagnostic and treatment modalities, prognostic factors, postoperative outcomes, and long-term results. We also report on the influence of hemodynamics on PAS prognosis.
MATERIALS AND METHODS
Study patients
We retrospectively reviewed the clinical records of all patients with a pathological diagnosis of PAS at the Asan Medical Center in Seoul, Korea between January 2000 and December 2014. Patients with insufficient medical data were also excluded. Diagnosis was confirmed by histological examination and immunohistochemistry. Although some reviews have designated PAS as a primary cardiac sarcoma (1617). Here we describe only primary PAS and not cardiac-origin sarcoma. A total of 20 patients were included in this study.
Data collection
Baseline data, including age at diagnosis, sex, duration of symptoms until diagnosis, symptoms at diagnosis, smoking history, diagnostic and treatment modalities, operation records, and pathologic findings were collected from medical charts. Echocardiographic studies were performed to identify PH. Transthoracic echocardiography (TTE) is the standard technique for diagnosing PH (18). European guidelines define the echocardiographic diagnosis of PH as “likely” when the tricuspid regurgitation velocity (TR Vmax) is > 3.4 m/s or the pulmonary artery systolic pressure is > 50 mmHg with/without additional echocardiographic variables (19). We diagnosed PH when TR Vmax was > 3.4 m/s. Other echocardiographic measurements, such as the ejection fraction of the left ventricle, the presence of an inferior vena cava plethora or a pericardial effusion, were also checked. Survival status and date of death were determined based on medical charts and the expiration date of the Korean national health insurance service. Patients were only classified as deceased if they died during the follow-up period. All other cases, including cases lost to follow-up, were censored.
Statistical analysis
All values were expressed as the median (range) for continuous variables and as the number or percentage for categorical variables. Survival analysis was performed using the Kaplan-Meier method, and the log-rank test and Cox proportional hazard model were used for univariate and multivariable analysis respectively. Variables used in multivariable analysis included age, sex and variables showing P value < 0.10 in univariate analysis (e.g. Receipt of chemotherapy and post-treatment PH). A P value of < 0.05 was considered to be statistically significant. Analysis was performed using PASW Statistics 18 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
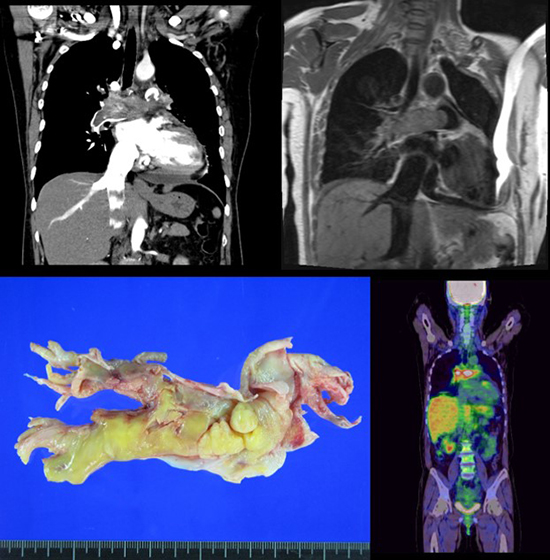
Of the 20 patients included in the analyses, 10 (50%) were male, and the median age was 54 years (range, 33–75 years) at diagnosis. Patient characteristics are summarized in Table 1. The median duration between symptom onset and diagnosis was 2 months (range, 0–28 months). Disease evaluation included computed tomography (CT; n = 20), TTE (n = 19), magnetic resonance imaging (MRI; n = 10), lung perfusion scan (n = 12), and 18F-fluorodeoxyglucose positron emission tomography (18FDG-PET; n = 17). Ten patients (50%) had a presumptive diagnosis of acute or chronic PE and received anticoagulation therapy preoperatively. Tumour tissues were directly obtained by surgery (n = 13), open biopsy (n = 2), endobronchial ultrasound transbronchial needle aspiration (EBUS-TBNA; n = 2), percutaneous needle biopsy (PCNA; n = 2), or pulmonary angiography with endovascular biopsy (n = 1). There were no statistically significant differences in survival by histologic subtype. PH was observed in 12 patients before treatment (median TR Vmax 3.8 m/s, range 3.2–4.4 m/s) and in 6 patients after treatment (median TR Vmax 3.75 m/s, range 2.9–4.0 m/s). Right ventricular dysfunction was observed in 11 patients before treatment and 8 patients after treatment. The bilateral pulmonary arteries and/or pulmonary trunk were affected in 60% of patients, while the unilateral pulmonary artery was involved in 30% of patients. The tumour extended to the heart in 5 patients.
Table 1
Characteristics of the pulmonary artery sarcoma patients (n = 20)

Treatment
Seventeen patients (85%) underwent surgery, although only five of these (30%) received complete resections. Surgery for PAS included pneumonectomy (n = 4), lobectomy (n = 4), pulmonary endarterectomy/tumour debulking with or without pulmonary artery reconstruction (n=8), and heart/lung transplantation (n = 1). The choice of procedure was dependent on factors such as tumour location and distal extension. There were three peri-operative deaths, two of which had unresolved severe PH after surgical resection, and one of which had acute respiratory distress syndrome after surgery. Eleven patients (55%) received post-operative treatment, 3 (15%) received chemotherapy, 5 (25%) received radiotherapy, and 3 (15%) received chemotherapy plus radiotherapy. The remaining 2 patients (10%) had inoperable disease involving both pulmonary arteries and received only chemotherapy, as complete resection was not possible. These patients were still alive at follow-up (22 and 37 months, respectively). One patient refused treatment and died due to disease progression.
Survival
The median overall survival (OS) for all 20 study patients was 24 months. We used Cox proportional hazard model analysis to identify factors influencing mortality (Table 2). We found that post-treatment PH was significantly associated with increased mortality (HR 9.501, 95% CI= 1.794–50.32; P = 0.008) (Fig. 1), while chemotherapy was negatively associated with mortality (HR 0.102, 95% CI 0.013–0.826; P = 0.032) (Fig. 2). Post-treatment PH was significantly associated with increased mortality in multivariable analysis (HR 5.946, 95% CI 1.551–31.7; P = 0.037) (Table 3). There were no significant differences in survival between patients who were misdiagnosed with PE and those who were not. There is no standard TNM staging system for primary PAS at present. Two previous studies have used their own staging system, described in Table 4 (1520). There were no statistically significant differences in mortality between these two staging systems in our current patients. The longest surviving patient (188.7 months) had pulmonary artery reconstruction and pulmonary valve replacement along with postoperative chemotherapy and radiotherapy. He developed thyroid metastases 2 years later and adrenal gland metastasis 6.7 years later, both of which were treated with sequential metastasectomies (21).
Table 2
Univariate Cox proportional hazards analysis of variable factors for mortality in the pulmonary artery sarcoma patients
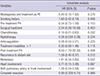
Fig. 1
Kaplan-Meier survival curve of pulmonary artery sarcoma patients with or without pulmonary hypertension after treatment.

Fig. 2
Kaplan-Meier survival curve of pulmonary artery sarcoma patients with or without chemotherapy.

Table 3
Multivariable Cox proportional hazard analysis of prognostic factors for mortality in the pulmonary artery sarcoma patients
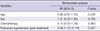
Table 4
The number of PAS patients for each stages. Pulmonary artery sarcoma stages defined in two previous studies

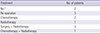
Recurrence
Twelve (60%) patients had recurrence or disease progression (median recurrence-free survival, 15 months; range, 3–45 months). Lung or locoregional (lymph nodes, chest wall) recurrence was observed in seven (60%) patients, while distant and/or multiple metastases (brain, thyroid, bone, adrenal gland, distant skin, muscles) were observed in five (40%) patients. Eleven patients (91.6%) received one or more treatment. Table 5 summarizes the treatments given after recurrence. Four patients died due to disease progression. Chemotherapy performance (HR 0.331, 95% CI 0.102–1.069; P = 0.053), and lung involvement (HR 5.394, 95% CI 1.423–20.454; P = 0.006) were correlated with recurrence in univariate analysis but not in multivariable analysis.
DISCUSSION
There have been few reports concerning the long-term results of PAS treatment. The 20 patients evaluated in this study constitute one of the largest single-centre studies in the published literature to date in Asia. The long-term outcomes of all patients are presented. The reported median age at PAS diagnosis (48.4–57.0 years) (610131520), and median OS (8-36 months) after treatment (101520), were similar to our study.
Due to absence of a gold standard diagnostic test, multiple tests are used to diagnose PAS. Chest radiography findings are not specific to PAS (22). Although CT provides more information on the anatomy of the intravascular process, it cannot easily differentiate between PE and PAS (22223). CT findings that favour PAS diagnosis include a heterogeneous enhancement of the mass occupying the main or the proximal pulmonary artery, and extravascular spread of the lesion (24). Echocardiography is a readily available tool for detecting PAS. The sensitivities of TTE and transoesophageal echocardiography in detecting these primary masses are reported as 93% and 97%, respectively (25). PAS patients may show a bulging mass impacted in the main pulmonary artery (MPA) on echocardiographic examination, which differs from the linear mass usually found in acute PE. The involvement of the pulmonary valves and attachment to the RVOT are other differential findings that suggest a malignant mass with infiltration (52627). When thrombi are visualized in the MPA of patients with acute PE, they are usually located in its distal part near the bifurcation and often extend to a pulmonary artery (2829). Despite the findings mentioned above, echocardiography is non-diagnostic for PAS. But TTE has no harmful effect, short-term follow-up echocardiographic examinations represent an attractive method for differential diagnosis (5). Gadolinium-enhanced MRI can be helpful in distinguishing a soft tissue mass from a thrombus by lesion enhancement (2630). Some experts have suggested that further investigation with MRI is warranted in patients who do not respond to initial anticoagulation (15). Ventilation/perfusion scintigraphy is used for assessing the likelihood of PE but it is not helpful for distinguishing PAS from thromboembolic disease (3132). 18FDG-PET plays an important role in the evaluation of pleuropulmonary neoplasms(223) and is a non-invasive method for differential diagnosis of diseases showing a contrast-filling defect in the pulmonary artery by CT angiography, as blood thrombi do not take up 18F-FDG but malignant tumours such as PAS do (2233334). In our study, malignancy was preoperatively suspected in 12/17 patients on the basis of PET (sensitivity 70%) and 9/10 patients on MRI (sensitivity 90%). Suspicion is justified when CT indicates a filling defect in the pulmonary artery that looks atypical for PE or when anticoagulant treatment fails to alleviate pulmonary perfusion abnormalities and systemic symptoms. 18FDG-PET, MRI or short-term follow-up TTE can help with differential diagnosis in this situation.
In our centre, tumour tissues are mostly obtained intraoperatively but can also be obtained by PCNA, EBUS-TBNA, or angiography. Some studies have reported the use of EBUS-TBNA to differentiate PAS from thromboembolism (35). However, proximal obstruction of the pulmonary arteries by sarcoma or thromboembolic material can cause hypertrophy of the systemic bronchial arteries, increasing the risk of haemorrhage from EBUS-TBNA (36).
Reported histopathologic classifications of PAS vary widely. Fibrous Histiocytoma-type pleomorphic fascicular sarcoma was the most common type of PAS (70%) in a French study (10), pleomorphic-fascicular sarcoma was frequently observed (65%) in an American pathology study (14), and approximately 30% of PAS were undifferentiated sarcomas in another study (37). In primary cardiac sarcomas, histologic grade of the malignancy has the greatest correlation with survival (38). In PAS, however, there were no statistically significant differences in survival by histologic grade, mitotic count, and presence of necrosis except in low-grade myofibroblastic sarcomas (14). In our present study, spindle cell sarcoma was the most common classification (40%) and there were no differences in survival between different histologic classifications in our patient series. The fourth edition of the World Health Organization (WHO) Classification of Tumours of Soft Tissue and Bone was updated in 2013 with immunohistochemical and genetic/molecular data for established tumour types, which might necessitate histopathological reviews of our study data.
In this study, complete surgical resection was only performed in a small number of patients, as PAS usually presents late as a bilateral, advanced disease. The possibility of complete resection did not significantly affect mortality, although definite conclusions are difficult due to the small sample size. According to recent studies, patients treated with chemotherapy or multimodality have increased median survival compared with those treated with monotherapy (920). Our study showed that chemotherapy may confer a survival benefit, but further studies are required to assess the role and regimen of chemotherapy in PAS. The only targeted agent approved for use in soft tissue sarcoma is the tyrosine kinase inhibitor pazopanib (39), but the use of it for PAS has not been reported. In this study, one patient who had progression after chemotherapy (ifosfamide with mesna, Doxorubicin, and Dacarbazine) was administered pazopanib as a second-line chemotherapy. However, we only had one month of follow-up and need more time to sufficiently evaluate its effects.
In our study, long-lasting PH after treatment was associated with poor prognosis. Therefore, we suggest that further studies are required focused on post-operative hemodynamic influences as the main treatment target and development of a staging system.
 XML Download
XML Download