

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The presence of ascites in cirrhotic patients is known to lower the long-term survival (1). Adequate prognostic assessment in these patients is crucial for monitoring the patient and decision-making for future therapeutic options but it is very difficult. The reason is that disease progression was affected by many factors including the degree of hepatic dysfunction, circulatory or renal dysfunction, portal hypertension, the cause of cirrhosis and the recovery of damaging process (2).
To date, Child-Pugh (CP) score (3), Model for End-Stage Liver Disease (MELD) score (4), serum sodium (Na) to MELD score (MELD-Na) (5), and hepatic venous pressure gradient (HVPG) (6) constitute the representative tools to predict mortality in patients with cirrhosis (7, 8). In cirrhotic patients with ascites, CP score has been widely used in clinical practice to estimate survival, but it has some limitations: 1) it does not reflect renal function that is an important prognostic factor especially in decompensated cirrhosis, 2) the cut-off values for continuous variables including bilirubin and albumin are ambiguously decided, and 3) it includes subjective variables such as hepatic encephalopathy and ascites (9). In contrast, MELD score consists of all objective and continuous variables such as serum bilirubin, creatinine and prothrombin time as INR, so that MELD score has advantages over CP score in reflecting both liver and kidney function and in excluding subjective variables. However, because MELD score does not reflect major complications of portal hypertension such as ascites, hepatic encephalopathy and variceal bleeding and patients with low MELD score occasionally show high mortality, MELD score dose not replace CP score completely (10). Since hyponatremia and impaired solute excretion in patients with advanced cirrhosis are also associated with poor outcomes (11), a combined prognostic model of MELD and serum sodium, MELD-Na can provide additional information for predicting mortality, especially in patients with awaiting liver transplantation (5). The increase of portal pressure in cirrhosis is closely associated with poor prognosis, too. The measurement of HVPG is a precise tool to evaluate the severity of portal hypertension and is helpful to predict prognosis (12). However, recent studies of the comparison between HVPG and MELD in patients with decompensated cirrhosis for prediction long-term mortality showed different results (13, 14, 15). Above all, one of the main limitations of these prognostic factors is the lack of evaluation of the nutritional status of cirrhotic patients.
Muscle wasting or sarcopenia which reflects nutritional status is independently associated with mortality and prognosis in cirrhotic patients (16). It can be evaluated by regional analysis of skeletal muscle on a single slice scan of abdominal CT examination, which was highly correlated with corresponding total body skeletal muscle volume of the individual. It is very accessible and highly precise to quantify the skeletal muscle in the body (17, 18). To date, data are insufficient about the prognostic values of sarcopenia in cirrhotic patients with ascites, especially in comparison with other representative predictors such as CP score, MELD score, MELD-Na and HVPG. Therefore, this study was aimed to assess and compare sarcopenia with other prognostic parameters to predict long-term mortality in cirrhotic patients with ascites.
MATERIALS AND METHODS
Patients
Between December 2009 and June 2013, a total of 89 non-critically-ill patients with decompensated cirrhosis were consecutively collected at Hanyang University Guri Hospital. All patients had previous histological confirmation of cirrhosis or a diagnosis of cirrhosis on the basis of standard clinical, biochemical parameters and imaging examinations (19). Refractory ascites is defined also based on the Korean clinical practice guideline for liver cirrhosis (19). All patients had stable hemodynamic parameters and were not active drinkers. We performed this study in a real-life clinical setting, permitting the use of anti-viral agents for viral hepatitis B or non-selective beta blockers for primary or secondary prophylaxis of variceal bleeding. All patients underwent abdominal CT examination within 2 months from laboratory examinations and HVPG. Exclusion criteria were unstable state, absence of ascites, creatinine levels above 1.5 times to upper normal limits, and failure of HVPG measurement. Finally 65 patients were included and analyzed (Fig. 1). Follow-up continued until 31 December 2013.
MELD and MELD-Na
MELD score were calculated for each patient on the day of HVPG measurement. The MELD score was by following equation: 9.57×loge (creatinine [mg/dL])+3.78×loge (bilirubin [mg/dL])+11.2×loge (international normalized ratio, INR)+6.43 (4). The MELD-Na score was calculated by following equation: MELD-Na=MELD+1.59×(135-Na) (5).
HVPG measurement
HVPG was measured by a radiologist with experience in more than 100 HVPG measurements. Under fluoroscopic guidance, a 6 French balloon tip catheter (Arrow International, Inc., Cleveland, OH, USA) was located in the right hepatic vein through the internal jugular vein. Free hepatic vein pressure was measured at a location within 5 cm from the junction of the right hepatic vein and inferior vena cava. After balloon inflation, the wedged hepatic vein pressure was measured at the same location. All the values were measured in three times, and the results were reported as the means of the three measurements. The HVPG was determined by subtraction of the free hepatic venous pressure from the wedged hepatic venous pressure.
Measurement of psoas muscle thickness on CT scan
According to the recent studies, in order to evaluate sarcopenia the psoas muscle area or thickness can be measured on the axial CT scan at the various levels of lumbar spine such as L3 vertebral level (20), L4 vertebral level (21), and at the level of umbilicus (22). These studies showed the good correlations of the psoas muscle mass and clinical outcomes. We measured the thickness of the right psoas muscle, at the level of endplate of L4 vertebra on a single axial portal phase scan of abdominal CT examination: psoas muscle thickness was determined as a largest diameter perpendicular to the longest diameter of psoas muscle including both the psoas major and psoas minor on an axial CT image (Fig. 2). To minimize the possible gender or racial effect on muscle mass measurement we decided to use the psoas muscle thickness by height (PMTH, mm/m) that was defined as each measured value of psoas muscle thickness divided by the height to adjust the stature of the corresponding patient.
At first, the right psoas muscle thickness was measured by the two radiologists independently and the data sets were analyzed for the interobserver agreement. Measurement of PMTH yielded an intraclass correlation coefficient of 0.906 for two observers assessing the same pairs of abdominal CT image. Then, the two radiologists measured the right psoas muscle thickness again in consensus, which was selected for the statistical analyses.
Statistical analysis
Descriptive statistics were produced for demographic, clinical, and laboratory characteristics for this study sample of patients. Quantitative and qualitative variables were expressed as mean±SD (ranges) and number (%), respectively. The correlation between PMTH and different parameters was analyzed by Spearman correlation coefficients. The diagnostic performances of CP score, MELD score, MELD-Na, HVPG and PMTH for predicting 1-yr mortality were evaluated by sensitivity, specificity, and the area under the receiver operating characteristics curve (AUROC). Optimal cutoff values were chosen to maximize the sum of sensitivity and specificity. According to optimal cutoff values, the Kaplan-Meier method with log-rank test was used to calculate survival. To assess the prognostic predictors of long-term mortality, the variables, including sex, age, etiology of cirrhosis, history of variceal bleeding, the degree of ascites, platelet count, serum albumin, serum total bilirubin, prothrombin time (international normalized ratio, INR), creatinine, serum Na, CP score, MELD score, MELD-Na, HVPG and PMTH were used in the Cox regression models and a hazard ratio (HR) of independent predictive factors were obtained. Only the variables significantly associated with the endpoints in univariate analysis were entered in a multivariate model. P value less than 0.05 was significant. Statistical analysis was performed using SPSS 18.0 (SPSS, Inc. an IBM Company, Chicago, IL, USA)
Ethics statement
This study was approved by the institutional review board of Hanyang University Guri Hospital (IRB No. 2014-04-002). The board of hospital approved the study protocol before the initiation of investigation. Informed consent was not obtained because this study was performed by retrospective review of medical records.
RESULTS
Baseline characteristics of patients
The mean age of study patients was 55±9.2 yr with 41 (63.1%) male. The causes of liver cirrhosis were alcohol in 37 (56.9%), viral hepatitis in 17 (26.1%), viral hepatitis and alcohol in 6 (9.3%) and others in 5 (7.7%). Only 3 patients had CP class A; 37, class B; 25 class C, respectively. Mean values of MELD score, MELD-Na, HVPG and PMTH were 12±4.1, 13±4.9, 19±5.2 mmHg, and 16±3.8 mm/m, respectively. Also, the baseline characteristics and the results of biochemical examinations are summarized in Table 1.
The correlation between PMTH and other prognostic variables
The PMTH values had a significant positive correlation with serum Na (r=0.266. P=0.033), and a significant negative correlation with CP score, MELD score, and MELD-Na (r=-0.265, r=-0.253, r=-0.281, respectively, all P<0.05). However, the correlation between PMTH and HVPG was not significant (Table 2). These findings suggested that PMTH may not be associated with the degree of portal hypertension but with that of liver dysfunction.
The diagnostic performances of CP score, MELD score, MELD-Na, HVPG and PMTH for predicting 1-yr mortality of cirrhotic patients with ascites
After the index CT examination, 19 (29.2%) patients died during a mean follow-up period of 20 (1-49) months. The causes of death were hepatic encephalopathy (n=7), hepatorenal syndrome (n=6), variceal bleeding (n=3), ischemic enteropathy (n=1), and septic shock (n=2). An ischemic enteropathy was developed due to the main portal vein and superior mesenteric vein thrombosis as a complication of cirrhosis, not associated with hepatocellular carcinoma.
The AUROCs of CP score, MELD score, MELD-Na, and PMTH for predicting 1-yr mortality were 0.777, 0.769, 0.800, and 0.833, respectively (all P<0.01). However, the diagnostic performance of HVPG was not significant with 0.695 of AUROC (P=0.053) (Table 3). The differences between PMTH and other prognostic variables were not significant (Fig. 3). The best cut-off value of PMTH to predict 1-yr mortality was 14 mm/m with 90.0% of sensitivity, 71.8% of specificity (P<0.001) (Table 3).
Survival analysis
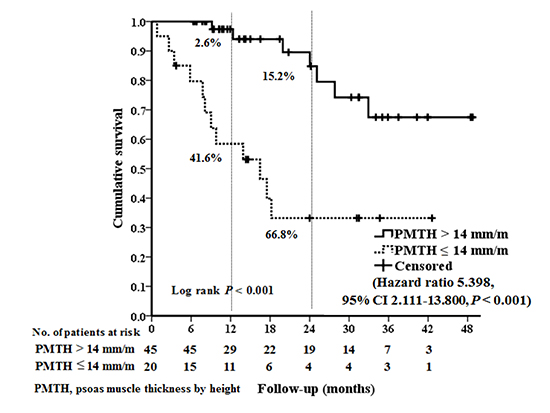
The mortality rates of all patients at 1-yr and 2-yr were 15.0% and 33.2%, respectively. The median survival periods in patients with PMTH≤14 mm/m were 16 (95% confidence interval, 7-26) months. The mortality rate at 1-yr and 2-yr were 2.6% and 15.2% with PMTH>14 mm/m, and 41.6% and 66.8% with PMTH≤14 mm/m (P<0.001) (Fig. 4). During follow-up, 12/20 (60%) patients with PMTH≤14 mm/m were dead (varcieal bleeding in 3, hepatic encephopathy in 5, hepatorenal syndrome in 1, ischemic enteropathy in 1, and septic shock in 2), whereas only 7/45 (15.6%) patients with PMTH>14 mm/m were dead (hepatorenal syndrome in 5, hepatic encephopathy in 2).
In the univariate analysis for death of cirrhotic patients with ascites, the presence of refractory ascites (P=0.010), INR (P=0.009), Na (P=0.005), CP score (P=0.015), MELD score (P=0.014), MELD-Na (P=0.001) and PMTH (P=0.001) were related with long-term mortality. In sex- and age-adjusted multivariate analysis using Cox regression model using refractory ascites, Na, CP score, MELD score, PMTH, only PMTH (HR, 0.812; 95% CI, 0.684-0.965, P=0.018) were significant (Table 4). Especially, the mortality in cirrhotic patients with PMTH≤14 mm/m was 5.4 times to that with PMTH>14 mm/m (HR, 5.398; 95% CI, 2.111-13.800, P<0.001).
DISCUSSION
The results of our study demonstrated clearly that the measurement of PMTH at the level of L4 lower endplate is very useful to predict long-term mortality. In cirrhotic patients with ascites, decreased PMTH was associated with higher mortality, independent of well-known prognostic indicators such as CP score, MELD score, MELD-Na, and HVPG.
The development of decompensation in cirrhosis is associated with poor prognosis (7). Certainly, common complications easily recognized in cirrhotic patients such as overt ascites, hepatic encephalopathy, variceal hemorrhage, and renal failure were associated with shortened survival. It is well-known that the prognostic factors in cirrhotic patients with ascites are related to the degree of underlying circulatory or renal dysfunction, portal hypertension, and liver dysfunction (6, 7). Considering these factors, the prognostic models including CP score, MELD score, MELD-Na, and HVPG have been widely used (6, 7). However, these models did not include nutritional status of the patients. Various measuring tools for nutritional status have been already introduced independent of CP class (23, 24, 25, 26). However, these tools are not optimal indices for nutritional status in terms of availability, reproducibility, practicality, and prognostic performance. Muscle wasting or sarcopenia, reflecting the nutritional status, was also a common complication related to survival, quality of life, and response of stressor in cirrhotic patients (27).
There are three conventional methods to evaluate muscle mass; dual energy x-ray absorptiometry, bioelectric impedance measurement, and cross-sectional imaging such as CT scan and magnetic resonance image (28, 29). In the literature, the assessment of the psoas muscle mass was found very accessible and highly precise to quantify the skeletal muscle in the body (17, 18). The psoas muscle can be easily identified and easily measured on a CT scan, because it is surrounded by retroperitoneal fat tissue and vertebra, and is not susceptible to the compression of ascites or hepatosplenomegaly. In the literature the level of the measurement of psoas muscle mass was recommended as a 5 centimeter above L4-L5 interspace. However, in the clinical situation, to find the level is not simple. So, we preferred level of umbilicus because it was very easy to recognize in abdominal CT scan. It is normally located on the level of L4 vertebra. By the way, in a patient with large amount of ascites the umbilicus was noted lower or higher level. To find an easier, simpler and reproducible method of measurement of psoas muscle mass, we selected the level of L4 lower endplate. It was usually corresponding to the umbilicus level. The sacralization of the L5 vertebra, lumbarization of S1 vertebra, lumbar rib or hypoplastic 12th rib may cause of error of selection of the vertebral level, so we regarded L4 as the last vertebra of its upper endplate located above iliac crests.
A major finding of this study was that the mortality risk is about 5-fold higher in cirrhotic patients with PMTH≤14 mm/m than in those with PMTH>14 mm/m during a mean follow-up period of 20 months. In this study the main causes of death in patients with sarcopenia were hepatic encephalopathy and septic shock. This was also consistent with the previous study that found correlation between protein malnutrition and sepsis in cirrhotic patients (30).
In contrast with a previous study (16), our result showed that sarcopenia evaluated by PMTH was correlated with the degree of liver dysfunction which was evaluated with conventional scores of CP, MELD, serum Na, MELD-Na but not correlated with portal hypertension or HVPG and other biochemical parameters such as serum albumin, bilirubin, INR, and creatinine. HVPG has been known to be a significant prognostic factor in cirrhosis but in this study HVPG did not reach the significant prognostic value (P=0.053). The possible explanation is that almost all enrolled patients had decompensated cirrhosis with ascites (clinical stage of 3 or 4) and in such a more advanced stage HVPG might play a limited role in predicting mortality (13). Interestingly, prognostic accuracy of PMTH for predicting long-term mortality was higher than but statistically similar to the performance of CP score, MELD, MELD-Na. It is needed to evaluate whether adding of PMTH on these widely-used prognostic parameters can increase the performance of mortality prediction in cirrhotic patients with ascites.
A recent study showed PMTH was associated with mortality in patients with refractory ascites and MELD score≤25 (22). Similarly, our patients had all MELD score below 20 and PMTH and presence of refractory ascites was predictive of long-term mortality, independent of other prognostic factors. Especially, in subgroup of refractory ascites, only PMTH was an independent risk factor of mortality, raising a possibility that refractory ascites is closely related to sarcopenia in respect of increased mortality. The treatment of patients with refractory ascites is very difficult and limited, and in some cases, transjugular intrahepatic portosystemic stent have been performed. Recently, a study showed that improvement of survival after transjugular intrahepatic portosystemic stent was associated with the reversal of sarcopenia evaluated by psoas muscle thickness (21). This result supported that possibility.
This study has several limitations. Firstly, it was a retrospective study of relatively small number of patients conducted in a single institution. To overcome this limitation, we consecutively collected subjects for the study with long-term follow up data. Also, other representative prognostic predictors including CP score, MELD score, MELD-Na were evaluated together with PMTH. Secondly, we measured empirically the thickness of the right psoas muscle at the level of L4 lower endplate level. However, the analysis of psoas muscle using single slice of the abdominal CT scan was highly correlated with corresponding total body skeletal muscle volume. CT is mainly a method for evaluation of disease progression in cirrhotic patients. Measurement of psoas muscle thickness using CT scan was easier, simpler, and reproducible. Furthermore interobserver variation was small and acceptable.
In conclusion, measurement of PMTH at the level of endplate of L4 was a useful objective and continuous variable for the evaluation of sarcopenia in cirrhotic patients with ascites. It was associated with long-term mortality independent of other well-known prognostic predictors with comparable accuracy.





 XML Download
XML Download