

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The introduction of tumor necrosis factor (TNF) inhibitors has revolutionized the management of chronic inflammatory diseases, including rheumatoid arthritis (RA) and ankylosing spondylitis (AS) (1). Many randomized clinical trials have found that TNF inhibitors, including a mouse-human chimeric monoclonal antibody (infliximab), a soluble TNF receptor immunoglobulin G fusion protein (etanercept), and a fully humanized monoclonal antibody (adalimumab), are effective and safe for managing RA and AS patients who do not to respond to traditional therapies. Although randomized controlled trials are considered the gold standard for evaluating the efficacy and safety of a therapeutic intervention, their results have limited applicability to patients in routine clinical practice (2). Observational studies using large health-care databases can complement the findings of randomized controlled trials by assessing treatment effectiveness in patients encountered in day-to-day clinical practice. Furthermore, well-designed observational studies can identify clinically important differences among therapeutic options, and provide data on diverse patient populations with common comorbidities and safety data with longer follow-up periods (3). For biologicals, such as TNF inhibitors used in the treatment of RA and AS, most data come from national-wide registries, such as the British Society for Rheumatology Biologics Registry (BSRBR) (4, 5, 6), Antirheumatic Therapies in Sweden (ARTIS) (7, 8) and SSAGT (Southern Sweden) (9), Rheumatoide Arthritis: Beobachtung der Biologika-Therapie (RABBIT; Germany) (10), Recherche Axée sur la Tolérance des Biothérapies (RATIO; France), Denmark Biologicals resistry (DANBIO) (11, 12, 13, 14), Spanish Registry of Adverse Events of Biological Therapies in Rheumatic Diseases (BIOBADASER) (15, 16), and the Consortium of Rheumatology Researchers of North America (CORRONA) (17). In Korea, the Korean Biologics Registry (KOBIO) was started in 2013, and does not yet provide data on TNF inhibitors in Korean patients with RA and AS.
Due to a lack of Korean data on the use of TNF inhibitors in RA and AS patients, we compared the between-group drug survival rates for infliximab, etanercept, and adalimumab in a single tertiary center and evaluated potential predictors of discontinuation of TNF inhibitors in these patients.
MATERIALS AND METHODS
Population and study design
The study population comprised 114 RA and 310 AS patients who were treated with three TNF inhibitors, infliximab, etanercept, or adalimumab, with at least 1 yr of follow-up at Chonnam National University Hospital, Gwangju, Korea from December 2002 to November 2011. All patients eligible for the study had been diagnosed with RA or AS by a physician. All RA patients met the 1987 American College of Rheumatology (ACR) criteria for RA (18) and all AS patients also met the modified New York Criteria for AS (19) or Assessments in Ankylosing Spondylitis (ASAS) criteria for axial spondyloarthritis (20). The TNF inhibitors were administered in the following manner. Infliximab (3-5 mg/kg) was given intravenously at 0, 2, and 6 weeks and then every 8 weeks. In cases of inadequate response, the frequency of infliximab treatment was increased to every 6 weeks. Etanercept was administered as a subcutaneous injection once (50 mg) or twice (25 mg) a week. Adalimumab (40 mg) was administered as a subcutaneous injection on alternate weeks.
For each patient, data on their treatment with infliximab, etanercept, or adalimumab were collected from the patients' charts, as were data on age, gender, education level, disease duration, Disease Activity Scores of 28 joints (DAS 28), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), laboratory findings including rheumatoid factor (RF) and anti-cyclic citrullinated peptide (CCP) antibody, and concomitant medications at the time of initiation of TNF inhibitors and during follow-up. For AS patients, the radiographic changes of the sacroiliac joints on plain radiographs were graded as 1-4 according to the modified New York criteria (19).
The primary outcome was TNF inhibitor discontinuation for any cause. Patients were followed for at least 1 yr from the time of TNF inhibitor initiation until discontinuation. Data were also collected on the cause of drug discontinuation for the following prespecified, mutually exclusive categories: adverse event, lack of efficacy, patient's intention, economic issue, or other. As a secondary outcome, predictors of discontinuation were investigated, including age, gender, laboratory variables, disease activity, and concomitant medication.
Statistical analyses
Data are shown as the means±standard deviation (SD). Non-parametric statistical methods were used for comparisons: the Kruskal-Wallis test for comparing continuous variables between groups and Fisher's exact test for differences in dichotomous variables. Drug-specific and calendar period-specific discontinuation rates were calculated and presented using Kaplan-Meier curves. Cox regression was used to estimate the hazard ratio (HR) for discontinuation. Predictors were investigated using univariate and multivariate models, stratified by drug. Variables with a P value of less than 0.10 in the univariate analysis were included in the multivariate analysis. Statistical analyses were performed using the SPSS software package. A P value of less than 0.05 was considered to indicate statistical significance.
RESULTS
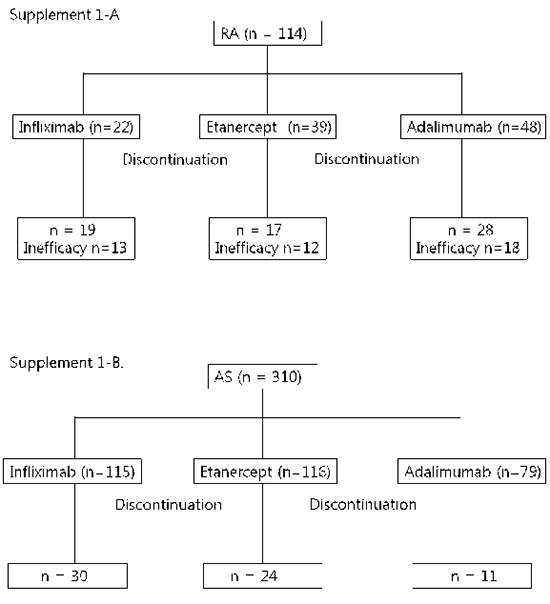
A total of 114 RA patients treated with TNF inhibitors from December 2002 to November 2011 were identified, with 22 patients receiving infliximab, 39 etanercept, and 48 adalimumab; 310 AS patients were identified during the same period, with 115 patients receiving infliximab, 116 etanercept, and 79 adalimumab.
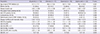
In the RA patients, the mean age at the start of TNF inhibitor was 51.4 (SD±14.1) yr, 80.5% (n=91) were women, and the disease duration of RA was 4.82 yr (SD±4.06). RF and anti-CCP were positive in 93.9% and 86.0% of the patients, respectively. Regarding concomitant medications, 93.9% (n=107) of the patients were taking corticosteroids and 83.3% (n=95) were taking methotrexate (MTX). The DAS 28 at baseline was 7.00±1.07. There were no significant differences among the three treatment groups with regard to age, gender, disease duration, RF and anti-CCP positivity, DAS 28, and concomitant medications. The baseline characteristics of the RA patients are shown in Table 1.
In the AS patients, the mean age at the initiation of TNF inhibitors was 35.4 yr (SD±11.8), 81.3% (n=252) were men, and the disease duration of AS was 3.49 yr (SD±5.22). The patients treated with infliximab were older than those treated with etanercept or adalimumab (P=0.032), and the patients treated with etanercept were more often male than those treated with infliximab or adalimumab (P=0.014). The disease duration was longer for patients treated with etanercept than for adalimumab and infliximab (P=0.032). MTX and other disease-modifying anti-rheumatic drugs (DMARDs) were used more commonly in patients treated with infliximab than in those treated with etanercept or adalimumab (P=0.005 and P=0.003, respectively). The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were higher in patients receiving infliximab than those receiving etanercept or adalimumab (P=0.014 and P=0.038, respectively). Table 2 shows the baseline characteristics of the AS patients.
Of the 114 RA patients included in the analysis, 64 discontinued the first TNF inhibitor after a mean of 33.8 (range 0-77) months; the number of patients who were prescribed infliximab, etanercept, and adalimumab was 19, 17, and 28, respectively. The most common cause of TNF inhibitor discontinuation was inefficacy, which was reported by 43 (67.2%) patients for all TNF inhibitors: 13 for infliximab, 12 for etanercept, and 18 for adalimumab. Adverse events occurred in 9 (14.1%) patients, including skin eruption in three, infection in five, and aggravation of heart failure in one patient.
Among the AS patients, 65 (21.0%) discontinued the TNF inhibitors: 30 for infliximab, 24 for etanercept, and 11 for adalimumab. The reasons for discontinuation were adverse events (39.7%, n=27), inefficacy (33.3%, n=21), intention of patients (9.5%, n=6), economic status (11.1%, n=7), hospitalization (3.2%, n=2), and lost to follow-up (3.2%, n=2). Adverse events leading to discontinuation included malignancy (3.7%, 1 patient taking infliximab), infection (13.8%, n=4), tuberculosis (11.1%, n=3), skin eruption (44.4%, n=12), cardiovascular complication (3.7%, n=1), and other causes (22.2%, n=6; pregnancy 2, uveitis 4).
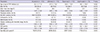
In the univariate Cox proportional hazard analysis, the drug discontinuation rate differed among the three TNF inhibitors in RA patients and etanercept (HR, 0.359; 95% CI, 0.188-0.688) had a lower drug discontinuation rate than infliximab (Table 3, Fig. 1). The use of concomitant corticosteroids at TNF inhibitor initiation was associated with higher discontinuation rates (HR, 1.835; 95% CI, 1.221-2.759, P=0.003), and the use of ≥3 DMARDs was associated with lower discontinuation rates (HR, 0.450; 95% CI, 0.223-0.910, P=0.026). In the multiple Cox regression analyses, the use of concomitant corticosteroids was a significant predictor of discontinuation (HR, 7.850; 95% CI, 1.012-60.890, P=0.049).
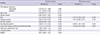
The univariate and multivariate Cox proportional hazard analyses for TNF inhibitor discontinuation in AS patients are presented in Table 4. There were significant associations between the discontinuation rate and male gender (HR, 0.441; 95% CI, 0.257-0.759, P=0.003), peripheral arthritis (HR, 2.079; 95% CI, 1.054-4.101, P=0.035), radiographic grade 4 sacroiliitis (HR, 1.949; 95% CI, 1.072-3.545, P=0.029), and concomitant DMARDs (HR, 1.787; 95% CI, 1.017-3.141, P=0.044). Multivariate Cox regression analysis showed that male gender (HR, 0.327; 95% CI, 0.149-0.722, P=0.006) and grade 4 sacroiliitis (HR, 2.629; 95% CI, 1.347-5.131, P=0.005) were significant predictors of discontinuing treatment (Table 4).
DISCUSSION
In this study, we found that although the survival rate did not differ among the three TNF inhibitors in AS patients, the etanercept group had a lower discontinuation rate than the infliximab group in RA patients. The most common cause of TNF inhibitor discontinuation in RA patients was inefficacy, whereas the main reason for discontinuation in AS patients was adverse events. In addition, RA patients who received corticosteroids in combination with TNF inhibitors were more likely to discontinue their therapy. The independent predictors of drug discontinuation in AS patients were male gender and complete ankylosis of the sacroiliac joint on radiographs.
One main finding of our study is that the majority of AS patients had a higher continuation rate of TNF inhibitor treatment compared to RA patients (Fig. 1). AS patients treated with a first TNF inhibitor had a good overall drug survival rate, with 79% of patients remaining on treatment after 2 yr. By contrast, RA patients treated with a first TNF inhibitor had a continuation rate of 44% after 1 yr. These findings are consistent with those of previous studies, including the Danish DANBIO (13, 14), Spanish BIOBADASER (16, 21), and a Norwegian study (22). Although other factors might influence the retention rates of TNF inhibitors, drug survival can be regarded as a surrogate marker for efficacy. Since the most common cause of discontinuation in RA patients was inefficacy, TNF inhibitors are more efficacious in the treatment of AS than in RA. The possibility that should be borne in mind is that a TNF inhibitor is the only effective treatment for AS patients with axial involvement, whereas several other biological agents other than TNF inhibitors are available for RA patients. Therefore, the comparative retention rate for RA might be lower than that for AS. In this study, the gap in the drug continuation rates between RA and AS was much higher than that reported in other studies. This could be attributed to strict insurance standards for TNF inhibitor coverage in RA patients in Korea. RA patients who are eligible for TNF inhibitors must have more than twenty active joints, elevated acute phase reactants, and inefficacy of two or more DMARDs over 6 months. Consequently, those patients who have very high disease activity are more likely to be refractory to TNF inhibitors.
In this study, etanercept had the best retention rate, whereas infliximab had the shortest drug persistency rate in patients with RA. The same findings are reported in the DANBIO (14), RADIUS (23), LORHEN (24), and Swiss SCQM studies (25), showing that the drug continuation rates are highest for etanercept and lowest for infliximab in RA patients. In contrast to the above-mentioned European studies, the US studies have shown the opposite result (17). Patients who started TNF inhibitors in the USA have much lower disease activity at initiation than European patients, and infliximab users have been treated with higher doses than in Europe. Considering the very high disease activity (DAS 28 score 7.00) in our patients at the time of TNF inhibitor initiation and the lower infliximab dose, our findings are more consistent with European than the US studies. The different survival rate of TNF inhibitors in our patients can be explained by the development of anti-drug antibodies, which are associated with lower response and lower retention rates in RA patients receiving TNF inhibitors (26). The formation of neutralizing antibodies against infliximab or adalimumab is common and is associated with the loss of the previously achieved clinical response (27), while anti-etanercept antibodies are not detected or only in a low number of patients without influence on efficacy (28). The absence of clinically significant immunogenicity against etanercept can be translated into the greater drug survival found for etanercept in comparison with infliximab or adalimumab.
In this study, the drug survival rate of AS patients did not differ among the three TNF inhibitors. Only a few studies on the drug survival of TNF inhibitors in AS patients have been published. In a DANBIO study of AS patients, the retention rates were similar among patients receiving infliximab, adalimumab, and etanercept (13). Based on these results, we postulate that the drug retention rate of TNF inhibitors does not differ in AS patients, in contrast to RA patients. Although the reason why the drug survival rate of TNF inhibitors differed between RA and AS patients in our study is unclear, one possibility is that infliximab is administered more frequently and at higher doses in AS, compared with RA, which is known to decrease the development of anti-infliximab antibodies. The lower incidence of anti-infliximab antibodies in AS patients might contribute to the similar retention rate among the three TNF inhibitors.
Another significant finding in the present study is the identification of causes of drug discontinuation. In RA patients in the SSAGT (29) and DANBIO studies (14), the main causes of TNF inhibitor withdrawal were adverse events and lack of efficacy. In AS patients in the same studies (20, 29), the reasons for treatment withdrawal were almost equally distributed among adverse events, inefficacy, and other reasons including disease remission and follow-up loss. In our study, more than half of RA patients discontinued the drugs due to inefficacy; another main reason was the occurrence of adverse events. The main reason for discontinuation in AS patients was adverse events and other reasons were inefficacy, intention of patients, economic status, hospitalization, and loss to follow-up. Given the different causes of discontinuation in RA and AS patients, we hypothesize that the interactions between rheumatic diseases and TNF inhibitors are different.
In the Cox regression analyses, concomitant medication with corticosteroids was identified as a significant predictor for discontinuing TNF inhibitors in RA patients. Although this association is not found in other observational studies, concomitant corticosteroid use reflects high disease activity in these patients and patients with high disease activity are more likely to be refractory to TNF inhibitors. On the other hand, it is controversial whether concomitant DMARDs medication predicts drug discontinuation. Treatment with concomitant DMARDs, especially MTX, was associated with better drug survival in the SSAGT study (9) and a Norwegian study (22), whereas the retention rate was greater without concomitant DMARDs in a French study (30). The impact of concomitant MTX use was not found in a Spanish study (16), as in our study.
In our study, female gender and grade 4 sacroiliitis in AS patients were associated with a higher risk of treatment termination. We found longer treatment retention of TNF inhibitors in males compared with females. This concurs with previous studies, not only in AS (13, 31), but also RA (16, 32) and psoriatic arthritis (33). Why the clinical response differs according to gender is still unclear.
This is the first study to show that grade 4 sacroiliitis was a significant predictor of discontinuation in AS patients. In the BSRBR (34) and DANBIO (33) studies, patients with a higher BASFI score at the start of TNF inhibitors were less likely to see an improvement in BASDAI. In line with this observation, patients who have severe functional disability as indicated by grade 4 sacroiliitis are less likely to improve and are more likely to discontinue their therapy.
We conclude that in this single-center cohort of RA and AS patients treated with TNF inhibitors in routine clinical practice, significant differences in drug survival and reasons for discontinuation of therapy were observed. Although the survival rate did not differ among the three TNF inhibitors in AS patients, the etanercept group had a lower discontinuation rate than the infliximab group in RA patients. Furthermore, we confirmed that concomitant corticosteroid treatment in RA patients and gender and radiographic progression in AS patients were significant predictors of TNF inhibitor discontinuation.


 XML Download
XML Download