

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Metformin is one of the most widely used oral hypoglycemic agents (1). Most of the current global clinical practice recommendations, including those of the American Diabetes Association, the European Association for the Study of Diabetes, and the Korean Diabetes Association, propose that metformin, if there are no contraindications, should be initiated with concurrent lifestyle modifications at initial diabetes diagnosis (2, 3, 4).
Most of the side effects due to metformin are mild and usually include gastrointestinal symptoms, such as abdominal distress, soft stools, and diarrhea (5). Generally, these side effects appear shortly after the initiation of metformin and promptly disappear after discontinuation. However, insidious or asymptomatic side effects resulting from long-term treatment, such as vitamin B12 deficiency, may not be easily detected without close attention. Serum vitamin B12 levels have been reported to be inversely associated with the dose and duration of metformin use (6, 7, 8). These studies reported that an average of 10 to 30% of patients exhibited malabsorptive vitamin B12 deficiency (6, 9).
Although the clinical significance of vitamin B12 deficiency related to metformin treatment is debatable, monitoring for vitamin B12 has been recommended for patients with type 2 diabetes, especially those on long-term metformin treatment (7). Clinically, vitamin B12 deficiency could lead to altered mental status, megaloblastic anemia, and neurological damage (7, 10, 11). Unfortunately, diabetic neuropathy symptoms can overlap with paresthesias, impaired vibration sensation and proprioception (12). Therefore, peripheral neuropathy due to vitamin B12 deficiency may be confused with diabetic peripheral neuropathy or may contribute to the aggravation of diabetic peripheral neuropathy (10, 11). The progression of neurologic damage due to vitamin B12 deficiency can be stopped by early detection and treatment with cobalamin supplementation (13). However, if this occurrence is misdiagnosed as diabetic neuropathy, permanent neurological damage may occur (11).
As metformin has been prescribed worldwide and treatment periods increase, the prevalence of metformin-induced vitamin B12 deficiency may have also significantly increased. However, the relationship between metformin use and vitamin B12 deficiency in the Asian population has not been widely investigated. This study focused on the prevalence of vitamin B12 deficiency and the factors associated with it in Korean patients with type 2 diabetes who were treated with metformin.
MATERIALS AND METHODS
Between January and September 2012, patients with type 2 diabetes, aged 20 to 80 yr, who had taken metformin for at least three months were recruited consecutively at the university-affiliated diabetes center of St. Vincent's Hospital in Korea. Exclusion criteria included patients with newly diagnosed type 2 diabetes, patients who had pernicious anemia, pregnant women, type 1 diabetes, decreased renal function (serum creatinine levels >1.7 mg/dL for men and >1.5 mg/dL for women), prior vitamin B12 injections, gastrectomy, colectomy, inflammatory bowel disease, and vegetarianism. Patients were also excluded if they had any severe medical illness, such as sepsis, severe infection, malignancy, liver cirrhosis, heart failure, or renal failure. Medication history was evaluated by a dietary supplement questionnaire, which included over-the-counter multivitamins, calcium supplements, histamine-2 receptor blockers (H2 blocker) and proton pump inhibitor (PPI). Alcohol intake was calculated as the weekly servings of alcoholic beverages determined by multiplying the frequency of alcohol consumption by the number of alcoholic beverage servings consumed on one occasion (14).
Laboratory analysis
The baseline demographic information of the participants was collected. Smoking habits were divided into current smoker, ex-smoker, and non-smoker. Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or any use of antihypertensive medications (15).
The primary outcome was biochemical vitamin B12 deficiency determined by serum vitamin B12 concentrations. The serum vitamin B12 and folate levels were quantified by chemiluminescent enzyme immunoassay (Immulite 2000; Siemens, Berlin, Germany). We defined biochemical vitamin B12 deficiency as serum levels ≤300 pg/mL without folate deficiency (1, 16). In the absence of recent anorexia or fasting, a serum folate concentration <2 ng/mL was diagnostic of folate deficiency. If the serum folate concentration was >4 ng/mL, folate deficiency was effectively ruled out (1). Anemia was defined as Hb <13 g/dL for men and <12 g/dL for women by WHO guidelines (17).
The blood glucose level was measured using an automated enzymatic method, and the HbA1c level was determined by high-performance liquid chromatography (HLC-723 G8; Tosoh, Tokyo, Japan). Total cholesterol (TC), triglyceride, and HDL-cholesterol were measured enzymatically using an automatic analyzer (Hitachi 736-40; Hitachi, Tokyo, Japan). The measurement of microalbuminuria was performed using immunoturbidimetry (Hitachi 7600-110; Hitachi, Tokyo, Japan) in a random spot urine collection, and the albumin-to-creatinine ratio (ACR) was calculated. Diabetic nephropathy was classified into three groups, as follows: no diabetic nephropathy (ACR<30 µg/mg creatinine); microalbuminuria (ACR of 30-300 µg/mg creatinine); and macroalbuminuria (ACR≥300 µg/mg creatinine) (18). Diabetic retinopathy was assessed from retinal photographs at baseline, and the findings were reviewed by a board-certified ophthalmologist. Diabetic retinopathy was classified as the absence or presence of diabetic retinopathy.
Statistical analyses
We used SAS version 9.2 (SAS Institute, Inc., Cary, NC, USA) for the statistical analysis. Clinical characteristics and parameters were expressed as the mean±standard deviation (SD), or numbers (percentage). Pearson's chi-square tests were used to test the differences in the proportion of categorical variables, and independent t-tests were used for evaluating the difference between the means of two continuous variables. Pearson correlation analyses were performed to examine the linear relationship between serum vitamin B12 and metformin use. The variables which were statistically significant in the univariate analysis, considered to be important in diabetes, or reported to affect vitamin B12 levels were included in the multivariate analysis. Multiple logistic regression analysis was performed to assess the independent predictive effect of the variables on the risk for vitamin B12 deficiency. Receiver operator characteristic (ROC) curve analysis was used to evaluate the relationship between the duration of metformin use and vitamin B12 deficiency and to determine the reflection point (cut-off value). The area under the curve (AUC) with 95% confidence interval (CI) was calculated. P values<0.05 were considered to be statistically significant.
RESULTS
During the study period, 832 eligible patients were identified and agreed to participate. Of the 832 patients, 799 (96.0%) completed the evaluation (Fig. 1). The clinical characteristics of these patients are shown in Table 1. The mean serum vitamin B12 concentration was 665.7±246.7 pg/mL (644.1±243.3 pg/mL in men, 664.0±249.3 pg/mL in women), and there was no significant difference according to sex. Vitamin B12 deficiency was present in 9.5% (n=76) of patients using metformin. There were no differences in the sex, alcohol use, over-the-counter multivitamin use, calcium supplement use, H2 blocker or PPI use, or diabetic complications between patients with and without vitamin B12 deficiency. However, patients with vitamin B12 deficiency had a longer duration of metformin use (P<0.001), a larger daily dose of metformin (P<0.001) than the patients without vitamin B12 deficiency (Table 1). Patients with vitamin B12 deficiency had higher rates of anemia (P=0.004) than the patients without vitamin B12 deficiency. There were differences in the insulin use (P<0.001) and sulfonylurea use (P<0.001) and no differences in the diabetic duration, baseline fasting glucose, creatinine level, HbA1c, or serum folate level between the two groups.
Of the 129 patients (16.1%) with anemia, the mean Hb levels of the vitamin B12 deficient and non-deficient groups were 11.6±0.7 and 11.2±1.0 g/dL, respectively (P=0.104). Four of the patients (3.1%) were confirmed with iron deficiency anemia (IDA), 66 (51.2%) were classified as anemia of chronic disease, and 2 (1.6%) had thyroid dysfunction. Four patients from the total study population (0.5%) had a mean corpuscular volume (MCV)>100 femtoliters (fL). Of the participants with anemia, only two patients (1.6%) had an MCV>100 fL. One person had a hemolytic disorder which resulted in macrocytosis and the reason for macrocytosis could not be explained in the other. No deficiencies in either vitamin B12 or folate were detected in those with MCV>100 fL. There were no differences in the smoking, BMI, duration of metformin use, daily dose of metformin, other type of diabetes medication including thiazolidinediones, antiplatelet agent, HbA1c, or folate level in subjects with and without anemia. However, patients with anemia were older and had longer duration of diabetes than those who were without anemia (64.1±10.8 yr vs. 58.0±10.8 yr; P<0.001, 15.1±7.6 yr vs. 10.5±7.7 yr; P<0.001). After adjusting for age, diabetes duration, alcohol use, smoking, diabetic nephropathy, diabetic retinopathy, cerebrovascular disease, coronary heart disease, folate and vitamin B12 deficiency, the anemic patients showed significant difference in older age (adjusted OR, 1.03; 95% CI, 1.01-1.06; P=0.003), diabetic duration (adjusted OR, 1.04; 95% CI, 1.01-1.07; P=0.011), diabetic nephropathy (adjusted OR, 4.17; 95% CI, 2.21-7.88; P<0.001), and vitamin B12 deficiency (adjusted OR, 2.21; 95% CI, 1.24-3.92, P=0.007), respectively.
The correlation between the levels of serum vitamin B12 and the duration of metformin use was evaluated. The vitamin B12 levels had a negative correlation with the duration of metformin use (r2=0.020, P<0.001) and daily dose of metformin (r2=0.073, P<0.001). Neither BMI (r2=0.000, P=0.671) nor diabetic duration (r2=0.000, P=0.718) showed any correlation with vitamin B12 levels. We also investigated the effect of categorical dose and duration of metformin use on vitamin B12 levels (Fig. 2). Box-and-whisker plot showed vitamin B12 level according to different daily dose of metformin and duration of metformin use (P<0.001). Post hoc anaylsis revealed lower vitamin B12 concentration in patients who taken metformin for ≥10 yr than patients receiving metformin for 4-10 yr and those taken metformin <4 yr (Fig. 2A). When analyzed in a similar manner, the vitamin B12 levels were lower in patients receiving metformin ≥2,000 mg/day and in those receiving 1,000-2,000 mg/day than in those receiving ≤1,000 mg/day (Fig. 2B).
Table 2 demonstrats the association of various risk factors with serum vitamin B12 deficiency. After adjusting for age, sex, diabetic duration, BMI, alcohol use, H2 blocker or PPI use, over-the-counter multivitamin or calcium supplement, insulin or sulfonylurea use, HbA1c level, TC level, presence of anemia and MCV level, the most significant OR was associated with the daily metformin dose and duration of metformin use. A 1,000 mg/day metformin dose increment conferred a greater than two fold increased risk of developing vitamin B12 deficiency. There was a significantly lower vitamin B12 concentration among those patients receiving 1,000 mg/day to 2,000 mg/day than in those receiving≤1,000 mg/day (adjusted OR, 2.52; 95% CI, 1.27-4.99; P=0.008). Additionally, the risk of vitamin B12 deficiency was increased in those taking ≥2,000 mg/day than those taking ≤1,000 mg/day (adjusted OR, 3.80; 95% CI, 1.82-7.92; P<0.001). Compared with metformin use of less than 4 yr, the adjusted OR was 4.65 (95% CI, 2.36-9.16; P<0.001) for metformin use of 4 to 10 yr and in use at least 10 yr, the adjusted OR was 9.21 (95% CI, 3.38-25.11; P<0.001). There was no association of serum vitamin B12 levels with sex, age, BMI, alcohol use, MCV level, TC level and HbA1c value. We found no significantly increased risk for the concurrent use of H2 blockers or PPIs, over-the-counter multivitamins, calcium supplements, insulin or sulfonylurea.
The ROC curve for the duration and dose of metformin use was analyzed. For the duration of metformin use, the AUC value was 0.72 (95% CI, 0.655-0.777; P<0.001) and the reflection point (cut-off value) was 45.5 months with a sensitivity of 80.0% and a specificity of 57.0%. The AUC value was 0.69 (95% CI, 0.628-0.752; P<0.001) and the reflection point (cut-off value) was 1,125 mg (sensitivity 64%; specificity 65%) for the daily dose of metformin (Fig. 3).
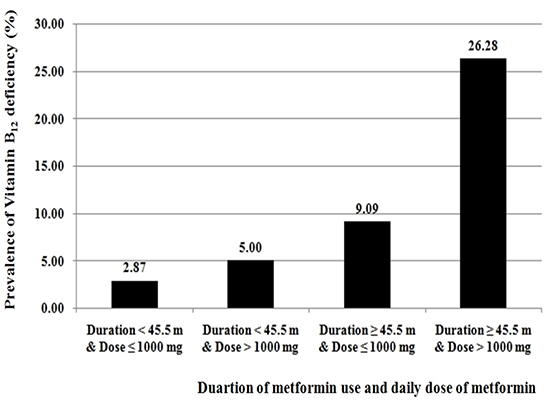
Patients who had taken metformin >1,000 mg/day for ≥45.5 months were approximately 10 times as likely to have vitamin B12 deficiency as patients taking metformin ≤1,000 mg/day for <45.5 months (Fig. 4).
DISCUSSION
Based on our results, we demonstrated that daily metformin dosage and treatment duration were the most consistent risk factors for vitamin B12 deficiency. This association remained evident even after adjusting for potential confounding factors by multivariate analysis, thus reinforcing our conclusion that higher metformin doses and longer treatment durations were independent risk factors. To the best of our knowledge, this is the first large-scale study that was specifically designed to investigate the prevalence and contributing factors for vitamin B12 deficiency confined to an Asian population with type 2 diabetes treated with metformin.
As in Western countries, metformin treatment with lifestyle modification is recommended as a first-line treatment for type 2 diabetes in Korea (2, 3, 4, 19). In Korea, the use of oral hypoglycemic agents among patients being treated for diabetes has been reported to be 80.1% (oral hypoglycemic agents alone, 70.0%, and in combination therapies with insulin, 10.1%) (20, 21). Metformin is the most frequently prescribed oral hypoglycemic agent (20, 21).
In this study, vitamin B12 deficiency was present in 9.5% of patients using metformin. The reported prevalence of vitamin B12 deficiency related to metformin use varies according to the study population. Data from the National Health and Nutrition Examination Survey showed that vitamin B12 deficiency was present in 5.8% of those with diabetes using metformin compared with 2.4% of those not using metformin (22). In a comparable study reported from Brazil, the prevalence of vitamin B12 deficiency in patients with type 2 diabetes using metformin was 6.9% (23). The mean serum vitamin B12 levels among American adults with diabetes were 430.2±13.0 pg/mL in metformin users and 524.0±10.6 pg/mL in non-metformin users and 475.3 ±3.9 pg/mL in non-diabetic adults (22). In our study, the mean vitamin B12 level in patients with diabetes using metformin was 665.7±246.7 pg/mL. According to previous reports, the average serum vitamin B12 of Korean adults in the healthy population aged 23 to 72 yr was 537.0±222.0 pg/mL in men and 664.1 ±309.8 pg/mL in women, and the mean value of vitamin B12 was not different between diabetic and non-diabetic populations in Korea (24, 25).
The pathogenic mechanisms of vitamin B12 deficiency in metformin treatment have not been fully elucidated. However, among the instances of bacterial overgrowth in the small intestine attributable to diabetes mellitus, changes in small bowel motility, alterations in the bacterial flora, competitive inhibition, the inactivation of vitamin B12 absorption, or the effect of calcium on cell membranes have been suggested to play a role (6, 8, 9, 26).
Vitamin B12 deficiency is clinically important because it is a reversible cause of bone marrow failure and demyelinating nerve disease. Neurologic damage, a possible consequence of metformin-induced vitamin B12 deficiency, can present as peripheral neuropathy and may be mistaken for diabetic neuropathy in patients on metformin treatment (10). Low vitamin B12 levels have been reported to be associated with worse nerve conduction velocities and poorer responses to light touch by monofilament detection (27). This may lead to the unnecessary use of anticonvulsants or tricyclic antidepressants (10, 28, 29). Another study explored the relationship between low serum vitamin B12 levels and cognitive impairment, depression and neuropathy. Low vitamin B12 states were more associated with symptoms of memory impairment with objective evidence of cognitive impairment than with depression or neuropathy (30). As vitamin B12-associated neuropathy is a treatable and reversible condition, early detection and treatment of vitamin B12 deficiency is clinically important in patients with diabetes using metformin.
Our study showed a clear relationship between the dosage or length of metformin use and vitamin B12 deficiency in patients with type 2 diabetes. According to our correlation analysis, vitamin B12 deficiency was associated with metformin dosage and length of administration. Subjects with metformin use ≥10 yr and daily dosage≥2,000 mg showed about a 4-fold higher risk of vitamin B12 deficiency compared to those with metformin use of <4 yr and daily dosage of ≤1,000 mg. Diabetic duration or presence of diabetic microvascular complications did not affect the development of vitamin B12 deficiency.
In the multivariate analysis, presence of anemia showed a statistically positive association with vitamin B12 deficiency. The classic form of anemia due to vitamin B12 deficiency is megaloblastic anemia (MCV>100 fL) (10). However, the observed mean MCV level in our subjects with vitamin B12 deficiency was not over 100 fL, and the prevalence of megaloblastic anemia was about 0.5%. There were no differences in the mean MCV between the groups with and without vitamin B12 deficiency. When the independent effect of the various risk factors for anemia were analyzed through multiple logistic regression analysis, age, diabetic duration, diabetic nephropathy and vitamin B12 deficiency were found to have a significant difference. Therefore, the anemia of our patients was most likely to have a multifactorial cause. Though megaloblastic anemia is widely regarded to have an increased MCV, previous reports have indicated that up to 30% of vitamin B12 responsive disorders have normal MCVs (13, 31, 32, 33). Also, masking of the macrocytic expression of megaloblastic anemia by coexisting thalassemia, iron deficiency and chronic illness has been widely reported (33, 34). As such, investigating the red cell distribution width and reticulocyte index or careful examination of the blood through a peripheral blood smear could have been helpful in distinguishing vitamin B12 deficiency-related anemia from anemia of other causes (34).
Neuropathic pain from vitamin B12 deficiency should be differentiated from that of diabetic neuropathy. However, we did not check the prevalence of suspicious neuropathic pain related with vitamin B12 deficiency. Generally, diabetic neuropathy can be confirmed by electromyography or nerve conduction tests, which were not done as they were not routinely performed at the outpatient level. These studies should be done in order to fully evaluate and diagnose neuropathic pain in patients with vitamin B12 deficiency.
The main strength of this study was that we have divided metformin use by both length of use and dosage, unlike previous studies which focused on only one factor. By doing this, we have confirmed that length of use and dosage have a cumulative effect. This is also the first study to present a reflection point for length of meformin use, which would be useful in selecting patients for vitamin B12 monitoring. Additionally, our study was designed as a large cohort of about 800 participants with type 2 diabetes in a single ethnic population.
In conclusion we demonstrated that vitamin B12 deficiency occurs more frequently in patients with type 2 diabetes with longer duration of metformin use and in those taking larger amounts of metformin. Currently, there are no published guidelines advocating routine screening for vitamin B12 deficiency among patients with type 2 diabetes undergoing metformin treatment. Although the clinical significance of vitamin B12 deficiency remains unclear, our data suggest the need for routine vitamin B12 monitoring in patients with type 2 diabetes, especially in metformin users of more than four years with average dose of over 1,000 mg per day, even in the absence of hematological abnormalities.






 XML Download
XML Download