

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chest compression depth (CCD) is an important factor in the effective performance of chest compressions (CCs) during cardiopulmonary resuscitation (CPR) (1, 2). According to the European Resuscitation Council (ERC) Guidelines for Resuscitation 2010, CPR performers should compress the sternum of a patient to a depth of approximately 5-6 cm on a firm surface when possible (3). To ensure performance of high-quality CPR, many kinds of feedback devices have been used, and these have been shown to improve CCD in studies involving manikins. These feedback devices have an accelerometer or a pressure sensor that measures CCD accurately when a patient is laid on a firm surface such as a floor (4). However, when CPR is performed in hospitals, patients are laid on mattresses with different configurations on a bed frame. Perkins et al. (5) found that mattress compression depth (MCD) leads to an overestimation of CCD during CPR with a feedback device in simulated cardiac arrest. Therefore, the performance of CPR on mattresses in hospitals may hinder compliance with ERC guidelines despite the use of feedback devices.
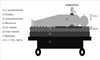
In an early study in this field, compression of a foam mattress placed under a manikin accounted for approximately 30%-40% of the total CCD (i.e., sternal-spinal CCD + MCD = total compression depth [TCD]) (5-7). This level interfered with the performance of adequate CCD (i.e., sternal-spinal CCD) (5-9) Therefore, many authors have proposed that the use of a backboard may improve CCD during CPR performed when patients are on a foam mattress (5-7, 10). However, there is no evidence for or against the use of backboards in the 2010 ERC guidelines (3). Inflated air mattresses [i.e., the other type of mattress that is often used for groups at high risk of cardiac arrest in hospitals (11, 12)] are also compressed during CPR, although studies on the effectiveness of a backboard when patients are on an air mattress during CPR have yielded mixed results. Some authors have examined MCD using an inflated air mattress placed on the floor or on a bed frame without a foam mattress (5, 6). Unfortunately, in clinical settings, inflated air mattresses are typically placed on top of foam that has been laid on a bed frame (see Fig. 1 for typical configuration of inflated air mattresses). No published studies have investigated MCD with the use of a backboard and the typical hospital bed configuration involving an inflated mattress. Air mattresses should be deflated for high-quality CPR when performing CC according to ERC guidelines for Resuscitation 2010. There is also a lack of research on the inflated air mattress configuration seen in Fig. 1 (3, 13).
For the purposes of this study, we hypothesized that MCD is increased when using the inflated air mattress configuration typically seen in hospitals compared to using a deflated air mattress placed on top of foam laid on a bed frame. We also hypothesized that the use of a backboard reduces MCD sufficiently to achieve accurate CCD during CPR with feedback devices. Additionally, we tried to confirm the effect of deflation of the air mattress on this configuration.
MATERIALS AND METHODS
Measurement of CCD and MCD using a dual accelerometer
As shown in Fig. 1, we used dual accelerometers (MMA 7260QT, Freescale Semiconductor Inc., Austin, Texas, USA) to estimate MCD and TCD. One accelerometer was placed on the manikin's sternum (a1), and the other was placed between the manikin's back and the surface (a2) (6). The combined CCD and MCD (TCD) were measured by a1, whereas a2 measured MCD only. TCD and MCD were obtained through double integration of acceleration signals. CCD was calculated by subtraction of MCD from TCD (14). During the integration, an error in depth occurred because of integration constants, but we were able to reduce this error by using the de-trend of the integrated signal (6, 14). Procedures for estimating MCD using an accelerometer are well established, and accuracy can be confirmed using a linear variable differential transformer (LVDT) RDP-100S (Radian Co., Ltd, Seoul, Korea) (6, 14).
Materials
A Resusci Anne Modular System Skill Reporter manikin (9.9 kg, Laerdal Medical, Orpington, UK) was used in all experiments involving performance of CPR. By adding additional weight to the manikin, total weight was increased 34 kg to simulate the upper body weight of adult humans. The bed frame (760 × 2,110 mm, 228 kg; Transport stretcher®, Stryker Co., Kalamazoo, Michigan, USA), the foam mattress (660 × 1,920 × 80 mm, soft foam with polyurethane cover; Stryker Co.), the inflatable air mattress (pressure 23 mmHg, 800 × 1,800 × 100 mm, MD-200 Normal L/V, polyurethane; Eunhye Medical Co., Seoul, Korea), and the backboard (450 × 600 × 10 mm, 3 kg; Lifeline Plastic, Sung Shim Medical Co., Bucheon, Korea) were used for various surface configurations, as shown in Fig. 2.
Study design and participants
This study was a randomized experimental trial with repeated measures; it was carried out at a university hospital on April 27, 2012. Eight emergency physicians from Hanyang University Hospital, who were also basic life support providers, took part in this study. The sample size was determined using G-power 3.1.2® (Heine Heinrich University, Düsseldorf, Germany) with a power of 0.8 and an α level set at 0.05.
Data collection
The participants performed CCs on manikins placed on the 4 different underlying surfaces with a visual feedback system according to the ERC guidelines. This was carried out in a randomized order after the drawing of lots. The 4 underlying surface conditions are described in Fig. 1. as A, B, C, and D. Surface B was chosen to analyze the effect of deflating the air mattress as per the 2010 ERC guideline suggestions (4, 8). Configuration C is a typical hospital configuration involving the use of an inflated air mattress.
For the CCs, the basic life support providers stood next to the manikins, which were placed on the varying underlying surfaces. The height of the manikin's back was set at the same height as the provider's knee using bed height adjustments and a step stool (15). Approximately 110 CCs were performed over 60 sec for each underlying support material according to the 2010 ERC guidelines; there were 5-min breaks between tests for each underlying support material.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences ver. 18.0 for Windows (SPSS, Chicago, IL, USA). All groups were analyzed using the Shapiro-Wilk test to test for normality. Repeated measures analysis of variance (ANOVA) was used to analyze comparisons of MCD, TCD and CCD between surfaces. Greenhouse-Geisser correction was applied considering violation of sphericity assumption as shown by the Mauchly test. Values for these compression depths are reported as mean ± standard deviation (SD) and 95% confidence interval (CI). Post-hoc analyses were performed using the Bonferroni correction and a P value of < 0.05 was considered significant.
RESULTS
Study participants
All study participants were male, and the median age was 33.5 yr (range 27-36 yr). The median weight was 85 kg (range 70-89 kg), and the median height was 173.5 cm (range 165-183 cm).
MCD on 4 different surfaces
The bed frame displacement depth was 5.6 ± 0.6 mm (95% CI, 5.2-6.1) for surface A. The MCD was 14.7 ± 1.4 (95% CI, 13.6-15.9) for surface B and 30.2 ± 4.0 (95% CI, 26.8-33.5) for surface C. For surface D, the MCD was 25.5 ± 2.9 (95% CI, 22.2-28.7). In comparison with surface A, the MCD for surfaces B, C, and D were significantly increased (all P values < 0.01). Additionally, compared with the MCD for surface C, the MCD for surface B, where the air mattress was deflated, was significantly decreased (P < 0.001). When we compared surface C with surface D, we found that the use of a backboard decreased MCD (P = 0.002) (Table 1). When comparing surface B with D, we found that deflation of the inflatable air mattress decreased MCD more than the use of a backboard (P = 0.002).
TCD for accurate performance of CC on 4 different surfaces
All providers performed CCs with visual feedback devices and CCD was found to be 50.3 ± 3.3 mm (95% CI, 47.5-53.1 mm) on surface A. For surface B, this was 50.2 ± 2.8 mm (95% CI, 47.8-52.5 mm), and for surface C, the figure was 50.5 ± 2.4 mm (95% CI, 48.5-52.5 mm). CCD was 50.4 ± 2.0 mm (95% CI, 48.7-52.1 mm) for surface D (all P > 0.99 in comparing one surface with others, respectively). To achieve the above-mentioned CCD without MCD feedback during CPR, TCD was 55.9 ± 3.8 mm (95% CI, 52.7-59.2) for surface A, 64.9 ± 3.8 (95% CI, 61.8-68.0) for surface B, 80.7 ± 3.7 (95% CI, 77.6-83.7) for surface C, and 75.9 ± 5.5 (95% CI, 71.3-80.5) for surface D (see Table 1).
DISCUSSION
Correct CCD is linearly related to the perfusion of vital organs during CPR (1). Edelson et al. (2) demonstrated that a 5-mm increase in CCD was associated with a 2-fold increase in shock success both in and out of hospital. Previous studies on the effectiveness of a backboard with an inflated air mattress have yielded mixed results; in addition, these studies examined MCD for an inflated air mattress that was placed on the floor or on a bed without a foam mattress, which is not a typical air mattress configuration (5, 6). However, in the present study, we examined the MCD for both use of a backboard and use of a deflated air mattress compared with the typical configuration involving inflated air mattresses used in hospitals. We also found the bed frame displacement. Jäntti et al. (16) reported that intensive care unit nurses performed CC just as effectively on the floor as they did when a patient was on a bed, and this without the use of feedback monitoring. However, the MCD for surface C (i.e., on a typical inflated air mattress configuration) was 30.2 ± 4.0 mm, which was the highest level seen for any of the 4 surfaces we studied. This means that when performing CCs on the typical inflated air mattress configuration (surface C), performers should compress the chest more deeply than required for the other surfaces. Surface A (i.e., on a bed frame without any mattress) resulted in 5.6 ± 0.6 mm of bed frame displacement which was the lowest level of all the 4 surfaces we studied. To achieve accurate CCD on surface C, the configuration has to be changed to surface A. However, it is impossible to remove the mattresses laid on bed frames as this interrupts CPR.
In this study, we found that MCD of surface C was 30.2 mm, which is approximately 40% of the TCD for surface C. The use of a backboard reduced MCD on surface C to 25.5 mm, which was 34% of TCD. However, this did not completely solve the problem of mattresses compression. On the other hand, the use of a backboard might help to perform adequate CC with a typical air mattress configuration. When deflation of the air mattress was completed, we found that MCD was 14.7 mm, which is approximately 30% of the TCD for surface B. Thus, we verified that deflation of an inflated air mattress is important for accurate CCs as per 2010 ERC guidelines (3). Furthermore, to reduce MCD, deflation was more effective than the use of a backboard. However, deflation takes more than 20 sec (13) or several seconds to several tens of seconds for a commercial air mattress. Therefore, we believe that use of a backboard might be helpful for accurate CCs until the mattress is entirely deflated.
Despite these findings, our study has few limitations. First, we did not evaluate the effect of a backboard while an air mattress was being deflated. Therefore, further research is required to assess whether use of a backboard contributes to more adequate CCD during deflation of an inflated air mattress during CPR. However, previously, the use of a backboard has been shown to improve CCD during CPR on a foam mattress (5-7). This surface is similar to a deflated air mattress on a foam mattress laid on bed frame (surface B in this study). Therefore, the backboard can be placed under the patient's back while the air mattress is deflating and can remain there after the mattress is entirely deflated. Second, we studied MCD on only 1 type of bed frame, air mattress, foam mattress, and backboard. Further examination in other type of bed frame, mattress and backboard might differ to the result of this study. It is worth noting that an inflated air mattress is usually placed on an intensive care unit bed, and not a stretcher bed. Therefore, further studies are now required to compare MCD for many types of bed frames, mattresses, and backboards.
In conclusion, compression of mattresses leads to large increases and high percentages of TCD when inflated air mattresses are placed on top of foam mattresses that have been laid on a bed frame. The use of a backboard and deflation of an air mattress in a typical inflated air mattress configuration reduces MCD and thus helps with the performance of accurate chest compression depth during CPR.


 XML Download
XML Download