

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dysphagia is frequently observed among patients suffering from stroke or other brain injuries. The frequency of dysphagia is reported to range from 29% to 81% after stroke (1, 2), and over 17% after traumatic brain injury (TBI) (3). Dysphagia after stroke or other brain injuries is known to be a risk factor for complications such as aspiration pneumonia, dehydration, and malnutrition. These complications influence the quality of life and long term prognosis after stroke or other brain injuries (4). Thus, dysphagia after stroke or other brain injuries should be screened aggressively. For this purpose, several bedside screening tests and clinical measurements are used to evaluate the presence and severity of dysphagia.
The videofluoroscopic swallow study (VFSS) is the most frequently utilized test to evaluate the nature and extent of dysphagia. With this test, it is possible to determine whether the patient can swallow safely, and identify the circumstances of safe swallowing. Using VFSS, we can test therapeutic and compensatory maneuvers to determine which ones are effective for a given patient. Most clinical centers often use protocols which include small amounts of liquid (1-2 mL), medium to large amount (5-10 mL) of liquid, semi-solid foods, and solid foods. However, these protocols should be adjusted by individual centers or countries according to their cultural context or dietary habits. Koreans usually eat steamed rice and soup as a staple food with several side dishes. Korean style soup itself is a thin liquid mixed with various types of solid or semi-solid components such as meat, radish or tofu. Frequently, steamed rice is mixed with soup, which produces a mix of solid and liquid foods (Fig. 1). The physiologic process of eating solid food is different from that of liquid food. Likewise, the swallowing physiology of mixed consistency food would be different from that of single consistency foods.
In clinical situations, dysphagia symptoms are often observed among patients who start on a regular Korean diet even though they have shown no significant abnormalities in VFSS using protocols in single consistency foods. From these experiences, we developed a hypothesis that the risk of aspiration or any abnormal symptoms of dysphagia is higher in mixed consistency foods than that of single consistency food. There are two studies which suggest the possibility of risk of aspiration of 'two phase mixture of foods' because the leading edge of the bolus of two phase food reaches lower in the pharynx than single consistency foods at swallowing onset (5, 6). However, the risk of aspiration or penetration of mixed consistency foods in the patients who showed no significant abnormalities from single consistency food VFSS still needs to be investigated. Also, for a practical reason, a study using mixed consistency food which is close to the typical Korean style diet is needed. Based on such needs, we designed this study to evaluate the risk of dysphagia of mixed consistency foods in patients with stroke or other brain injuries by comparing the single versus mixed consistency food VFSS.
MATERIALS AND METHODS
This study was designed as a prospective study. All patients were recruited from an inpatient rehabilitation unit of Chung-Ang University Hospital in Seoul, Korea. We assessed the eligibility of patients according to the following inclusion criteria; 1) definite evidence of stroke or other brain injuries in magnetic resonance imaging (MRI) or computerized tomography (CT), 2) patients who had started their regular hospital diet because they had no overt evidence of symptoms of dysphagia in bedside examination (alert mental status, opening of mouth for oral feeding, intact laryngeal movement with successful dry swallowing, swallowing one teaspoon of water without delay, involuntary cough, drooling or voice change), and 3) no significant abnormal findings in single consistency food VFSS, no overt penetration or aspiration when taking 2 and 5 mL of liquid, curd-type yogurt, soft blend diet (rice porridge) and steamed rice, and no significant residue (more than 10%) in the valleculae or pyriform sinus in the pharyngeal phase.
Single consistency food VFSS and mixed consistency food VFSS were performed during the admission period in the rehabilitation unit. A protocol from Logemann's study was modified and subsequently used (7). In the single consistency food VFSS, patients were given 2 mL and 5 mL of diluted barium (barium/water, 35/65% weight/volume ratio), curd-type yogurt, soft blend diet (rice porridge) and steamed rice orally. These were given twice at each lateral and anteroposterior position. When there were 1) no abnormal findings in the oral phase, 2) no overt penetration, aspiration and 3) no significant residue (more than 10%) in the valleculae or pyriform sinus in pharyngeal phase in the single consistency food VFSS, mixed consistency (dual consistency) VFSS was performed. Mixed consistency VFSS was done using 4 g of steamed rice mixed with 4 mL of diluted liquid barium twice at each lateral and anteroposterior position (Fig. 2).
All test procedures were recorded on videotape and the findings were analyzed by two physicians of rehabilitation medicine. We referred to the videofluoroscopic dysphagia scale (VDS) to evaluate the findings of VFSS (8, 9). VDS assesses the following 14 items: lip closure, bolus formation, mastication, apraxia, tongue-to-palate contact, premature bolus loss, oral transit time, triggering of pharyngeal swallow, vallecular residue, laryngeal elevation, pyriform sinus residue, coating of pharyngeal wall, pharyngeal transit time, and aspiration.
The oral transit time (OTT), pharyngeal delay time (PDT), and pharyngeal transit time (PTT) were measured in the single consistency food VFSS using 5 mL of diluted barium.
Ten young subjects without history of stroke or other brain injuries and swallowing difficulty were also recruited as a control group for comparative purposes.
We used an independent t-test to compare OTT, PDT, and PTT of each group, and chi-square test to compare the incidence of abnormal findings between patients with delayed PDT/PTT value versus those with normal PDT/PTT value. P values below 0.05 were considered significant.
RESULTS
A total of 49 patients after stroke and other brain injuries were included in the patient group. The mean (SD) age of the patient group was 61.8 (15.0) yr, and the duration from onset to the date of VFSS was within 60 days in 32 patients and above 60 days in 17 patients. Of the 49 patients, 17 had intracerebral hemorrhage, 16 had cerebral infarction, 10 had traumatic brain injury, and 6 had duplicated types of stroke or other brain injuries. In terms of the location of brain damage, 36 patients had supratentorial lesion, 5 had infratentorial lesion including brain stem, and 8 had lesions on both sides of the tentorium (Table 1).
The mean (SD) age of the control group was 31.9 (3.2) yr. In the mixed consistency food VFSS, a majority (8 of 10 subjects, 80%) of the control group showed good bolus formation during mastication without premature spillage of liquid. Two subjects (20%) of the control group showed premature spillage of liquid during the oral phase (Fig. 3A), but the pharyngeal swallowing reflex was immediately triggered to swallow the liquid component and they continued chewing the solid component in the mixed consistency food VFSS (Fig. 3B). There were no abnormal findings in the pharyngeal phase of swallowing in the control group.
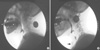
In the patient group, 25 out of 49 patients (51%) showed no abnormal findings in the mixed consistency food VFSS. However, 24 patients (49.0%) showed abnormal findings in the mixed consistency food VFSS, which were categorized in the following ways: 1) posterior spillage of liquid prematurely to pyriform sinus in the oral preparatory phase of swallowing (chewing) of solid component (23 of 49, 46.9%) (Fig. 4A), 2) laryngeal penetration of prematurely spilled liquid in the oral preparatory phase of solid component (6 of 49, 12.2%), 3) subglottic aspiration of prematurely spilled liquid in the oral preparatory phase of swallowing (chewing) of solid component (2 of 49, 4.1%) (Fig. 4B), and 4) significant (more than 10%) residue in valleculae or pyriform sinus (2 of 49, 4.1%). All the patients with laryngeal penetration and subglottic aspiration, and one patient with significant residue in the pyriform sinus showed posterior spillage of liquid prematurely to pyriform sinus in the oral preparatory phase.
There were no statistically significant differences between the control group and the patients group in OTT, PDT, and PTT. However, within the patient group, PDT and PTT showed statistically significant delays in the 24 patients with any abnormal findings in mixed consistency food VFSS compared to the 25 patients without abnormal findings (Table 2). All the patients had normal OTT value (< 1.5 sec). The PDT of all the patients was below 2.0 sec. However, the PDT of 7 patients was above 0.5 sec; 5 of these 7 patients showed posterior spillage of liquid prematurely to pyriform sinus in the oral preparatory phase, 1 patient showed laryngeal penetration, and 1 showed no abnormality. The patients whose PDT value was above 0.5 sec showed a statistically significant incidence of abnormal findings in mixed consistency food VFSS compared to those whose PDT was below 0.5 sec (P < 0.05). The PTT of 9 patients was above 1.0 sec; 7 of these 9 patients showed posterior spillage of liquid prematurely to pyriform sinus in the oral preparatory phase, 1 showed laryngeal penetration, and 1 showed no abnormality. The patients whose PTT value was above 1.0 sec showed a statistically significant incidence of abnormal findings in mixed consistency food VFSS compared to those whose PTT was below 1.0 sec (P < 0.05).
DISCUSSION
Before starting the regular diet composed of foods with different consistencies, we usually conduct VFSS using conventional protocols with single consistency foods; liquid, semi-solid, and solid. However, in this study, we found that nearly half (49.0%) of the patients with no significant abnormalities in single consistency food VFSS showed abnormal findings in mixed consistency food VFSS such as posterior spillage of liquid prematurely to pyriform sinus in the oral preparatory phase of swallowing (chewing) of solid component, laryngeal penetration or subglottic aspiration of prematurely spilled liquid in the oral preparatory phase of swallowing (chewing) of solid component, and significant (more than 10%) residue in valleculae or pyriform sinus. Premature spillage of liquid to the valleculae or pyriform sinus prior to the pharyngeal swallowing is known to be risky because it could cause aspiration before swallowing because a part of the bolus is spilled into the pharynx before the swallowing reflex is triggered, while the airway is still open (10). However, when we eat solid food, premature loss of the chewed bolus to the valleculae during mastication is known to be normal (this is known as 'Stage II transport in the process model of swallowing) (6), because the soft palate seal to the back of the tongue is broken by active tongue movement during the chewing. In our study, 23 patients from the patient group (46.9%) showed posterior spillage of the liquid component of mixed consistency food to pyriform sinus during chewing, possibly because of broken sealing of soft palate to the back of the tongue during chewing, which could increase the risk of penetration or aspiration. All patients with laryngeal penetration or subglottic aspiration in mixed consistency food VFSS had premature spillage of the liquid component. In the control group, premature spillage of liquid during oral preparatory phase was also observed in 2 out of 10 subjects, but the pharyngeal swallowing reflex was immediately triggered to swallow the liquid component and the subjects continued chewing the solid component of the mixed consistency food. From these findings, immediately triggered swallowing of prematurely spilled liquid during chewing of the solid component is considered to be one of the important differences between the control and patient group in mixed consistency food VFSS.
We also observed that in the patient group, 24 patients with any abnormalities in mixed consistency food VFSS showed statistically significant delays in PDT and PTT, compared to 25 patients without abnormal findings (Table 2). The patients with delayed PDT and PTT value showed statistically significant incidence of abnormal findings in mixed consistency food VFSS compared to patients with a normal value of PDT and PTT. The delays in PDT reflect the delayed swallowing reflex or decreased sensation of oropharynx, which could increase the risk of aspiration and penetration after premature spillage of liquid during chewing of solid components in mixed consistency food VFSS (11, 12). Below 0.5 sec was taken as the normal value of PDT for evaluation because PDT prolongation by 0.4 to 0.5 sec in normal subjects over age 60 yr is considered statistically significant in another study (13). As a result, we could anticipate an increased risk of abnormal findings including aspiration and penetration in mixed consistency food VFSS when a patient showed delayed PDT in single consistency food VFSS using liquid.
In a study with a mixture of liquid and solid foods, two-phase food was proposed to increase the risk of aspiration in healthy subjects because the bolus of food reached to lower parts of the pharynx (hypopharynx) than single phase food (which reached to the oropharynx) before the onset of swallowing (5). Another study reported the risk of increased aspiration or penetration of the two-phase mixture food in subjects with dysphagia (14). In our study, we also found that there were significant abnormal findings in mixed consistency food VFSS among patients with stroke or other brain damages who had no overt signs or symptoms of dysphagia and no significant abnormality in single consistency food VFSS. Based on our findings as well as previous studies, we suggest to conduct mixed consistency food VFSS before starting regular diet for patients with stroke or other brain damages to minimize the potential risk of aspiration or penetration.
Nevertheless, this study has several limitations. First, the control group was relatively young. In a follow-up study, we would like to conduct mixed consistency food VFSS for healthy subjects aged over 60 yr. Second, we used 4 g of steamed rice mixed with 4 mL of diluted liquid barium as material for mixed consistency food VFSS because this type of mixture was the most common in regular Korean diets, and this volume was close to that of one scoop of a Korean-style spoon. In the report using two phase food which was done in other countries, they used 4 g of corned beef hash mixed with 5 mL of liquid barium but the reason for using this food or volume combination was not described (5). We tested a maximum of 5 mL of liquid, and the total volume of mixed consistency food was increased to over 5 mL because it is composed of 4 mL of liquid plus 4 g of steamed rice. We cannot exclude that the results of this study were influenced by this increment in the food volume. In further studies, we would like to conduct VFSS using the same volume of liquid compared to the same volume of the mixture of liquid and solid food, and various combinations of mixed consistencies such as liquid and semi-solid or liquid and solid food other than steamed rice.
In conclusion, VFSS protocols using mixed consistency foods detected abnormalities which were not found in the single consistency food VFSS among patients with no overt signs or symptoms. Therefore, we suggest that mixed consistency food should be included in the regular VFSS protocols before starting regular diets for patients suffering from stroke or other brain injuries.





 XML Download
XML Download