

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Vascular access (VA) events including stenosis and thrombosis are major causes of VA failure with hemodialysis (HD). Surveillance of VA is currently recommended because underdialysis due to the vascular access problem can be minimized, and the rate of thrombosis can be reduced (1-3). Vascular access blood flow (VABF) is one of the clinical predictors of stenosis and thrombosis and has been used for surveillance of VA in most HD centers. Previous reports have shown that low VABF (access flow rate less than 600 mL/min in arteriovenous grafts [AVGs] and less than 400 to 500 mL/min in arteriovenous fistulas [AVFs]) is a risk factor for vascular access stenosis and thrombosis (1, 4-6). These reports also indicated that a sequential decrease in VABF (more than 25% over 4 months) can predict VA stenosis and thrombosis (5, 7, 8). In these reports, however, VABF was a short-term predictor of stenosis and thrombosis (almost within 3 months) (4, 5, 7, 9, 10).
The early detection of stenosis and thrombosis and the early correction of lesions have not been clearly demonstrated to prolong VA survival. Tessitore et al. (6) reported that a higher baseline VABF was the only variable associated with a favorable outcome for VA longevity. However, HD patients were enrolled with various VA ages, and the study was not designed to evaluate long-term predictors. In order to evaluate whether early VABF may predict long-term VA patency, we performed a prospective long-term observational study among patients newly started on HD.
MATERIALS AND METHODS
Patient characteristics
A total of 57 patients at the Gachon University Gil Hospital outpatient dialysis center were included. They started HD between January 1, 2005 and December 31, 2007, and all of the patients had de novo VAs. Patients with maturation failure of VA were excluded from the study, as it was impossible to measure VABF using the ultrasound dilution technique. This study was approved by the institutional review board of Gachon University Gil Hospital (#GIRBA 1780). All of the patients were dialyzed with biocompatible membranes (F5 or F6; Fresenius Medical Care AG, Bad Homberg, Germany) three times per week using Fresenius 4008H (Fresenius Medical Care AG).
Vascular access characteristics
All of the permanent de novo VAs were actively used for chronic HD three times per week. The time difference between the VA operation and the first use of VA was at least six weeks in AVFs and at least four weeks in AVGs. Baseline characteristics, including the type of VA and its anatomic location, were collected for all VAs starting HD (Table 1).
Study design
This study was designed as a prospective cohort observational study. VABF was measured with the ultrasound dilution technique (Transonic Systems, Inc., Ithaca, NY, USA) at one month intervals until six months after the VA operation. The measurement was performed within the first half-hour of the dialysis session for each patient at a blood flow rate of 250-300 mL/min (11, 12). Ultrafiltration was turned off 3 min before the start of the measurements in order to avoid the effect of hemoconcentration during the measurements. All patients were monitored for VA events such as VA stenosis and thrombosis. Patients who had physical findings of persistent swelling of the arm, prolonged bleeding after needle withdrawal or altered characteristics of pulse or thrill in the outflow vein also had their VABF measured, and they were referred for angiography if their VABF was less than 600 mL/min in grafts and less than 400 to 500 mL/min in fistulas (1).
Definitions
The endpoint of interest was the development of new VA events at the follow-up examination. VA events included VA stenosis, which was defined as a 50% or greater decrease in luminal diameter, and thrombotic events on fistulography or vascular operation (13). All VAs were monitored for the occurrence of VA events until the last follow-up visit.
Data on the early VABF parameters, which we call the early VABFs, were collected between the first use of VA up to six months after the VA operation. When the VA events occurred within the first six months, data were collected from the first use of the VA to the time of the VA events. The early VABF parameters consisted of the average, minimum, and initial values of early VABF rates, and these were calculated from the early VABFs. The initial value of VABF was defined as the VABF measured at the first use of the VA.
Statistical analyses
The data are presented as medians (interquartile range) for continuous variables and as proportions for categorical variables. Normally distributed data were analyzed with unpaired t-tests; skewed data were analyzed with the Mann-Whitney U test. The early VABF parameters were divided into the lowest quartile and all other quartiles, according to the VA types. The event-free survival based on the early VABF parameters was analyzed using the Kaplan-Meier method and tested using the log-rank test. The hazard ratios between the early VABF parameters and the development of vascular events were determined by univariate Cox-regression analysis. A multivariable Cox-regression analysis then was performed to evaluate the effects of the early VABF parameters, with adjustment for confounding variables. Covariates were assessed at the baseline examination and included gender, age, hypertension, diabetes, vascular access type, hemoglobin levels, body mass index, parathyroid hormone (PTH), and calcium-phosphorus product levels.
The analyses were conducted using SPSS for Windows version 11.0 software (SPSS Inc., Chicago, IL, USA). P<0.05 was considered to be statistically significant.
RESULTS
The baseline demographics are listed in Table 1. The median age of the patients was 54.0 (44.0-63.0) yr, and the proportion of male patients was 44%. The VA types included AVFs in 27 patients and AVGs in 30 patients. About half of the patients had diabetes mellitus, and most of the VAs were located in the left lower arms. Anti-platelet agents were prescribed to most of the patients.
The lowest quartiles of average early VABF rates were 853 mL/min in AVFs and 830 mL/min in AVGs (Table 2). We compared the lowest quartile of average early VABF with the other quartiles according to the VA types (Table 1). There were no significant differences between the lowest quartile group and the other quartile groups in clinical factors such as gender, age, hypertension, diabetes, hemoglobin levels, calciumphosphorus product levels, anti-platelet agents, body mass index, previous catheter history, and location of VA, although the baseline PTH levels were slightly lower in the lowest quartile group with AVF. Two surgeons created all of the VAs in our study. Surgeon A operated from January to July 2005 and Surgeon B operated from August 2005 to December 2007, and there was no significant difference in the proportion of patients in the lowest quartile group and the other quartiles between the two surgeons (P=0.711 in AVF, P=0.847 in AVG). None of the enrolled patients had outflow tract obstruction.
A total of 40 VA events in 23 patients were documented throughout the total observational period (0.404 events/patient-year). During the 20.4±10.6 month observation, six patients were discontinued from follow-up: four patients died, and two patients received renal transplantation. On 15 patients, fistulography was performed for screening VA malfunction. Eleven cases were identified based on the low level of VABF using the ultrasound dilution technique, and four cases were identified from the abnormal physical examination findings. Six cases showed fistulographic stenoses that were located at the anastomic sites or juxta anastomic proximal veins in AVF, and seven cases showed stenoses that were located at the venous anastomic sites or the arterial anastomic sites in AVG. Two cases had mild stenosis (less than 50% in luminal diameter), and had no further intervention. Ten cases of thrombotic events showed abnormal findings such as no thrill and no pulsation of VA, and all of them received thrombectomy. In summary, the new VA events included 13 cases of stenosis, and 10 cases of thrombosis.
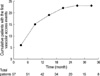
Within 12 months after the VA operation, the number of the new VA events was 15 out of a total of 23 events (65%). The mean time between the VA operation and the new VA events was about 10 months in the 23 patients who experienced the VA events (Fig. 1).
Risk factors for the development of the new vascular access events
We analyzed the unadjusted and adjusted hazard ratios for early VABF parameters associated with the development of the new VA events (Table 3). The lowest quartile of average early VABF (<853 mL/min in AVF, <830 mL/min in AVG) was associated with the development of total VA events after adjustment for gender, age, hypertension, diabetes, vascular access type, hemoglobin levels, body mass index, parathyroid hormone, and calcium-phosphorus product levels (hazard ratio [HR], 3.077; 95% confidence interval [CI], 1.127-8.395; P=0.028). HR for the lowest quartile of minimum early VABF for the risk of VA events was 2.652, but this was not statistically significant. The initial value of VABF was not related to the new VA events. The lowest quartiles of the average and minimum values obtained from the early VABFs were significantly associated with the development of the new VA stenosis after adjustment of covariates. However, the unadjusted and adjusted hazard ratios for all of the parameters associated with the development of the new thrombosis were not statistically significant.
VA patency until the new vascular access events
After the stratification of groups according to VA types, patients with the lowest quartile of average early VABF had worse total VA event-free survival rates than those in the other quartiles (P=0.002). Patients with the lowest quartile of average values had also lower stenosis-free survival probabilities than those in other quartiles (P=0.003) (Fig. 2). However, there was no significant relationship between thrombosis-free survival and the lowest quartile of average early VABF (data not shown).
Total event-free survival and stenosis-free survival were also significantly worse in patients with the lowest quartiles of minimum early VABF (P=0.013 and P=0.011, respectively); this was similar to the results obtained for patients in the lowest quartiles of average early VABF. However, thrombosis-free survival did not show a significant difference between the lowest quartile and other quartiles.
Subgroup analysis in patients with all of the vascular events
Ten patients (4 in AVFs and 6 in AVGs) had 2 or more events, and 4 patients had 3 or more events during the observational period. Six patients had new VA events within 6 months of the VA operation. Vascular access survival could not be analyzed because only 2 patients had vascular access failures.
DISCUSSION
The aim of the study was to evaluate whether early VABF can predict long-term VA patency in incident HD patients. We found that low levels of average and minimum early VABF may increase the risk of the development of total VA events, especially with regard to the new VA stenosis, and can predict poor event-free survival or stenosis-free survival probabilities. Thus, patients with low average or minimum levels of VABF within six months after the VA operation should be monitored more carefully and frequently.
Several reports have shown that a low VABF or a sequential decrease in VABF increases the risk of VA stenosis and thrombosis within a short-term period (1, 4, 5, 7, 9, 10). Previous trials studying the association between VABF and VA longevity enrolled HD patients with a mean VA age of more than 18 months (6). In contrast, our current study enrolled incident HD patients with de novo VAs and evaluated the clinical usefulness of early VABF parameters as long-term predictors of VA stenosis and thrombosis.
VABF measured up to six months after the VA operation was defined as early VABF. Practically, the maturation period is four to six weeks after the operation for AVFs and two or more weeks for AVGs. By our definition, early VABF included three to four values of VABF from every patient because we measured VABF on a monthly basis. These serial data could be more representative of VA patency than a single measurement of VABF. In addition, according to the natural history of VA, the VA patency rates rapidly decrease during the early period, and loss of VA patency occurs at a rate of 25% within 9 months (14). Moist et al. (15) reported that a longer time between graft creation and study enrollment is associated with a decreased risk of graft thrombosis. Thus, VA surveillance should be started right after the first use of the VA, and these early VABFs could have a more important role than VABF values from the late period. This is another reason that we enrolled only patients with de novo VAs.
The average and minimum early VABF values were significant predictors of event-free survival of VAs in our study. The initial VABF parameters displayed a wide range of values and were not useful in predicting the VA events, as the early values of VABF could change after the first use of the VA. The current data demonstrated that early VABF parameters were not significantly associated with VA thrombotic events. In contrast, other reports have shown that a low VABF has also been associated with an increased risk for VA thrombosis (5, 9, 16-18). There are several possible explanations for this discrepancy. First, most of the thrombotic events may follow VA stenoses, and some of the patients with a VA stenosis in our study might have been treated before thrombosis occurred. In addition, anti-platelet agents were prescribed for most of the enrolled patients; this could have reduced the development of thrombosis (15, 19).
There were some limitations to our study. First, the sample size was not large enough to stratify the subgroups. However, we followed up patients for durations that were longer than used in any of the previous clinical trials (4, 7, 10, 17) in order to overcome the effects of a relatively small number of patients. In addition, we enrolled incident HD patients with de novo VAs in order to avoid a lead-time bias. Second, overall VA patency could not be analyzed because there were few VA failures in the enrolled patients. We considered primary patency as the end point, which could be viewed as a surrogate indicator of overall VA patency. A large-scale trial is needed to clarify this potential relationship between early VABF parameters and overall VA survival. Third, several reports revealed that VABF measurement using the ultrasound dilution technique allows non-invasive continuous monitoring of VA and has good accuracy and reproducibility (1, 11, 12, 20-22). However, the ultrasound dilution technique method cannot be used until the patient is using VA for HD; thus we could not evaluate information on VA maturation.
Some reports showed that the early detection of stenosis and thrombosis and the early correction of lesions cannot prolong VA overall survival (1, 2, 23). In contrast, other reports demonstrated that well-programmed regular surveillance not only fosters the ability to detect VA events, but also prevents the morbidity and mortality associated with the failure to detect VA dysfunction (1, 3). We showed that low values of early VABF parameters may predict VA events, especially stenosis in incident hemodialysis patients. This suggests that we should focus on the high risk group with low values of early VABF parameters for effective surveillance of VA patency.
In summary, we found that low values of early VABF parameters were associated with the development of VA events, especially VA stenosis, and poor event-free survival or stenosis-free survival probability. This suggests that some of the VABF parameters in the early period of VA creation may predict long-term VA patency in incident HD patients. These results indicate that some groups of patients with low values of early VABF parameters should be monitored more carefully to prevent VA events.




 XML Download
XML Download