

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Wiskott-Aldrich syndrome (WAS) is an X-linked primary immunodeficiency characterized by a clinical triad of immunodeficiency, thrombocytopenia, and eczema (1, 2). WAS is caused by mutations in the gene encoding Wiskott-Aldrich syndrome protein (WASP) that affect all hematopoietic stem cells including lymphocytes, monocytes, neutrophils and platelets (3). Various WASP gene mutations have been reported in patients with WAS and X-linked thrombocytopenia, a clinically mild allelic variant (4-9).
The treatment of WAS depends on the severity of the immunodeficiency. In severe cases of WAS, the immunodeficiency limits the life expectancy of the patient, and immune reconstitution is the treatment of choice. Imai et al. (10) demonstrated correlations between the clinical phenotype, the extent of the mutation, and the presence or absence of WASP and also recommended hematopoietic stem cell transplantation (HSCT) especially for the patients with WASP-negative WAS. Recently, there have been reports of successful treatment of WAS by unrelated HSCT with cord blood (CB) as well as bone marrow transplant when a matched sibling donor was unavailable (11-16). Although phenotypic corrections for immunologic and hematologic parameters have been reported, genotypic corrections for WAS with cord blood stem cell transplantation (CBSCT) have not been demonstrated.
In this report, we demonstrate 2 cases of WAS which were phenotypically and genotypically corrected with unrelated CBSCT.
CASE REPORT
Patient 1 (UPN 1) is a male who was diagnosed with WAS at the age of 5 months. He presented with incidentally detected thrombocytopenia (23,000/µL) with skin eczema and severe, recurrent otitis media and diarrhea on admission. The second male patient (UPN 2) presented with neonatal thrombocytopenia at birth and received intermittent intravenous immunoglobulin (IVIG). Thereafter he experienced skin eczema and recurrent infections such as cellulitis and pneumonia, until he visited our hospital at 3 months old. Flow cytometric analysis of peripheral blood mononuclear cells (PBMC) for these 2 patients revealed a defect in WASP, leading to the diagnosis of WAS. Subsequently, the nonsense mutations, Arg211stop and Arg13stop, were confirmed by genomic analysis (17). Before transplantation, these patients were treated with monthly infusions of IVIG as well as supportive treatment but there was no clinical improvement.
CBSCT was performed in a laminar air flow room with conventional supportive therapy. The pre-transplantation conditioning regimen for the 2 patients was 1 mg/kg of busulfan intravenously every 6 hr on days -9 through -6. This was followed by 50 mg/kg of intravenous cyclophosphamide on days -5 through -3 and 30 mg/kg of intravenous antithymocyte globulin (ATG) on days -3 through -1. Prophylaxis for acute graft versus host disease (GVHD) included continuous infusion of cyclosporine A beginning on day -1, targeting whole blood levels to be 200 to 400 ng/mL, and 1 mg/kg/dose of methylprednisone every 12 hr on days 5 through 19, and then a taper.
The degree of human leukocyte antigen (HLA) match confirmed by high resolution DNA typing between the infused CB and the patients was 4/6 for UPN 1 and 5/6 for UPN 2. Infused cell doses of TNC and CD34+ cells for UPN1 and UPN2 were 6.24×107/kg and 5.08×107/kg for TNC, respectively, and 1.33×105/kg and 4.8×105/kg for CD34+ cells, respectively.
T-, NK-, and B-cell enumeration and quantitative immunoglobulin studies (for immunoglobulin [Ig] G, A, M, D, and E) were performed. Cytofluorographic analyses of lymphocyte subpopulations were performed with murine monoclonal antibodies conjugated to either fluorescein (FITC) or phycoerythrin (PE) and then analyzed by flow cytometry (FACScan; Becton Dickinson, San Jose, CA, U.S.A.).
Heparinized venous blood samples from patients and family members were fractionated on a Ficoll-Hypaque gradient to isolate PBMCs. For mutational analysis, genomic DNA was extracted from the peripheral lymphocytes, and 12 WASP gene exons were amplified by polymerase chain reaction (PCR) followed by direct sequencing according to the protocol of Sasahara et al. (18).
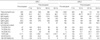
Hematopoietic reconstitution following CBSCT was uneventful, with an absolute neutrophil count (ANC) of more than 500/µL on days 31 and 13 and a platelet count of more than 20,000/µL on days 58 and 50, for UPN 1 and UPN 2, respectively. Molecular chimerism studies using the VNTR method showed a complete donor cell type for these patients (data not shown). Acute GVHD did not occur, even after the infusion of HLA 1 or 2 antigen mismatched CB. UPN 1 experienced 1 episode of sepsis with B. cepacia during the pre-engraftment period without any complications. UPN 2 experienced fever and respiratory distress with hypoxemia due to pulmonary edema as well as skin rashes on the trunk in the pre-engraftment period (from days 8 to days 10), which mimics engraftment syndrome. He recovered with oxygen supply via endotracheal tube and fluid restriction as well as methylprednisone therapy. Both patients were clinically well without eczematous skin and recurrent infections at 60 months (UPN 1) and 55 months (UPN 2) post CBSCT. Clinical data regarding CBSCT are shown in Table 1. The elevated total eosinophil counts and serum IgE levels have been normalized since 7 months post-transplantation in both children (Table 2). Other immunologic parameters including IgG, IgA, IgM, IgD and lymphocyte subsets are summarized at Table 2.
To determine whether the genotype was corrected by CBSCT, we analyzed the WASP gene sequence before and after CBSCT in UPN 1. UPN 1 had a single base substitution (C665T) in exon 7 that results in an amino acid change in codon 211 (Arg211stop) before CBSCT. Following CBSCT, UPN1 had a normal sequence at the mutation site in exon 7 of the WASP gene (Fig. 1).
DISCUSSION
The gene responsible for WAS (WASP) consists of 12 exons with 1,823 bp. WASP encodes a 502 amino acid protein that is expressed selectively in hematopoietic stem cell-derived lineages (4). To date, approximately 100 mutations in the WASP gene have been described. These mutations consist of frameshift mutations, missense mutations, or splice-site mutations, which all give rise to aberrant transcription (4-9). A correlation between clinical phenotype and genotype was reported independently by several investigators (7, 9). Imai et al. (10) observed that patients with missense mutations were WASP-positive, but patients with nonsense mutations, large deletions, small deletions, and small insertions were WASP-negative. Patients with splice anomalies were either WASP-positive or WASP-negative. Lack of WASP expression was associated with susceptibility to bacterial, viral, fungal, and Pneumocystis jiroveci infections and with severe eczema, intestinal hemorrhage, death from intracranial bleeding, and malignancies. They also revealed that the rates for overall survival and event-free survival were significantly lower in WASP-negative patients. Conclusively, they recommended HSCT to improve prognosis, especially for WASP-negative patients.
Recently, HSCT has been the principal modality for correction of immune deficiencies such as WAS. Since CB has been successfully transplanted to reconstitute patients with WAS, as first reported in 1994 (11-16), CB appears to be an alternative donor source compared with matched unrelated bone marrow with successful engraftment associated with no to mild acute GVHD and without development of chronic GVHD. In this study, we identified 2 WAS patients who had nonsense mutations in WASP and we successfully treated them by unrelated CBSCT with engraftment with no associated GVHD.
In CBSCT, the immunologic reconstitution resulted in consistent and stable T-cell, B-cell, and natural killer-cell development. The kinetics of recovery of phenotypic expression and function of the T cells occurred between 60 and 100 days and that of natural killer cells at approximately 180 days (19). The immunologic parameters, especially CD8 of our patients also demonstrated normal values after CBSCT.
Furthermore, following CBSCT, we found that UPN1 had a normal sequence at the mutation site in the exon 7 of WASP gene. While CBSCT has been successfully performed for phenotypic correction including clinical features and immunological parameters in WAS, our study emphasizes the evidence of genetic correction as well as phenotypic correction by CBSCT in WAS. To our knowledge, this is the first report documenting a genetic correction by CBSCT in WAS.
Collectively, our data demonstrate that CBs could be an important source of stem cells for the phenotypic as well as genotypic correction of genetic diseases such as WAS.


 XML Download
XML Download