

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical cancer represents the second most common gynecologic malignancy worldwide. Various molecular and epidemiologic studies have established a strong association between high-risk (HR) human papillomavirus (HPV) genotypes and the development of cervical cancer and its precursor lesions, cervical intraepithelial neoplasia (CIN) 2 or 3 (1-5). The majority of cases of cervical cancer is caused by infection with at least 1 of the 13 accepted HR carcinogenic HPV types (i.e., types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68) (1, 3, 5). Among the carcinogenic HPV types, HPV 16 and HPV 18 account for approximately 70% of all cervical cancers (6). Consequently, it has been proposed that highly sensitive HPV detection methods, such as the HPV DNA test, could enhance the efficacy of population-based screening programs, either as a sole screening tool or as an adjunct to current cervical cytologic screening.
Recently, the detection of HPV infection depends almost entirely on molecular methodologies, of which the Hybrid Capture (HC) 2 assay (Qiagen, Gaithersburg, MD, U.S.A.) is the only commercial HPV DNA test approved by the U.S. Food and Drug Administration (FDA) (7, 8). The HC 2 assay has also been approved in the U.S. as an adjunct to the Papanicolaou test for cervical cancer screening for women aged over 30. While the HC 2 assay can detect 13 HR HPV genotypes, it neither allows the identification of specific genotypes nor provides any information about multiple HPV infections.
Recent studies have provided evidence for a difference in oncogenic potential among the HR HPV genotypes, highlighting the importance of HPV genotyping, particularly HPV 16 and HPV 18 (9). There are numerous polymerase chain reaction (PCR)-based HPV genotyping methods in widespread use. The commercially available PCR-based HPV genotyping methods have included the primer sets, GP5+/GP6+ (10, 11) and MY09/11, and their subsequently modified derivatives PGMY09/11 (12, 13) and the SPF10 system (14-16).
Recently, a novel PCR-based HPV detection and genotyping method has been developed, the HPV 4 Auto-capillary eElectrophoresis (ACE) test (Seegene Inc., Seoul, Korea). In contrast to other commercially available PCR methods, the HPV 4 ACE test uses a newly-developed dual priming oligonucleotide (DPO) system in order to minimize the risk of non-specific priming. This test has the ability to identify HPV 16 and 18 genotypes and can detect 11 other HR HPVs.
In contrast, the PCR HPV Typing Set test (Takara Bio., Shiga, Japan), which is commercially available, uses two primer sets which can detect 7 HR (HPV-16, 18, 31, 33, 35, 52, and 58) and 2 LR HPV genotypes (HPV-6 and 11) (17-20).
The purpose of this study was to evaluate the efficacy of the HPV 4 ACE test, as compared to the HC 2 assay and the PCR HPV Typing Set test for the detection of HR HPV DNA in cervical swab samples. In addition, we compared the HPV 4 ACE test with the PCR HPV Typing Set test for the detection of HPV 16 and HPV 18. Finally, we evaluated the sensitivity and specificity of these HPV DNA tests in correlation with cytologic results.
MATERIALS AND METHODS
Study population and specimen collection
One hundred ninety-nine women who were referred to the Colposcopy Clinic in Guro Hospital of Korea University for abnormal cytology between April and June 2008 were prospectively enrolled. A cervical specimen for liquid-based cytology, along with simultaneous HPV DNA detection by the HC 2 assay, was collected from each woman. Genomic DNA was extracted from each sample and the HPV DNA tests were performed by both the HPV 4 ACE test and the PCR HPV Typing Set test on the same specimen. The study protocol was approved by the Institutional Review Board for Research on Human Subjects at the Korea University Guro Hospital, and written informed consent was obtained from the patients.
Liquid-based cytology
A Cervex-Brush (Rovers Medical Devices, Oss, The Netherlands) was used to obtain samples from the uterine cervix. The brush was immediately rinsed in a vial of PreservCyt solution (Cytyc, Boxborough, MA, U.S.A.). The vial was placed in the Thin Prep Processor (Cytyc). The ThinPrep slide was then fixed in ethanol and stained with Papanicolaou's stain. The number of epithelial cells on these slides was estimated from the number of cells contained within computer-derived coordinates for 50 random fields located within a 20-mm diameter circular area where the cells were deposited. The diagnoses were made using the 2001 Bethesda System for cervical cytology.
HC 2 assay
HPV DNA testing by the HC 2 assay was performed with the HC 2 assay system according to the manufacturer's protocol (Qiagen). The specimens were denatured at 65℃ for 45 min and hybridized under high-stringency conditions with a mixture of RNA probes that detects 13 different oncogenic HPV types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68. The resultant DNA-RNA hybrids were captured on the surface of the microtiter plate wells coated with an anti-DNA-RNA hybrid antibody. The immobilized hybrids were then reacted with an alkaline phosphatase-conjugated anti-hybrid monoclonal antibody. Light intensity was measured with a luminometer. The recommended positivity threshold of 1 pg/mL was used as a cutoff, and all specimens with a relative light unit/control (RLU/CO) ratio of ≥1.0 were considered positive.
HPV 4 ACE test
The residual cell in the PreservCyt solution were centrifuged at 13,000×g for 15 min, and the cell pellets were resuspended in 200 µL of phosphate-buffered saline. The resuspended cell pellets were added to a DNA purification column (Qiagen, Inc., Valencia, CA, U.S.A.). The extraction of total DNA was performed according to the manufacturer's instructions.
Briefly, PCR was conducted in a final reaction volume of 20 µL containing 3 µL of isolated DNA from cervical swab, 4 µL of 5×HPV 4 ACE primer mixture, and 10 µL of 2×Master Mix (Seegene Inc.). The cycling conditions were as follows: denaturation for 15 min at 94℃; amplification for 40 cycles, with denaturation for 30 sec at 94℃; annealing for 1 min 30 sec at 60℃; and extension for 1 min 30 sec at 72℃. The amplified PCR products were separated in 2% agarose gel stained with ethidium bromide or ScreeningTape® System (Lab901 Ltd., Edingurgh, U.K.). Briefly, following PCR, 2 µL of the amplification product was mixed with 6 µL loading buffer (Lab901) in a 0.2 mL PCR Tube. Insert the sample block into the TapeStation (Lab901) and place the 0.2 mL PCR tube containing the sample. Amplicon analysis was then performed on the ScreenTape System with the Seegene View software. Seegene's capillary electrophoresis system provide the detection software which automatically read the PCR product and analyze the amplicon intensity while conventional capillary electrophoresis need user's manual read of the peak with naked eyes after mixing the PCR product with SYBR green or Cyto-9 dye.
PCR HPV Typing Set test
The DNA of swab was extracted from swabs using a QIAamp DNA Micro Kit (Qiagen, Inc.) according to the manufacturer's instructions. The concentration of DNA was measured using a spectrophotometer (DU®530; Beckman, Fullerton, CA, U.S.A.), and the DNA quality was confirmed on agarose gels. The PCR method using the HPV Typing Set was used. The HPV subtype was determined using the HPV Typing Set (Takara Bio., Shiga, Japan), a primer set for PCR specifically designed to identify HPV genotypes 6, 11, 16, 18, 31, 33, 35, 52, and 58 in genomic DNA. The primer HPVpU-31B was used to amplify the DNA of HPV 6 and 11 (LR HPV genotypes) and HPVpU-1M was used to amplify the DNA of HPV 16, 18, 31, 33, 35, 52, and 58 (HR HPV genotypes). The PCR HPV Typing Set method was used according to the manufacturer's instructions. This set includes both malignant and benign control templates for verification of the PCR reaction by using the primer pairs provided in the set. Their expression was normalized using the supplied control template as an endogenous reference. Restriction enzyme digestion of PCR products can also be confirmed because PCR products recognized the sites of Ava II, Afa I, Bgl II, Acc I, and Ava I and small sizes of DNA fragments are yielded by digestion of restriction enzymes. The DNA fragments were confirmed on agarose gels and identified the HPV genotypes.
Statistical analysis
To compare the clinical accuracy of the HC 2 assay, the HPV 4 ACE test, and the PCR HPV typing set test to detect high-grade cervical lesions, we also calculated the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV); the sensitivity and specificity of the three tests were compared by the paired proportion test.
Agreement between the HPV assays was assessed by Cohen's kappa statistic, with values of 0.00-0.20 indicating poor agreement, 0.21-0.40 fair agreement, 0.41-0.60 moderate agreement, 0.61-0.80 substantial agreement, and 0.81-1.00 almost perfect agreement. McNemar's chi-square analysis for matched pair data was performed to analyze contingency tables comparing HPV tests. Statistical analyses were performed with SPSS, version 12.0, statistical software (Chicago, IL, U.S.A.). All tests were two-sided, and a P value <0.05 was considered significant.
RESULTS
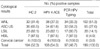
The cytologic findings, as well as all three HPV DNA test results, were available for 199 patients. The overall HR HPV detection rates were 52.3% (104/199) by the HC 2 assay, 54.3% (108/199) by the HPV 4 ACE test, and 48.7% (97/199) by the PCR HPV Typing Set test (Table 1). The HR HPV-positive rates by the HC 2 assay, HPV 4 ACE test, and PCR HPV Typing Set test were 31.4%, 37.3%, and 33.3%, for the normal cytology group, 65.5%, 61.8%, and 58.2% for atypical squamous cells of undetermined significance (ASCUS), 82.1%, 82.1%, and 60.7% for low-grade squamous intraepithelial lesion (LSIL), respectively. In the cytologic high-grade squamous intraepithelial lesion (HSIL) group, which is clinically important for its tendency to progress to cervical cancer, all 3 tests showed identical positivity rates (87.5%), and a 100% HR HPV detection rate was observed in the cervical cancer group by all 3 tests. The HPV 4 ACE test did not show any significant difference in HR HPV positivity in the normal cytology group from the HC 2 assay and the PCR HPV Typing Set test (P=0.143 and P=0.585, respectively). However, there were 17 discordant samples between the HC 2 assay and the HPV 4 ACE test in normal Pap smear samples; 5 samples were HC 2-positive and HPV 4 ACE-negative, and 12 samples were HC 2-negative and HPV 4 ACE-positive. Of 12 samples, 4 included HR HPV genotypes (HPV 16/18, 16/33/58, 16/31, and 52), which were identified by the PCR HPV Typing Set test. In contrast, there were no HR genotypes identified in the former 5 samples. In cytologic ASCUS, the detection rate of the HPV 4 ACE test for HR HPV was also not significantly different from the HC 2 assay and the PCR HPV Typing Set test, but the HC 2 assay showed a significantly higher detection rate for HR HPV than PCR HPV Typing Set test (P=0.02). With the HC 2 assay and the HPV 4 ACE test, a significantly higher percentage of LSIL Pap smear samples tested positive for HR HPV than with the PCR HPV Typing Set test (82.1% vs. 60.7%, P=0.03). In women with cytologic HSIL, the HPV 4 ACE test showed a detection rate of 87.5% for HR HPV, which was the same level as that of both the HC 2 assay and the PCR HPV Typing Set test.
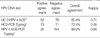
The concordance for HR HPV detection between the HC 2 assay and the HPV 4 ACE test was 85.4%, showing substantial agreement (kappa coefficient=0.71; Table 2). In contrast, the concordance between the HC 2 assay and the PCR HPV Typing Set test was 72.4%, showing moderate agreement (kappa coefficient=0.45). For the detection of HPV 16 and HPV 18, the HPV 4 ACE test and the PCR HPV Typing Set test showed substantial agreement (89.9%, kappa coefficient=0.65). However, 20 cases (10.1%) gave discordant results; specifically, 8 cases were positive by the HPV 4 ACE test, but negative by the PCR HPV Typing Set test, whereas 12 samples were PCR HPV Typing Set test-positive, but HPV 4 ACE-negative (Table 3).
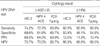
Table 4 shows the HR HPV detection related to cytologic results. The overall HR HPV prevalence increased in parallel with the increasing severity of the Pap smear result. When an abnormal Pap test was defined as ASCUS or higher, the sensitivity and specificity of the HPV 4 ACE test were not inferior to the HC 2 assay (72.2% vs. 74.2% [P=0.40], and 61.8% vs. 68.6% [P=0.27], respectively; Table 4). In addition, the sensitivity and the specificity of the HPV 4 ACE test were also comparable to the PCR HPV Typing Set test (P=0.27 and 0.36, respectively).
When the abnormal Pap test was defined as LSIL or higher, all three HPV DNA tests performed similarly for the detection of HR HPV DNA (data not shown). Furthermore, with respect to cytologic HSIL or cervical cancer, all 3 tests had the same level of sensitivity (92.9%) and a similar level of specificity (Table 4).
DISCUSSION
The purpose of this study was to examine the performance of the novel HPV 4 ACE test for the detection of HR HPV and HPV 16 and 18 genotypes, as compared to the HC 2 assay and the PCR HPV Typing Set test. Since the approval by the U.S. FDA, the HC 2 assay has been used as a gold standard when evaluating the efficacy of the various novel HPV DNA detection methods (21-24). In addition, the PCR HPV Typing Set test has been widely used for the detection of HPV in a number of studies (17-20).
Given that the HPV 4 ACE test has only recently become commercially available, there is no study to compare this test with other HPV detection methods. The HPV 4 ACE test can identify HPV 16 and HPV 18 genotypes among 13 high-risk HPVs and can detect the presence of other 11 high-risk HPVs. For this aspect, the novel HPV 4 ACE test can be called as an upgraded version of the HC 2 assay. Because of the overwhelming importance of the HPV 16 and 18 genotypes in the progression to high-grade cervical lesions, genotyping of the HPV 16 and 18 with simultaneous detection of 11 other high-risk HPVs seem to be very efficacious, as compared to other PCR-based genotyping methods or HPV DNA chip. The HPV 4 ACE test uses a dual priming oligonucleotide (DPO) system that is structurally and functionally different from the primer system currently in widespread use. The conventional priming system is based on a single priming event between the primer and template, which often leads to extension of non-specific products. In contrast, the DPO system has two separate primer segments (a 5'-segment 18-25nt in length and a 3'-segment 6-12nt in length). This unequal distribution of nucleotides leads to different annealing preferences for each segment. The longer 5'-segment preferentially binds to the template DNA and initiates stable annealing, whereas the short 3'-segment selectively binds to its target site and blocks non-specific annealing (25).
In the present study, the HPV 4 ACE test showed the same or comparable levels of the HR HPV detection rate, as compared to the HC 2 assay and the PCR HPV Typing Set test. In addition, the HPV 4 ACE test revealed substantial agreement with the HC 2 assay for the detection of 13 HR HPVs. In contrast, the PCR HPV Typing Set test showed a lower concordance level than the HPV 4 ACE test with the HC 2 assay, which might be partially attributed to the differences in the number of HR HPVs that could be detected by both tests. The PCR HPV Typing Set test can only detect 7 HR HPVs, whereas 13 types can be detected by the HC 2 assay. Furthermore, in terms of HPV genotyping, particularly the HPV 16 and HPV 18 genotypes, the HPV 4 ACE test also showed substantial agreement with the PCR HPV Typing Set test. As shown in Table 3, 20 samples were discordant between the HPV 4 ACE test and the PCR HPV Typing Set test. Although the HPV 4 ACE test failed to detect HPV 16 or HPV 18 in 12 of 20 samples, there were only 2 samples negative for any HR HPV. Furthermore, these two cases were shown to be 1 normal and 1 ASCUS in cytology, not squamous intraepithelial lesions.
A recent study reported by Sandri et al. (21) compared the AMPLICOR HPV test with the HC 2 assay for the detection of 13 HR HPVs. The AMPLCOR HPV test is similar to the HPV 4 ACE test in terms of PCR-based HPV detection methods. In their study, the HR HPV DNA detection rate of the AMPLICOR HPV test was higher than the HC 2 assay in normal Pap smear samples, whereas the two tests performed similarly on abnormal Pap smear results. In contrast, our study showed no significant difference between the two tests for HR HPV DNA positivity, regardless of cytologic results.
Another study performed by Stevens et al. (22) evaluated the performance of the HC 2 assay and the AMPLICOR HPV test according to cytologic results. In cytologic HSIL or higher, the sensitivity of the HC 2 assay and the AMPLICOR HPV test were 87.4% and 95.2%, respectively, which was similar to our results. When compared to another PCR-based HPV DNA detection method already in use, such as the AMPLICOR test, the novel HPV 4 ACE test showed comparable sensitivity for the detection of HR HPV.
With respect to the PCR HPV Typing Set test, Fujinaga et al. (18) evaluated the performance of this test in 39 cervical carcinoma tissue specimens. According to their report, the overall prevalence of HR HPV was 84.6%, of which there were 19 HPV 16-positive specimens and 5 HPV 18-positive specimens. In our study, although evaluated in cytology samples, the HR HPV detection rate was 100% in 6 cervical cancers. Among 6 samples, 4 HPV 16-positive and 1 HPV 18-positive samples were identified.
Our study had some limitations. First, the number of samples with cytologic LSIL or higher were not sufficient to conclude our results. Second, we could not evaluate the performance of HPV DNA tests using tissue samples due to loss of follow-up. For that reason, we evaluated the sensitivity and specificity of the three HPV tests using cytology specimens in three different conditions, that is the "disease" was defined as; 1) ASC-US or worse, 2) LSIL or worse, and 3) HSIL or worse.
Nevertheless, our study showed that the novel HPV 4 ACE test can substitute for the various HPV DNA tests already in use, particularly the HC 2 assay. The HPV 4 ACE test is basically the same test as HC2 assay in terms of detecting 13 high-risk HPVs. But the difference between the two tests is that HPV 4 ACE test can give the information about the presence of HPV 16 and 18 genotypes, which account for about 70% of cervical cancer. So we can not only detect other 11 high-risk HPVs but also genotype the HPV 16 and 18 simultaneously by performing the HPV 4 ACE test. This is very important difference in that knowledge about the presence of HPV 16 and 18 would be helpful to triage the patients who are needed to get frequent follow-up or not. Furthermore, in the era of HPV vaccination, information regarding specific carcinogenic HPV genotypes identified by HPV DNA tests, such as the HC 2 assay in women positive for HR HPV, would be helpful for discriminating women with clinically-relevant diseases that are most likely to progress from those with diseases that regress spontaneously. In addition, persistent infection with HR HPV genotypes, such as HPV 16 and HPV 18, is known to be a necessary condition for the development of high-grade cervical intraepithelial neoplasia and invasive disease (26). Therefore, selective HPV genotyping for HR HPV genotypes would be crucial for distinguishing women who are at high risk for progression from those who are likely to regress.
Thus, the HPV 4 ACE test has the ability to detect the presence of 13 HR HPVs and also to identify HPV 16 and HPV 18 genotypes simultaneously in high concordance with the HC 2 assay. To make this novel diagnostic tool more credible, further studies with larger samples and comparison with other various HPV DNA genotyping methods is needed.

 XML Download
XML Download