

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Idiopathic inflammatory myopathies (IIM) have classical clinical manifestations of muscle weakness related to chronic inflammation in skeletal and systemic inflammation in other organs, including the skin, joints, lungs, gastrointestinal tract, and heart. On the basis of muscular symptoms, skin rash, and histopathological features, different subgroups have been identified with dermatomyositis (DM), polymyositis (PM), and inclusion body myositis.1 IIM are believed to be very rare, and their epidemiologic features have been poorly studied. A recent systematic literature review found that the incidence of IIM ranged from 1.16 to 19 incident cases/million/year and the prevalence from 2.4 to 33.8/100,000 persons.2 The average onset age of IIM patients varies from 44.2 to 55.1 years, and women are dominant.234 The prevalence of DM increases significantly with geographical latitude from northern Europe to southern Europe,5 highlighting the potential role of environmental factors in disease development. The wide reported ranges in epidemiologic studies may be related to genetic and environmental factors, but the relationships are not well defined. In addition, there may also be differences in database, study design, heterogeneity in case ascertainment, and methodology. Therefore, an epidemiologic study of these rare diseases using a large population database is essential to identify geographical and population-based disparities and offer clues to disease characteristics and etiology.
Identification of the exact prevalence of IIM provides information on the disease burden based not only on number of patients, but also on comorbidities. The impact of comorbidities on disease outcome and prevalence has been well evaluated in other rheumatic diseases, especially rheumatoid arthritis (RA).67 IIM is considered to be associated with severe comorbidity, primarily related to muscle weakness and various systemic organ involvement, as well as increased mortality.891011 However, little is known about comorbidities related to IIM.
Therefore, we aimed to estimate the prevalence and incidence of IIM in Korea from 2006 to 2015 and to describe comorbidities in patients with IIM.
METHODS
Data source
Korean National Health Insurance Service (NHIS) database
The entire Korean population in 2015 was 49,705,663 people. All people in Korea are eligible for coverage under the National Health Insurance Program. Therefore, a total number of 47 million, or over 96.3% of the total population, was included in the NHIS database.12 The NHIS database contains individual beneficiary information, in addition to healthcare service information such as diagnosis, procedures, prescriptions, and tests. We used the NHIS database between January 2004 and December 2015.
Study population and covariates
Definition of IIM
The case definition required more than one visit based on the myositis International Classification of Disease-tenth (ICD-10) diagnostic codes of M330, M331 or M339, M332, and registration with the national rare intractable disease supporting program. Patients who suffer from rare incurable diseases can be registered to the Individual Copayment Beneficiaries Program (ICBP) to reduce their burden of medical expenses.13 Application to this program for DM and PM requires a thorough clinical and laboratory survey that fulfills the diagnostic criteria proposed by Bohan and Peter.1415 Patients' selection flow presented in the Supplementary Fig. 1.
Sub-diagnosis was classified as juvenile dermatomyositis (JDM, M330), DM (M331 or M339), and PM (M332). For patients with more than two different diagnostic codes of IIM at different visits, sub-diagnosis was set by prioritizing the diagnostic code first registered to the ICBP. Adult patients aged more than 18 years with a JDM code were classified with the adult diagnostic code (DM or PM) from the closest visit date. However, adult patients with the JDM code applied continuously was classified with JDM. Juvenile patients aged less than 18 years were classified as JDM to avoid underestimation of juvenile myositis.
Prevalence and incidence
Prevalence cases were evaluated for each year between 2006 and 2015. To identify incident cases, patients without any diagnostic code or ICBP code for IIM for 24 months before the index date in each year were extracted. Patients older than 18 years with JDM were excluded for detection of incidence cases, because they may have previously been diagnosed with JDM but be in clinical remission.
Comorbidities
Comorbidities were detected based on the Elixhauser comorbidity index16 and calculated by ICD-10 codes within one year preceding the IIM index date in 2015 prevalent cases. In addition, pulmonary diseases such as interstitial lung disease, pneumothorax, pneumomediastinum, and acute myocardial infarction were also detected based on ICD-10 codes.
Statistical analysis
The overall prevalence per 100,000 persons and incidence per 1,000,000 persons between 2006 and 2015 were estimated. The year-specific mid-year population from the same year provided by the Korean National Statistics Office was used to calculate the prevalence and incidence of IIM. Categorical variables are presented as frequency and percentage, and continuous variables are presented as mean with standard deviation (SD) or median with interquartile ranges (IQR). All analyses were performed using SAS 9.2 (SAS Institute, Cary, NC, USA).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Hanyang University Medical Center and was exempt from an IRB review because we used existing, publicly available data and the information of the subjects could not be identified directly or through identifiers linked to the subjects (IRB No. HYUH 2017-09-009). Informed consent was waived because we utilized a de-identified database which was opened to the public.
RESULTS
Prevalence and incidence rate of IIM patients
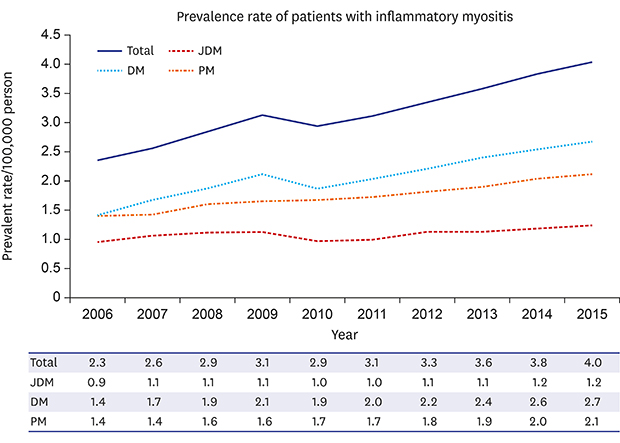
Prevalence was estimated at 2.3–4.0 (0.9–1.2 for JDM, 1.4–2.7 for DM, 1.4–2.1 for PM)/100,000 persons (Fig. 1). We identified 1,150 prevalent cases of IIM in 2006 and 2100 cases in 2015. The mean age (± SD) of prevalent patients with IIM was 51.2 (± 16.9) years, and 72.1% were women. Most (82.4%) visited tertiary or general hospitals, with 74.5% of patients visiting internal medicine departments and 11.1% of patients visiting neurology departments. Among DM patients, 83.6% frequently visited internal medicine, 4.8% visited neurology, and 4.5% visited dermatology, while 70.9% of PM patients frequently visited internal medicine and 20.5% visited neurology. About 10% of patients with IIM visited an emergency room once per year, and 9.6% experienced hospitalizations three or more times per year (Table 1). Health care utilization was not different between DM and PM.
Fig. 1
Prevalence trends between 2006 and 2015 in patients with inflammatory myositis.
JDM = juvenile dermatomyositis, PM = polymyositis, DM = dermatomyositis.

Table 1
Characteristics of prevalent patients with inflammatory myositis in 2015

We identified 218 incident cases of IIM in 2006 and 191 cases in 2015 (Fig. 2A). Incidence rates were estimated at 2.9–5.2 (0.7–1.9 for JDM, 1.8–4.0 for DM, 1.6–3.0 for PM)/1,000,000 person-year. The trend of IIM incidence rates did not appear to increase significantly over a period of 10 years (Fig. 2B).

Comorbidities of IIM patients
In 2015, the median with IQR of the Elixhauser comorbidity index was 3 (2, 5) in PM, and 2 (1, 4) in DM. More than two-thirds of patients (70.7%) had more than two comorbidities. Chronic pulmonary disease and uncomplicated hypertension were common among IIM patients, with prevalence rates of 34.1% and 27.1%, respectively, followed by peptic ulcer disease at 21.8%. In all sub-diagnosis, chronic pulmonary diseases were the most common comorbidity (Fig. 3). Uncomplicated hypertension, peptic ulcer disease, and liver diseases were followed in patients with DM, or PM. However, anemia was more common than liver disease and peptic ulcer disease in JDM.
Fig. 3
Percentage of comorbidities of prevalent patients with inflammatory myositis in 2015.
AIDS/HIV = acquired immune deficiency syndrome/human immunodeficiency virus.

The percentage of patients with ILD was 20.0% in IIM patients and was similar in DM and PM. However, pneumothorax (0.6% in DM vs. 0.4% in PM) and pneumomediastinum (0.8% in only DM) were more frequent in DM (Table 2). The percentage of patients with acute myocardial infarction was 1.9% in DM and 3.0% in PM.
Table 2
Comorbidities of prevalent patients with inflammatory myositis according to sub-diagnosis in 2015

DISCUSSION
Using a nationwide population-based database that included most of the Korean population, we estimated an overall IIM prevalence rate of 2.3–4.4/100,000 persons and an incidence of 2.9–5.2 per 1,000,000. We did not observe any trends in incidence over a 10-year period.
Our calculated prevalence and incidence were lower than those reported in a recent study from Sweden between 2007 and 2011 (prevalence of 14/100,000 and incidence of 11/1,000,000) and a meta-analysis of prevalence (14/100,000 between 1982 and 2010 and incidence 7.98/1,000,000 between 1951 and 2010). In comparison with the data from other Asian populations, our prevalence was similar to that of Taiwan at 2.9/100,00017 and lower than the reported Japanese prevalence of 13.2/100,000 using a registration system from an intractable diseases database.18 These findings revealed no similarities in geographic or ethnicity in our prevalence result. Rather, our prevalence was similar to a previous US prevalence of 5.5/100,000 from hospital records review data,19 Israel incidence of 2.18/1,000,000 from general hospital record review,20 and Japanese prevalence of 2.4/100,000 from enquiries sent to practitioner offices and hospitals.21 The variability in prevalence and incidence estimates was attributed to possible methodologic differences in a recent systematic review report.2 The highest estimates are noted in register-based studies where cases are defined using administrative codes,222324 thus potentially overestimating the true incidence or prevalence. The lowest estimates are found in studies where cases are defined using classification criteria and biopsy findings,252627 thus potentially underestimating the true incidence/prevalence. Our database using the ICBP registration system may have included patients diagnosed definitely by specialists, although the source was claims data.
Several previous studies from the US report a significant increase in the incidence rate of overall IIM over time. The incidence rate increased from the first 11-year period (2.6/million/year) to the second 11-year period (6.5/million/year) from 1947 to 1968 in one study26 and from 2.5 for 1963–1972 to 8.9/million/year for 1973–1982 in another.19 These trends likely reflect improvements in medical record indexing, increased awareness of physicians with community experience over time, and improved diagnostic tools.2 In Korea, the ICBP system for rare incurable diseases was started in 2004. The gradual increase of incidence by 2009 might reflect the effect of promoting the system. Some prevalent patients could be newly registered to this system, which might cause a slight overestimation of incidence. However, there was no increasing tendency over a 10-year period. Further long term follow-up investigation will be needed.
About 88% of patients with IIM had more than one comorbidity. Chronic pulmonary disease was the most common in all types of IIM, with a higher prevalence (20.0%) compared to in RA (11.6%), as reported in Korean claims data.28 We presented the prevalence of various comorbidities using the Elixhauser score, which was more recently developed.16 This score includes more conditions and is becoming more widely used as recent comparisons suggest that it outperforms the Charlson comorbidity index with use of administrative claims data.29
A key strength of the present study is that it is a large, population-based study using a nationwide database. Furthermore, the national registration system for rare and intractable diseases allowed identification of patients who met the classification criteria for IIM. Because IIM is an extremely rare condition, a larger study population increases the reliability of both incidence and prevalence rates. In addition, an understanding of the prevalence of comorbidities in IIM can facilitate estimation of disease burden and severity.
There were several limitations to this population-based study. First, our case definition may have missed patients with mild symptoms who did not meet classification criteria. Second, we could not conclude whether there was an increase or decrease in trends over time in incidence of IIM because it is very rare disease, and trends could be affected by the starting point of the national registration system for rare diseases in Korea. Going forward, we could update the trends using more long term data. Third, misclassification of sub-diagnoses is possible, and amyopathic DM and inclusion body myositis were not identified in our study due to the lack of specific diagnostic codes. If inclusion body myositis could be added as one of the specific rare diseases in our registration system, we could estimate its prevalence. Fourth, we did not determine the cardiac comorbidities, which have the high mortalities in the patients with IIM, because several cardiac diseases such as myocarditis and pericarditis can be asymptomatic and may not be assigned the appropriate diagnostic codes.
In conclusion, our study observed a slightly lower prevalence and incidence of IIM in Korea compared to recent reports from other countries. More than two-thirds of patients had more than two comorbidities.
 XML Download
XML Download