

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Trichophyton tonsurans is an anthropophilic dermatophyte, responsible for infections of the scalp and sometimes of the glabrous skin or nails. Unlike dermatophytosis caused by other dermatophytes, the clinical features of infection due to T. tonsurans are not very apparent initially. Tinea corporis due to T. tonsurans appears as small, erythematous, scaly plaques, often measuring only 1–2 cm in diameter, have no central clearing, and are similar in appearance to eczema. Tinea capitis due to T. tonsurans can be subdivided into three types: the seborrheic subtype, which is primarily characterized by the presence of dandruff and crusts; the kerion celsi subtype; and the black dot subtype. Epidemiological data regarding T. tonsurans infections have emerged from different studies and countries (1234). Infection due to T. tonsurans is common in Mexico, in other countries of Latin America, and in large cities in the United States. By contrast, such infections are rare in Korea; in addition, since its first diagnosis in Korea in 1995, a small number of cases have been found. In 1995, South Korean gladiators were reported to be infected with T. tonsurans during international competitions (1). Since 2000, infections due to T. tonsurans have spread to non-gladiators. Moreover, cases of intrafamilial infections have been reported in the Korean dermatological literature (2). This study aimed to investigate the epidemiological characteristics of infections due to T. tonsurans in Korea.
MATERIALS AND METHODS
Patients
The epidemiological and mycological characteristics of 77 patients diagnosed with T. tonsurans were retrospectively investigated by examining the medical records obtained from the Catholic skin disease clinic between 2004 and 2014.
Methods
The medical records were used to evaluate the annual prevalence and patients’ distribution according to age, sex, season, site, and infection mode. Patients were divided into three groups: gladiators, intrafamilial infection among non-gladiators, and non-gladiators. In addition, microscopic examination using a 15% KOH solution had been performed in all patients. Diagnosis of infections due to T. tonsurans had been confirmed using fungal culture in potato dextrose agar corn meal Tween 80 media. The culture media were maintained at 24–26℃ and examined after 1 to 2 weeks. The patients with T. tonsurans-positive cultures were enrolled in this study. Furthermore, microscopic examination with lactophenol cotton blue stain was performed to identify filamentous fungi.
RESULTS
Prevalence of infection due to T. tonsurans
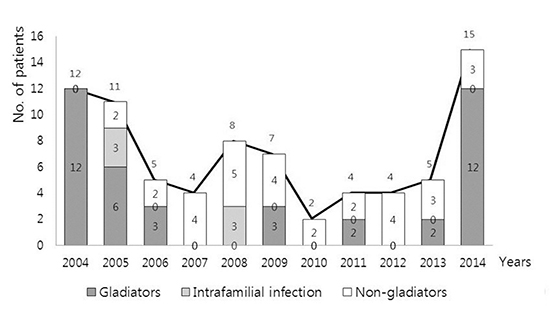
The annual number of patients infected with T. tonsurans was the lowest in 2010 (2 cases, 2.6%) and the highest in 2014 (15 cases, 19.5%). Infections due to T. tonsurans still occurred in Korea until quite recently. Gladiators, including wrestlers, judoists, and Ssireum players (Korean traditional wrestlers), showed the highest incidence in both 2004 and 2014 whereas the prevalence in non-gladiators and intrafamilial infection remained constant during this period (Fig. 1A). The proportion of T. tonsurans infection in dermatophytosis was maintained steadily (0.02%-0.07%), but in 2014, the proportion was increased (0.12%) (Fig. 1B).

Distribution of infection according to sex and age
Of the77 patients, 58 were men and 19 were women (ratio of 1:0.3). The mean age was 19.3 years among the total population, 17.3 years among male patients and 25.3 years among female patients. Fifty-five patients were teenagers (71.4%) (Fig. 2). Gladiators were in the age group 10–20 years (Table 1). Approximately 50% of the patients among the non-gladiators and intrafamilial infection were in the age group 10–20 years.

Seasonal distribution
A total of 27 cases (35.1%) occurred in the spring, representing the highest incidence compared with the other seasons, followed by 26 cases (33.8%) in the winter, 15 cases (19.5%) in the fall, and 9 cases (11.7%) in the summer. The incidence of infections due to T. tonsurans among gladiators was the highest in the spring compared with other seasons, conversely, among the non-gladiators and intrafamilial group, the incidence was the highest in the winter (Fig. 3).

Topographical distribution
The most common site of infection due to T. tonsurans was the face (Fig. 4A). Of the 77 patients, 20 cases (25.9%) had infections of the face. The scalp and arms were the second most common sites of infection, followed by the arms, neck, back, and chest. The number of cases of infection due to T. tonsurans was 13 cases (16.9%) on the scalp, 13 cases (16.9%) on the arms, 11 cases (14.3%) on the neck, 7 cases (9.1%) on the back, and 4 cases (5.2%) on the chest. The legs, feet, hands, nail, and hip were less common sites of infection due to T. tonsurans. Only 9 cases had infections in the legs, feet, hands, nail, and hip, accounting for 11.7% of the cases. Tinea corporis was the most common subtype of dermatophytosis caused by T. tonsurans (Fig. 4B). Thirty-eight cases (49.4%) involved tinea corporis, including infections of the neck, chest, back, arms, and legs. The second most common subtype was tinea facieii, with 20 cases (25.9%). The third most common subtype was tinea capitis, with 13 cases (16.9%). Only 3 cases involved tinea pedis or tinea unguium (3.9%). The most common subtype among gladiators infected with T. tonsurans was tinea corporis, followed by tinea capitis and tinea facieii (Fig. 4B). In tinea corporis of gladiators by T. tonsurans, 9 cases (34.6%) were infected on the arm, 8 cases (30.8%) on the neck, and 4 cases (15.4%) on the back, but in non-gladiators and intrafamilial infection, 5 cases (35.7%) on the back, 3 cases (21.4%) on the arm and neck.

Analysis of infection mode
Of the 77 patients, 40 cases (51.9%) were gladiators, including wrestlers, judoists, or Ssireum players (Fig. 5). They were infected through contact during combat sports events. Seven cases were developed through intrafamilial infection (9.1%). The remaining 31 cases occurred in non-gladiators (40.3%).
DISCUSSION
The incidence of infection due to T. tonsurans differs among countries (3456) and such infections were not reported in Korea before the 1990s. Since the first report in 1995, this organism has also been observed in gladiators in Korea, including wrestlers, judoists, and Ssireum players. Suh et al. (1) reported the first case of the black dot subtype of tinea capitis caused by T. tonsurans in a middle school wrestler. Subsequently, Choi et al. (7) reported three cases of kerion celsi caused by T. tonsurans in high school wrestlers in 1998. Sung et al. (8) reported eight cases of infection due to T. tonsurans both wrestlers and non-gladiators. This is the first report of infection due to T. tonsurans in non-gladiators. Of interest, Kim et al. (9) reported one case of tinea corporis caused by T. tonsurans in an American girl living in Korea.
There have been various reports of infections due to T. tonsurans in the Korean dermatological literature. Kim et al. (10) reported one case of kerion celsi caused by T. tonsurans in an 11-year-old boy. Lim et al. (11) reported the cases of 2 boys with kerion celsi caused by T. tonsurans: one in a 16-year-old high school-judoist and the other 7-year-old non-gladiator.
Jun and Kim (12) conducted a large study on the epidemiological, clinical, and mycological characteristics of dermatophytosis in 1,394 Korean amateur wrestlers through a nationwide group examination between July 1995 and April 1996. Infections due to T. tonsurans were detected in 575 (42.5%) wrestlers. The head and neck areas were the preferred sites among the skin lesions. Jun and Choi (13) also performed a large study involving 316 cases of infection due to T. tonsurans in 2004. This same study showed the epidemiological, clinical, and mycological characteristics of the patients infected with T. tonsurans between 1999 and 2000. The majority of their patients (204, 64.6%) were high school judoists, followed by middle school judoists (18.7%), and those attending college or university (16.7%). The scalp was the most common infection site, followed by the upper extremities, including the hands, face, neck, trunk, and legs. Twenty-six patients (8.2%) infected with T. tonsurans had a family history of the disease. Family members including mother, brothers, father, sisters, and aunt were reported to be affected by the disease in decreasing order of frequency. Jun and Chung (14) also reported two cases of infection due to T. tonsurans through intrafamilial transmission. Park et al. (15) evaluated the clinical and epidemiological characteristics of 105 patients infected with T. tonsurans between March 1995 and December 2003, among them, 73 were gladiators, including wrestlers and judoists, and 32 were non-gladiators. The results of KOH wet mount were positive in 87.6% cases. The preferred anatomical sites were the scalp (37 cases), face (37 cases), upper extremities (17 cases), and neck (15 cases), in decreasing order. The number of infections between the sexes was 89 cases in men and 16 cases in women. The mean age was 16.1 years. The most common season was winter (47 cases). In addition, the occurrence of infection among gladiators reached the peak in 1997 but has remained constant since 1995. In contrast, the number of cases in non-gladiators increased gently until 2003.
In our study, 51.9% of the patients infected with T. tonsurans were gladiators, including wrestlers, judoists, and Ssireum players. With regard to seasons, most cases (27 cases) occurred in the spring, followed by the winter, fall, and summer. Because international or domestic competition for combat sports was frequently held in the spring, the prevalence of T. tonsurans infection to gladiators was highest in the season. The most common site of infection due to T. tonsurans was the face, followed by the scalp, arms, neck, back, and chest. Tinea corporis was the most common subtype of dermatophytosis caused by T. tonsurans, followed by tinea facieii and tinea capitis. It is probably explained by frequent physical contact during strenuous exercises like wrestling and judo.
In both Park’s study (15) and our own, teenagers showed the highest prevalence and the face was the most common infection site. However, comparing with Park’s study, our study showed a decrease in tinea capitis and the prevalence of T. tonsurans in non-gladiators was steady.
Large studies on infection due to T. tonsurans reported several interesting cases in the Korean dermatological literature. Lee et al. (16) reported one case of tinea capitis caused by T. tonsurans. Park et al. (17) reported a single case of tinea capitis and two cases of tinea facieii due to T. tonsurans in a family, characterized by intrafamilial infection among a grandfather, grandmother, and grandson. Kim et al. (18) reported a single case of kerion celsi caused by T. tonsurans in a 21-year-old woman. Additionally, Ko et al. (19) reported a single case of kerion celsi caused by T. tonsurans. Oh et al. (20) reported an unusual case of onychomycosis due to T. tonsurans. Kim et al. (2) reported one case of mycosis of the scalp and one case of tinea corporis due to T. tonsurans in the Korean general population.
T. tonsurans is an anthropophilic dermatophyte. Therefore, it is transmitted by contact among humans. Intrafamilial infection and the increased prevalence among gladiators corroborate the contact transmission of T. tonsurans. Infection due to T. tonsurans can occur via contact with contaminated objects such as, combs, clothing, and shavers. At the time of the first report of infection due to T. tonsurans, outbreaks occurred in South Korea. However, such outbreaks were reported only a few times among gladiators, who are frequently exposed to infected patients during international or domestic competitions. The prevalence of infection in non-gladiators has remained constant until recently. It results from the education and environment improvement for prevention of T. tonsurans infection.
Outbreaks of T. tonsurans infection also occurred in Japan. This emphasizes the importance of educational efforts and public awareness campaigns to prevent T. tonsurans infection. To this end, a study was performed within the judoists’ federation of Tokyo from 2008 to 2014. The percentage of judoists with infection of T. tonsurans decreased over that period from approximately 10% to 5% (3).
In the United States, infections due to T. tonsurans are common as a consequence of changing patterns in global travel and immigration. In addition, the infection of T. tonsurans is especially common among individuals with curly hair, pomade users, and those of a lower economic status. However, the modes of dispersal are unclear, though it is associated with homes, schools, and other institutions. Transmission can occur through direct transfer, or through the use of shared resources and facilities such as pillows and couches. T. tonsurans has its persistent nature in indoor environments and its ability to be transmitted through asymptomatic carriers.
On the contrary to the US, there is low prevalence of T. tonsurans infection in our country. Although there is a low occurrence of outbreaks due to T. tonsurans in South Korea, T. tonsurans infection should be monitored carefully in the country.
 XML Download
XML Download