

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatitis A is an infectious disease caused by the hepatitis A virus (HAV), which is transmitted by the fecal-to-oral route, and a one-time infection can provide lifelong immunity (1). The disease typically presents as a mild disease with no overt clinical features in children, but the severity of disease increases with age. It tends to show more severe symptoms such as persistent jaundice and fulminant hepatitis in the elderly and patients with underlying liver diseases (23).
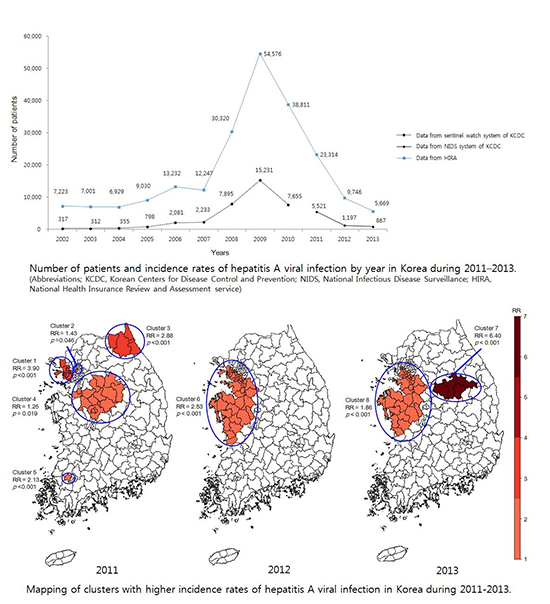
The distribution of hepatitis A is uneven according to geographical region and population group; the epidemiology of hepatitis A is closely related to socioeconomic factors (4). HAV infection is more prevalent in low socioeconomic areas where a lack of sanitation and poor hygiene facilitate spread of the infection. Improvements in sanitation and living standards are contributing to a change in the epidemiology of the viral disease (5); this is the case in Korea. The decrease in HAV infection in young children has resulted in the reduction in the seroprevalence of anti-HAV IgG, with a corresponding increase observed in the adult population (6). As a result, since the 2000s, hepatitis A has taken over from hepatitis B as the leading cause of viral hepatitis in the adult population in Korea (7). In 2009, the incidence of hepatitis A peaked and a total of 15,231 cases were reported to the Korea Centers for Disease Control and Prevention (KCDC). Although the number of reported cases has decreased from 2010 onwards, HAV infection is still poses a great threat to public health.
Considering the importance of HAV infection to public health, the KCDC designated HAV infection a national notifiable infectious disease and, for effective control, is going to add hepatitis A to the national vaccination program for children, beginning May 2015.
The aim of the present study was to describe the current status and regional differences in the incidence rate of hepatitis A in Korea.
MATERIALS AND METHODS
Study setting
HAV was designated a national notifiable infectious disease in 2001 and a surveillance system based on sentinel hospitals was established. Since 2011, the surveillance system has been expanded to every hospital and all HAV infection cases are mandatorily reported by physicians to the KCDC through the National Infectious Diseases Surveillance (NIDS) system. These reported cases have the typical symptoms of acute hepatitis, which include the presence of anti-HAV serum IgM or a positive reverse-transcription polymerase chain reaction result. The data from the NIDS system includes demographic data such as gender, age, and residence of each patient; disease onset; and prognosis. We also used International Classification of Disease B15 (ICD) data from the National Health Insurance Review and Assessment Service (HIRA) to identify the trend of HAV infection from 2002 to 2013. In addition, we used national population data from Statistics Korea for estimating the incidence rates of HAV infection according to age, gender, and administrative district, and investigating the demographic factors associated with regional differences in incidence.
Statistical analysis
The incidence rate of HAV was presented by: years and months; patient age and gender; and county level administrative districts. For estimating incidence rate, we used national statistical data, which stratified the total population by age, gender, and county level administrative districts. The incidence rates were imputed into the biogeographical information system software program DIVA-GIS 7.5 to evaluate the distribution of Hepatitis A by each county. A total of 251 county level administrative districts were used as the spatial unit of analysis. To assess the overall spatial correlation, Moran's index (I) was calculated for the distribution of Hepatitis A incidence rate using the R Statistical Package (Institute for Statistics and Mathematics, Vienna, Austria, v3.1.2, www.R-project.org). Moran's I is a measure which enable the detection of the spatial autocorrelation for a county with its adjacent county. The values range from -1 (indicating perfect dispersion) to +1 (perfect correlation). A zero value indicates a random spatial pattern.
Cluster analysis was performed using the spatial and space-time scan statistic (SaTScan) software, version 9.0 (Martin Kulldorff, Boston, MA, USA), which uses a continuous Poisson model to find hotspot of HAV infection. SaTScan literally scans across the study region with varying sized candidate area (scan window). For each window, the likelihood (here based on Poisson distribution for counts data) is calculated and the candidate area with the maximum likelihood defines the most likely cluster and so on.
RESULTS
Demographic characteristics
Data from the HIRA service revealed that Hepatitis A cases had increased from 2005, reached a peak in 2009, and had then decreased from 2010 over the next 4 yr. A similar pattern was found in data from the KCDC sentinel surveillance system between 2002 and 2010. Hepatitis A incidence have decreased continuously since 2011, the year when the surveillance system was expanded to every hospital. A total of 7,585 cases of HAV infection were reported through NIDS system between 2011 and 2013; 5,521(10.9 cases per 100,000 populations), 1,197 (2.3 cases per 100,000 populations), 867 (1.7 cases per 100,000 populations) cases were reported in 2011, 2012, and 2013 respectively (Fig. 1). Fifty-eight patients were infected outside of the country and 7,527 patients represented autochthonous HAV infection cases. Autochthonous HAV infection occurred more frequently among men than among women (4,619 cases, 6.1 cases per 100,000 population vs. 2,908 cases, 3.9 cases per 100,000 population). The mean patient age was 32.2±9.7 yr. The incidence rate was highest in the 20-29 yr-old group (2,309 cases, 11.6 cases per 100,000 population) and the 30-39 (3,306 cases, 13.6 cases per 100,000 population) yr age groups; they accounted for 88.6% (5,616/7,527) of total cases. Higher incidence rate was shown in the metropolitan area compared to the non-metropolitan area (3,525 cases, 5.1 cases per 100,000 population vs. 4,002 cases, 4.9 cases per 100,000 population) (Table 1). Autochthonous hepatitis A incidence reached a peak in March of each year (14.5%, 1,089/7,527), and the majority of cases were reported from March to June of each year (53.6%, 4,038/7,527) (Fig. 2).
Geographic distribution of HAV
The incidence rates of HAV infection in the various administrative districts of Korea ranged from 0 to 21.9 cases per 100,000 residents. Spatial autocorrelation was significant (Moran's index, 0.62; P<0.01). The incidence rates of HAV infection for each administrative district and the results of the spatial scan statistics are shown in Fig. 3 and Fig. 4. For 2011, five clusters with higher risk for HAV infection were found and the relative risks (RR) were determined as 3.90 in Cluster 1 (P<0.001); 1.43 in Cluster 2 (P=0.046); 2.88 in Cluster 3 (P<0.001); 1.25 in Cluster 4 (P=0.019); and 2.13 in Cluster 5 (P<0.001). One cluster(Cluster 6) was found in 2012 (RR=2.35, P<0.001) and two clusters (Cluster 7 and 8) were found in 2013 (RR=6.40, P<0.001; RR=1.86, P<0.001, respectively). Geographic analyses revealed a consistently high relative risk of HAV infection in mid-western regions (Clusters 4, 6, and 8) (Fig. 4).
DISCUSSION
In this nationwide study of HAV infection in Korea, various analyses including spatial analyses, such as Moran's I and SaTScan, were applied to the nationwide data collected from 2011 to 2013 in order to determine the present epidemiologic status of HAV infection. The data suggested that the prevalence of hepatitis A has been decreasing gradually since 2010 and the population group at risk for acquiring the disease was young males in their twenties or thirties who are living in cluster regions.
Through NIDS system, the KCDC has investigated the number of hepatitis A cases since 2001.The number of reported cases increased sharply until 2009; only 106 cases were reported in 2001, followed by 2,081 cases in 2006, 2,233 cases in 2007, 7,895 cases in 2008, and 15,231 cases in 2009. In 2010, the number of reported cases was 7,655 and with this, the HAV infection incidence rate seemed to take a downward turn despite of the expansion of the surveillance into whole hospitals since 2011.
We also conduct additional analysis with the data from the HIRA in order to reconcile the trend of HAV infection between 2002 and 2013. According to the analysis of data from the HIRA, the number of hepatitis A patients increased continuously until 2009 and decreased rapidly since 2010. This is a similar pattern which is reported in NIDS date in KCDC. However, in the present study, we can find much higher incidences in HIRA data than those in NIDS system. In the HIRA database, a reimbursement claim for HAV diagnosis is made when an examination has been performed because the infection is suspected, and not definitely diagnosed. Therefore, unlike data from NIDS system, data from the HIRA include many suspected cases that lack laboratory confirmation and the number of patients with HAV infection may be overestimated.
Our study showed that young adults aged 20-40 yr old were the age group with the highest risk for symptomatic HAV infection. Previously, hepatitis A had been mostly detected in children under 10 yr of age in Korea (389). However, the number of infections in early age has decreased in accordance with socioeconomic development and this results in a low anti-HAV antibody seroprevalence rate among young adults. Other recent studies in Korea have also shown that the age group most at risk for infection was the 20-40 yr-old age group (378910).
Anti-HAV antibody seroprevalence rates reflect vulnerability to HAV infection in a certain population group; therefore, epidemiologic change patterns can be predicted through the analysis of anti-HAV antibody seroprevalence rate changes. In fact, the seroprevalence data of many Asian countries that have experienced rapid socioeconomic progress coincide with epidemiologic shift patterns (11). In Korea, the rates of seropositivity for the period 1979-1981 were as follows: 46.6% for 1-9 yr-olds; 86.4% for 10-19 yr-olds; 96% for 20-29 yr-olds; and 100% among people >30 yr old (12). In 1989, Lim et al. reported that the anti-HAV seropositivity in Koreans according to age was: 27% for 1-9 yr-olds; 76% for 10-19 yr-olds; and 95.3% for 20-29 yr-olds (13). In 1997, however, Sohn et al. (6) reported that an anti-HAV antibody seroprevalence rate of only 8% was observed among teenagers (10-19 yr old). A study conducted in the Guri city from 2001 to 2013 revealed that the seroprevalence of IgG anti-HAV in the late 2000s had increased compared with the early 2000s: 66% for 1-9 yr-olds; 34% for 10-19 yr-olds; and 18% for 20-29 yr-olds (8). Considering the total sales of HAV vaccine products and the high vaccination rate (about 40%) among children aged 1-2 yr in 2006, the results of the Guri city study seems to be the effect of the vaccination against HAV which began in 1997 (10).
Interestingly, prevalence in males was predominant. The higher prevalence in males has been reported in many of the previous studies not only in Korea (389), but also in many other countries (14151617). However, the exact cause that leads to this difference in gender prevalence is still not known.
The incidence rate of hepatitis A peaked during the months March to June, which is consistent with that reported by previous studies conducted in Korea (79). In Hong Kong, which is located near Korea, a higher hepatitis A incidence was reported during spring to early summer (17). In contrast to this, there were no seasonal differences reported in the studies conducted in Greece and the United States (1819).
Our study has some limitations. First, the analyzed data includes only patients who were diagnosed at health care institutions. Therefore, subclinical cases might not have been counted in this study. Second, the laboratory systems for detecting HAV infection in each hospital were not standardized. We consider this a natural limitation of data collected from multiple institutions. Third, the surveillance system is based on doctor's reporting to KCDC. The spatial disparity of incidence rate might be the result of differing reporting rates by areas. Finally, this study uses population data, and it does not integrate personalized data. Therefore, it does not take into account personal characteristics or dynamic factors such as population movement.
Fortunately, the KCDC is going to initiate a hepatitis A national vaccination program for children beginning May 2015. However, the majority of young adults at present who have not yet experienced HAV infection, and who did not receive a vaccination are still vulnerable to hepatitis A. Therefore, effective HAV control and prevention strategies for young adults, especially young males in their 20s and 30s who are living in cluster regions are also necessary.


 XML Download
XML Download