

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atypical meningiomas (AMs) are reported to account for 20%-35% of all meningiomas; they represent an intermediate subtype between benign and anaplastic meningiomas in the World Health Organization (WHO) classification (1234). Although benign meningiomas are generally slow growing and have a low recurrence rate after gross total resection (GTR) (56), AMs are more locally aggressive and demonstrate more rapid tumor progression. The extant literature suggests: they have a 5-yr recurrence rate of approximately 40% in the absence of postoperative radiotherapy (178). AMs are also associated with significantly increased mortality. Because of their aggressive behavior, AMs have an unpredictable outcome, and reported series have included only a few patients (910). Even after GTR, tumor recurrence is observed after several years in some 20 to 30% of cases (1112). Thus, a reasonable organized therapeutic strategy could be instituted if recurrence could be predicted from surgical specimens, and for this reason many authors have investigated the histological indices of proliferative and apoptotic potential in resected AMs, such as, BCL2 (1314), proliferating cell nuclear antigen (13), and Ki-67 cell cycle-specific nuclear antigen (1516). From these indices, researchers have attempted to establish the nature of the relationship between histological aggressiveness and the recurrence of AMs.
Especially, Apoptotic pathway activation is an important issue related to growth and clinical outcome of tumors. In fact a malfunction of the apoptotic pathways leads to the setting of malignant tumors (1718). Altered expression of anti-apoptotic and pro-apoptotic factors have been frequently associated to recurrence and/or aggressive behavior of meningiomas (1920). Apoptosis is known to follow two different mechanisms: an intrinsic pathway caused by cellular oxidative/metabolic stress and mediated by disarrangement of the mitochondrion and caspase-9 activation, and an extrinsic pathway, triggered by binding of ligands to death receptors that in turn activate caspase-8 (21). Other factors such as BAX pro-apoptotic protein and BCL2 anti-apoptotic protein complete the biochemical intracellular pathways of apoptotic process (2223), that converge on activation of caspase-3 (24). However, there have been no comprehensive studies of posttranscriptional epigenetic regulation (such as histone modification) of these two mechanisms in terms of expression of the anti-apoptotic and pro-apoptotic factors in AMs. The mechanisms of histone modification include the methylation, acetylation, ubiquitylation and etc. Among them histone methylation has been much studied, and several enzymes which are associated with the methylation and demethylation of histone 3 lysine are well defined.
In this study, by immunohistochemically analyzing tumor samples obtained by surgical resection, we aimed to determine the prognostic values of certain pro-apoptotic factors (CASP3, TRAIL-R1, IGFBP, BAX, and XAF1) and anti-apoptotic factors (survivin, ERK, RAF1, BCL2, and MDM2) for predicting the recurrence of AMs after surgical resection. We also estimated the expression of histone 3 lysine methyltransferase (MLL2, RIZ, EZH1, and NDS2) and histone 3 lysine demethylase (KDM5c, JMJD2a, UTX, and JMJD5) in the same way.
MATERIALS AND METHODS
Patient collections
A retrospective case study and clinical review was conducted of the 353 meningioma patients who were treated surgically by either: YZ Kim at Samsung Changwon Hospital and; HD Kim at Dong-A University Medical Center from January 2000 to June 2012. All patients underwent radical surgery and provided a tumor sample for histopathological diagnosis. Among these, we selected tumors that met the diagnostic criteria for AMs that were based on the 2000/2007 WHO classification (25). The following patients were excluded from this study: (1) patients with recurrent atypical meningioma after treatment for previous benign meningioma; (2) patients with multiple intracranial meningiomas, who were excluded due to the difficulty in evaluating treatment response; (3) patients with spinal cord meningioma; (4) patients with preoperative radiotherapy for tumor; and (5) patients with ≤6 months follow-up period due to follow-up loss. The following characteristics were reviewed retrospectively for each patient based on listed information in their medical record: sex, age at the time of surgery, symptoms at diagnosis, tumor location and size, histology grade, the duration of follow up, and recurrence.
Neuroradiological findings of atypical meningiomas
Tumor size was defined by the largest tumor diameter, rounded to the nearest centimeter on gadolinium-enhanced T1-weighted magnetic resonance imaging (MRI) scans before the initial surgery. Peritumoral edema was estimated by the longest distance from the margin of the tumor in fluid attenuation inversion recovery (FLAIR) images. The locations of tumors were divided into two different groups: convexity and non-convexity. Recurrence was defined as the presence of a new tumor in patients with a completely resected tumor, as judged on the first postoperative MRI scan, or evidence of new growth of an incompletely resected tumor on serial postoperative MRI scans as compared to immediate postoperative MRI scans.
All patients underwent preoperative MRI scans. Baseline postoperative MRI scans were also performed immediately after surgery to evaluate the residual mass; follow-up scans were also performed at three or six month intervals in the first two years after surgery. To assess tumor recurrence, serial MRI scans were performed at 1-2 yr intervals in asymptomatic patients; however, if mass-related symptoms or focal neurological signs developed, an MRI scan was performed immediately. Two neuroradiologists (YG Song and HY Lee) at Samsung Changwon Hospital, and one neuroradiologist (SS Choi) at Dong-A University Medical Center, individually conducted radiologic reviews to characterize tumors and determine the presence of recurrence.
Immunohistochemical staining
All tissue specimens were examined for pro-apoptotic factors (CASP3, TRTAIL-R1, IGFBP, BAX, and XAF1), anti-apoptotic factors (Survivin, ERK, RAF1, BCL2, and MDM2), histone methyltransferase (MLL2, RIZ, EZH1, and NSD2), and histone demethylase (KDM5c, JMJD2a, UTX, and JMJD5). For this analysis, the labeled streptavidin-biotin method was performed on sections from paraffin-embedded tissues that were used for pathological diagnoses. The following monoclonal or polyclonal primary antibodies were utilized: CASP3 (1:100, Abcam, UK), TRAIL-R1 (1:100, Life Technology, USA), IGFBP (1:200, Santa Cruz Biotechnology, Germany), BAX (1:100, Santa Cruz Biotechnology), XAF1 (1:100, Santa Cruz Biotechnology), survivin (1:100, Cell Signaling Technology, USA), ERK (1:75, Cell Signaling Technology), RAF1 (1:100, Santa Cruz Biotechnology), BCL2 (1:100, Santa Cruz Biotechnology), MDM2 (1:100, Santa Cruz Biotechnology), MLL2 (1:100, Santa Cruz Biotechnology), RIZ (1:50, Santa Cruz Biotechnology), EZH1 (1:200, Abcam), NSD2 (1:50, Abcam), KDM5c (1:100, Abcam), JMJD2a (1:200, Abcam), UTX (1:100, Santa Cruz Biotechnology), and JMJD5 (1:100, Abcam).
Analysis and interpretation of immunoreactivity
Appropriate positive and negative controls were used throughout the study. Negative controls were obtained by omitting the primary antibody. Sections from normal meninges obtained from autopsy specimens were used as the apoptosis-associated factors and histone modifying enzymes. Ten fields were selected from regions with the highest concentrations of immunopositive nuclei and were examined at high power magnification (×400). Each field corresponded to a total number of cells ranging from 700 to 1,000, in relation with the cellularity of the tumor specimen. Areas of necrosis, normal meningeal cells, and endothelial cells were excluded from the evaluation. On considering 1,000 cells with manual counting, the immunoreactivity of these factors was described as the percentage of immunopositive cells. All slides were reviewed by the two different neuropathologists, EH Lee and DC Kim, who were blinded to patient clinical and radiological information. There was only one discordant case (1.5%) in both reviews of immunoreactivity, and its immunoreactivity was determined after discussion.
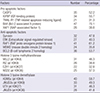
The purpose of analyzing the immunoreactivity of apoptosis-associated factors and histone modifying enzymes in this study was to determine: whether or not these factors have an effect on the recurrence of AMs. Therefore, we performed receiver operating characteristic (ROC) curve analysis on the immunoreactivity of apoptosis-associated factors and histone modifying enzymes to predict the likelihood of recurrence in patients (26). We tried to determine the threshold of immunoreactivity to the highest possible sensitivity and specificity. Through sensitivity-specificity analysis, the cut-off value (the point at which sensitivity and specificity cross) was determined for each factor, as correlated with recurrence (Table 1). In fact, in the autopsy specimen all of the apoptosis-associated factors and histone modifying enzymes were immunohistochemically stained below the cut-off value that we had determined. Therefore, based on the cut-off value for the immunoreactivity of each factor, sequential correlation analysis with the recurrence of AMs was performed.
Statistical analysis
Differences between subgroups were analyzed using Student's t-test for normally distributed continuous values and the Mann-Whitney test for non-normally distributed continuous values. The Chi-square test was used to analyze categorical variables. To define the cut-off value, the performance of each apoptosis-associated factor and histone modifying enzyme as a prognostic factor for the recurrence of AMs was investigated by means of ROC curve analysis and sensitivity-specificity analysis. Recurrence-free survival (RFS) was calculated according to the Kaplan-Meier method, and comparisons between groups were performed using log-rank tests. Variables that were found to be significantly associated with recurrence in AMs in the univariate analyses were then included in multivariate analyses. In multivariate analysis, the Cox proportional hazard regression model was used to assess the independent effects of specific factors on the tumor recurrence rate and to define the hazard ratios for significant covariates. Two-sided P values below 0.05 were considered statistically significant. SPSS version 12.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis.
Ethics statement
The study was approved by the institutional review boards of Samsung Changwon Hospital (2014-SCMC-034-00) and Dong-A Medical Center (13-12-001). The informed consent was obtained from all the subjects if survived or one of family members if died or unconscious for collection of clinical data.
RESULTS
Patient and tumor characteristics
Among a total of 353 meningioma patients, our study ultimately enrolled 67 AM patients (39 female, 28 male). The mean age at diagnosis for these AM patients was 56.6 yr (range, 26.4-87.2 yr). Of the 67 patients, 63 (94.0%) had clinical symptoms before diagnosis. The most frequent chief complaints at presentation were: headache (n=33, 49.3%), seizures (n=13, 19.4%), focal neurological deficit such as motor weakness and dysphasia (n=11, 16.3%), and altered mentation (n=6, 9.0%).
Twenty-nine tumors (43.3%) were located in the convexity regions and 38 tumors (56.7%) in the non-convexity regions. The mean maximal diameter of tumor was 4.38 cm (range, 2.45-8.32 cm), and the mean extent of peritumoral edema was 2.05 cm (range, 0.00-5.54 cm).
Results of immunohistochemical staining
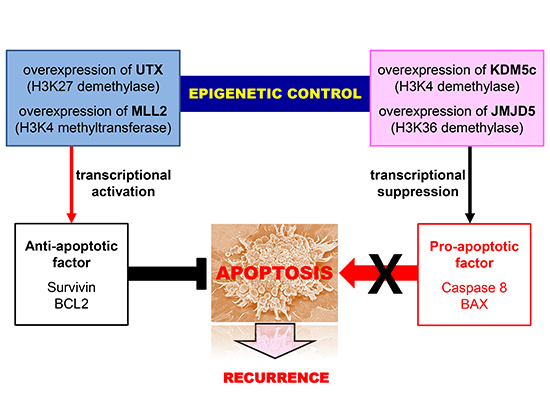
The number and ratio of samples with immunohistochemical overexpression was summarized according to the each factor in Table 2, and several samples with immunohistochemical over- or low expression were also illustrated in Fig. 1. Interestingly, there were several unique patterns of immunohistochemical expression between apoptosis-associated factors and histone modifying enzymes: 1) all the samples that had immunohistochemical overexpression of MLL2 (n=31) also showed immunohistochemical overexpression of UTX (n=31) identically; 2) of the 32 samples with immunohistochemically overexpressed survivin, 30 samples (93.8%) had overexpression of MLL2 and UTX simultaneously, which means that UTX and MLL2 could induce the expression of survivin ; 3) of the 36 samples with immunohistochemically overexpressed BCL2, 31 samples (86.1%) had also overexpression of MLL2 and UTX, which means that UTX and MLL2 could induce the expression of BCL2; 4) of the 20 samples with immunohistochemically low expressed BAX, 19 samples (95.0%) showed overexpression of KDM5c simultaneously, which means that KDM5c could suppress the expression of BAX; 5) of the 31 samples with immunohistochemically low expressed CASP3, 28 samples (90.3%) showed overexpression of JMJD5 simultaneously, which means that JMJD5 could suppress the expression of CASP3 (Fig. 2).
Recurrence and clinical outcome
The mean follow-up time from date of surgical resection was 47.7 months (range, 8.4-132.1 months). During follow-up, 26 patients (38.8%) presented with recurrence; all of which occurred more than one year after surgery. The mean time to recurrence (TTR) was 61.8 months (range 15.6-111.1 months). The actual 5-yr and 10-yr RFS were 67.8% and 28.3%, respectively. All recurrences occurred at the original site of surgery and there was no distant metastasis extracranially.
In terms of the clinical and radiological characteristics, recurrence occurred in 15 (39.5%) of the 38 patients who were <60 yr old, 13 (46.4%) of the 28 female patients, 16 (42.1%) of the 38 patients whose tumor had a non-convexity location, 12 (46.2%) of the 26 patients who had a tumor size of ≥5 cm, 10 (47.6%) of the 21 patients who had a tumor with peritumoral edema ≥3 cm. The TTR was not significantly different according to the above clinical (age, P=0.889; sex, P=0.475) and radiological characteristics (tumor location, P=0.548; maximal tumor size, P=0.462; peritumoral edema, P=0.617) except for the extent of surgical resection (P<0.001).
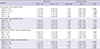
In terms of immunohistochemical staining for pro-apoptotic factors, the recurrence rate was lower, and the TTR was significantly longer, in the patients with overexpression of CASP3 (14.3%, P<0.001), TRAIL-R1 (19.0%, P=0.009) and BAX (21.3%, P=0.006) than those with low expression of these factors. In terms of immunohistochemical staining for anti-apoptotic factors, the recurrence rate was lower and the TTR was significantly longer in the patients with low expression of survivin (22.9%, P=0.002), MDM2 (27.9%, P=0.038), and BCL2 (19.4%, P=0.021) than those with overexpression of these factors. In terms of immunohistochemical staining for histone modifying enzymes, the recurrence rate was lower and the TTR was longer in the patients with low expression of MLL2 (25.0%, P=0.027), UTX (16.7%, P=0.001), and JMJD5 (23.1%, P=0.006) than those with overexpression of these factors. Conversely, the patients with immunohistochemical overexpression of KDM5c had a lower recurrence rate (17.5%) and a longer TTR (83.6±10.4) than those with low expression of this factor (P<0.001) (Table 3).
Univariate analysis of factors predicting recurrence of atypical meningiomas
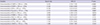
In terms of apoptosis-associated factors, immunohistochemical overexpression of CASP3 (P<0.001), IGFBP (P=0.006), and BAX (P<0.001), and immunohistochemically low expression of survivin (P=0.003), BCL2 (P=0.016), and MDM2 (P<0.001) was associated with recurrence in univariate analysis (Table 4). In terms of histone modifying enzymes, immunohistochemical overexpression of MLL2 (P=0.021), UTX (P<0.001), and JMJD5 (P<0.001), and immunohistochemically low expression of KDM5c (P<0.001) was associated with recurrence in univariate analysis (Table 4). In terms of clinical and radiological characteristics, however, there was no factor predicting recurrence in the univariate analysis.
Multivariate analysis of factors predicting recurrence of atypical meningioma
Multivariate analysis showed that the following factors were independently associated with a recurrence: immunohistochemically low expression of CASP3 (Hazard ratio (HR) of 5.243, P<0.001) and BAX (HR of 6.338, P<0.001), and immunohistochemical overexpression of survivin (HR of 4.415, P=0.007), BCL2 (HR of 3.699, P=0.013) and MDM2 (HR of 2.946, P=0.037) (Table 5). The factors that were associated with recurrence in the univariate analysis, but were not independently associated with a higher rate of recurrence in multivariate analysis, were as follows: immunohistochemically low expression of IGFBP (P=0.064) and KDM5c (P=0.382), and immunohistochemical overexpression of MLL2 (P=0.131), UTX (P=0.316), and JMJD5 (P=0.504) (Table 5). Interestingly, the patterns of immunohistochemical expression of all histone modifying enzymes were not associated with recurrence independently; even though they had an association with recurrence of AMs in univariate analysis.
DISCUSSION
For most of AMs, the conventional strategy of combining both surgery and radiation therapy provides both long-term effectiveness and sufficient clinical results (78). However, some meningiomas recur or are resected subtotally due to their delicate location at skull based structures. Abnormal apoptosis is a hallmark of human meningiomas and deregulation of the genes controlling the apoptotic cascade is closely related to tumor development, progression, and recurrence (1920).
In this study, expectedly certain pro-apoptotic factors (such as CASP3 and BAX) and anti-apoptotic factors (such as survivin, BCL2, and MDM2) were associated with recurrence of AMs. In the apoptotic pathway, caspases are executioner enzymes playing a fundamental role in degradation phase (27). Although there are no comprehensive reports in AMs, in many other tumors, cell transformation is associated with a genetic silencing or alteration of caspase activation process (28). However, the presence of caspase activation cannot be taken as an absolute signal for cell death because caspase inhibitors have been found (29). Tumor cells can survive and proliferate producing more caspase inhibitor factors such as surviving; this has often times been associated to therapy resistance and poor prognosis in tumor clinical outcomings (1930). Survivin, as the most representative caspase inhibitor factors, block apoptosis by interacting with CASP9 activated fragment (31), while another apoptotic inhibitor, c-FLIP, reduces the cleavage of CASP8 and 9 (32). Other factors such as BAX pro-apoptotic protein and BCL2 anti-apoptotic protein complete the biochemical intracellular pathways of apoptotic process (23) that converge on activation of CASP3 (24). In particular, CASP3 was reported to have a lower expression in WHO grade II and III meningioma than WHO grad I meningioma (33). In this study, overexpression of survivin and BCL2 and underexpression CASP3 and BAX were associated with high recurrence rate in AMs, which was concordant with previous reports. Otherwise, there are dissenting reports to this finding that a high expression of CASP3 has been found associated with recurrence in meningioma (1920), which might be due to the use of a fresh specimen instead of archival ones and inclusion of all the grade of meningiomas.
Survivin is known to be expressed in fetal tissue and transformed cells in adults (3435). The expression of survivin not only appears to correlate with aggressive tumor behavior and a poor prognosis, but is also considered a risk factor for resistance to chemotherapy and radiation treatment (36). In the majority of primary nervous system tumors, particularly in glioblastomas and peripheral nerve sheath tumors, survivin is also expressed (30). In glioblastomas, positive survivin expression was seen in immunohistochemistry and detected in high levels throughout the specimens, with a positive correlation to the Ki-67 proliferation index (3738). However, no correlation between the intensity of survivin staining and the clinical course of the tumors has been observed (30). Fortunately, authors found out that the overexpression of survivin should be associated with high rate of recurrence in AMs, just by immunohistochemical analysis.
Histone modification is one of major epigenetic mechanism to regulate the expression of genes, and includes methylation, acetylation, ubiquitylation, and phosphorylation. Methylation of histone residues occurs at the side chains of arginines and lysines. Histone H3 is the primarily methylated at the four lysine residues within N-terminal tail (K4, K9, K27, and K36). Methylation of H3K4 and H3K36 activates the expression of genes, and methylation of H3K9 and H3K27 suppresses the expression of genes. In this study, the overexpression of MLL2 (H3K4 methyltransferase), UTX (H3K27 demethylase), and JMJD5 (H3K36 demethylase), and the underexpression of KDM5c (H4K4 demethylase) showed the short TTR. Additionally, MLL was expressed identically with UTX, which was concordant with previous report by Lee et al (39). Interestingly, presenting study showed that high rate of UTX-MLL complexes were overexpressed in the samples with overexpression of survivin and BCL2, which meant that UTX-MLL complex should activate the expression of survivin and BCL2. Similarly, high rate of KDM5c and JMJD5 were overexpressed in the samples with low expression of BAX and CASP3 respectively, which meant that KDM5c and JMJD5 should suppressed the expression of BAX and CASP3 respectively. Although above four enzymes did not influence on the recurrence of AMs directly, they might regulate the expression of several apoptosis-associated factors (such as CASP3, BAX, survivin, BCL2, and MDM2). As a result, these apoptosis-associated factors had significant association with recurrence of AMs. In fact there are several reports about the oncogenetic role of these histone modifying enzymes; UTX in renal cell carcinoma (40) and myeloid malignancies (41), MLL2 in medulloblastoma (42) and gastric cancer (43), JMJD5 in clear cell renal cell carcinoma (40), KDM5c in breast cancer (44). Recently, UTX and MLL4 was suggested that they should regulate transcriptional programs for cell proliferation and invasiveness in breast cancer cells coordinately (45), and downregulation of MLL3 was suggested that this should be required for the growth and metastasis in esophageal squamous cell carcinoma (46). However, they did not investigate clinical role of these enzymes, neither any role in apoptosis of tumor progression. This is the first study dealing the epigenetic role of histone modifying enzymes in regulating apoptosis of AMs.
Clinically, recurrence rates vary between studies, depending on both the duration of follow-up and the number of patients studied. An analysis of some of these studies has shown that the patient's age at diagnosis (11), complete resection or GTR (4), and postoperative radiotherapy (1147) are invariably associated with lower risks of atypical meningioma recurrence. As regards the extent of resection, which is a significant independent predictive factor of recurrence in atypical meningiomas as well as in meningiomas overall, many authors have reported similar results. As published previously (the data was not presented in this article), the results in the present study–those obtained through Kaplan-Meier survival analysis and the Cox proportional-hazards regression model–correspond well with these findings, suggesting that the most important factor in determining the likelihood of meningioma recurrence is the extent of tumor resection (48). However, in this study, postoperative radiotherapy was not an independent factor predicting the recurrence of atypical meningiomas in the multivariate analysis (Cox proportional-hazards regression model), and it showed only a tendency to predict a recurrence (P=0.058) (48).
In spite of the acquired results, this study has several notable limitations. First, we analyzed the apoptosis-associated factors and histone modifying enzymes only at the protein level using immunohistochemical staining without any examination of DNA and RNA such as Western blotting and quantitative real-time polymerase chain reaction (qRT-PCR) methods. Because these samples were not frozen tissues but archival formalin-fixed paraffin-embedded samples, molecular analysis using DNA was practically impossible. Therefore, a molecular genetic study such as DNA sequencing is essential to show the epigenetic role of histone modifying enzyme to regulate expression of apoptosis-associated factors. Second, we did not examine all the factors in apoptotic pathway; we also did not examine all the histone modifying enzymes. We examined just the 4 histone lysine methyltransferases and 4 demethylases, which we could not examine all the relation between apoptosis-associated factors and histone modifying enzymes. Finally, the retrospective nature of the analysis is the main limitation of this work. We attempted to partially mitigate this bias by extracting patient data from complete medical and radiological records and by recruiting patients who were treated using the same treatment protocol. Despite these efforts, however, the conclusion drawn from our study needs further validation through prospective and randomized clinical trials.
Conclusively, in this study, we investigated the prognostic values of certain apoptosis-associated factors and histone 3 lysine methyltransferases and demethylases for predicting the recurrence of AMs after surgical resection by immunohistochemically analyzing tumor samples obtained by surgical resection. We found that low expression of CASP3 and BAX and overexpression of survivin, BCL2, and MDM2 are associated with the recurrence of AMs. Although histone 3 lysine methyltransferases and demethylases are not shown to have the independent association with recurrence of AMs, among them, MLL2, UTX, JMJD5, and KDM5c should have an influence on time to recurrence and regulate the expression of apoptosis-associated factors. However, as these analyses were performed only at the protein level, molecular genetic study is essential to confirm our results.




 XML Download
XML Download